Article Text

Abstract
Objectives The objectives of this study are to analyse the long-term follow-up of a randomised controlled trial of induction treatment with azathioprine/methylprednisolone (AZA/MP) versus high-dose intravenous cyclophosphamide (ivCY) in patients with proliferative lupus nephritis (LN) and to evaluate the predictive value of clinical, laboratory and renal biopsy parameters regarding renal outcome.
Methods 87 patients with biopsy-proven proliferative LN were treated with either AZA/MP (n=37) or ivCY (n=50), both with oral prednisone. After 2 years, renal biopsy was repeated, and all patients continued with AZA/oral prednisone. The primary study end point was sustained doubling of serum creatinine. Secondary end points included renal relapse, end-stage renal disease and mortality.
Results After a median follow-up of 9.6 years, no significant differences between AZA/MP versus ivCY groups were found in the proportion of patients with sustained doubling of serum creatinine (n=6 (16%) vs n=4 (8%); p=0.313), end-stage renal disease (n=2 (5%) vs n=2 (4%); p=1.000) or mortality (n=6 (16%) vs n=5 (10%); p=0.388). Renal relapses occurred more often in the AZA/MP group (n=14 (38%) vs n=5 (10%); p=0.002, HR: 4.5). Serum creatinine, proteinuria and immunosuppressive treatment regimens at the last follow-up were comparable. Clinical and laboratory parameters at baseline and after 2 years, and renal biopsy parameters (only) at baseline predicted renal outcome.
Conclusion Induction treatment with ivCY was superior to AZA/MP in preventing renal relapses, but other parameters for renal function did not differ. AZA/MP can therefore serve as an alternative in patients with proliferative LN who wish to avoid gonadal toxicity of CY. Several prognostic factors of long-term renal outcome were identified.
Statistics from Altmetric.com
Introduction
Randomised controlled trials (RCTs) at the National Institute of Health have demonstrated that induction treatment with oral or intravenous cyclophosphamide (ivCY) combined with oral prednisone (OP) is effective in preventing end-stage renal disease (ESRD) in proliferative lupus nephritis (LN) compared to prednisone monotherapy.1 2 However, CY use is associated with many side effects, especially gonadal toxicity.3 4 The National Institute of Health data did not allow a conclusion as to whether induction treatment with azathioprine (AZA), a drug with less long-term side effects,5 6 combined with intravenous methylprednisolone (ivMP) could be an alternative for CY.
In the first Dutch Lupus Nephritis Study (enrolled between 1995 and 2001), 87 patients with systemic lupus erythematosus (SLE) with proliferative LN were randomly assigned to either AZA (2 mg/kg/day) combined with ivMP (3×3 pulses of 1000 mg) and OP (initially 20 mg/day) or ivCY (750 mg/m2, 13 pulses in 2 years) combined with OP (initially 1 mg/kg/day). After 2 years, both groups were treated with AZA plus OP. After a median follow-up of 6.4 years, non-sustained doubling of serum creatinine and renal relapses occurred significantly more often in the AZA/MP group. Renal function at the last visit did not differ between both treatment groups.7 However, an extended follow-up is needed to evaluate the long-term effects on renal function.2 8 9 Since the use of non-sustained doubling of serum creatinine has been criticised as a robust primary study end point, we adopted the generally accepted sustained doubling of serum creatinine for the present analysis.10
Identifying prognostic factors for outcome after immunosuppressive treatment is important for optimising treatment strategies in individual patients with LN. Therefore, the predictive value of laboratory and histological parameters at baseline and after 2 years was also studied in the first Dutch Lupus Nephritis Study. Although the increase in chronicity index (CI) was larger in the AZA/MP group compared to the CY group, CI at baseline could not predict renal outcome after the median follow-up of 6.4 years. Furthermore, 2-year repeat renal biopsies did not provide any additional information regarding renal outcome at the last follow-up.7 However, for histological parameters, longer follow-up is necessary to ascertain their prognostic value.
The aims of the present study were to analyse the long-term follow-up data of induction treatment with AZA/MP versus high-dose ivCY in patients with proliferative LN and to evaluate the predictive value of clinical, laboratory and renal biopsy parameters with regard to renal outcome after immunosuppressive treatment in these patients.
Methods
Patients
Between September 1995 and September 2001, 87 patients (86% female, 76% Caucasian) were included in the first Dutch Lupus Nephritis Study. All patients aged between 18 and 60 years fulfilled ≥4 American College of Rheumatology criteria for SLE, had creatinine clearance >25 ml/min (Cockcroft–Gault formula) and had biopsy-proven proliferative LN (WHO class III, IV, Vc or Vd). Patient characteristics and additional inclusion and exclusion criteria have been described previously.7 11 The study was approved by the ethics committees of all participating hospitals, and written informed consent was obtained from all patients.
Treatment
Patients were randomly assigned to the AZA/MP or CY group. Patients in the AZA/MP group (n=37) started with AZA (2 mg/kg/day) at day 1, which was combined with ivMP (1000 mg) for 3 consecutive days. This cycle of three pulses was repeated after 2 and 6 weeks. OP (20 mg/day) was added and was tapered to 10 mg/day after 5 months. Patients in the CY group (n=50) received ivCY (750 mg/m2) every 4 weeks for a total of 6 pulses, followed by 7 pulses every 12 weeks. OP was added (1 mg/kg/day) and was tapered to 10 mg/day after 6 months. After 2 years, treatments were identical in both groups: AZA (2 mg/kg/day) plus OP (10 mg/day). After 4 years, it was advised to taper the dosage of both drugs over a year: first, OP was reduced to 10 mg every other day, and then AZA, to 1 mg/kg/day. The patients were advised to continue this treatment regimen for at least 2 more years. The study had an open-label design.
In case of cytopenia, impaired renal or liver function, AZA/MP or CY treatment was adjusted as described previously.11 Recommendations for treatment of hypertension and hyperlipidemia were given, but the choice of drugs was left to the treating physician. From March 1998, the prescription of angiotensin-converting enzyme (ACE) inhibitors in case of proteinuria >0.5 g/day was compulsory.
Assessments
Patients were evaluated every 4 weeks during the first 6 months and then every 3 months thereafter. After 4 years, physicians asked patients to come back on a regular basis for a follow-up (at least yearly). Serum creatinine, proteinuria, anti-double-stranded DNA antibodies (anti-dsDNA), complement factor 3 (C3) and complement factor 4 (C4) were recorded. Anti-dsDNA positivity was assessed according to local standards. The primary study end point was sustained doubling of serum creatinine, which was defined as doubling of the lowest obtained serum creatinine at any time during follow-up, confirmed on 2 consecutive visits excluding other causes. Secondary end points were treatment failure and renal relapse, ESRD and mortality. Primary treatment failure was defined as doubling of baseline serum creatinine at week 12. Consequently, patients were switched to the other treatment arm. Renal relapses could occur after week 12 and were defined as nephritic flare, which is doubling of the lowest obtained serum creatinine so far, and/or proteinuric flare, which is the development of either a nephrotic syndrome (proteinuria >3.5 g/day) while the lowest protein excretion so far had been repeatedly ≤2.0 g/day or proteinuria >1.5 g/day without other causes in a previously non-proteinuric patient. In case of a renal relapse, induction treatment was repeated. If that course failed or in case of a second renal relapse, patients were switched to the other treatment arm.
Renal biopsy
Renal biopsy samples were obtained from all 87 patients before randomisation for study treatment. After 2 years, repeat renal biopsy samples were obtained (for study purposes only) from 41 patients. Two of these repeat renal biopsies were excluded due to lack of glomeruli. All renal biopsies were reviewed by experienced nephropathologists.7 CI and activity index (AI) were determined.12
Statistical analysis
Statistical analysis based on an intention-to-treat principle was performed with PASW Statistics 18 (SPSS, Chicago, Illinois, USA). χ2 and Fisher's exact tests were used to compare percentages between treatment groups. Kaplan–Meier curves were used to compare the proportion of patients that reached primary or secondary study end points between treatment groups. Hazard ratios (HR) with 95% confidence intervals (95% CI) were calculated using univariate Cox regression. Multilevel analysis was used to compare the course of clinical and laboratory parameters between treatment groups.
Predictor analyses for time to occurrence of sustained doubling of serum creatinine and renal relapse were performed using forward conditional Cox regression of variables with p value ≤0.2 in univariate analysis. Predictor analyses for serum creatinine (log transformed) and proteinuria (square root transformed) at last visit were performed using multivariate linear regression with forward inclusion of variables with p value ≤0.2 in univariate analysis. The last observation carried forward method was used, except for two patients who were lost to follow-up during the first 2 years. The following prognostic factors were tested: induction treatment, gender, ethnicity, age, duration of SLE, LN as a presenting symptom, hypertension (defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, or the use of antihypertensive drugs), serum creatinine, proteinuria, anti-dsDNA positivity, C3, C4, and renal biopsy CI and AI. The probability of F for entry was 0.05. p Values <0.05 were considered statistically significant.
Results
Primary and secondary study end points
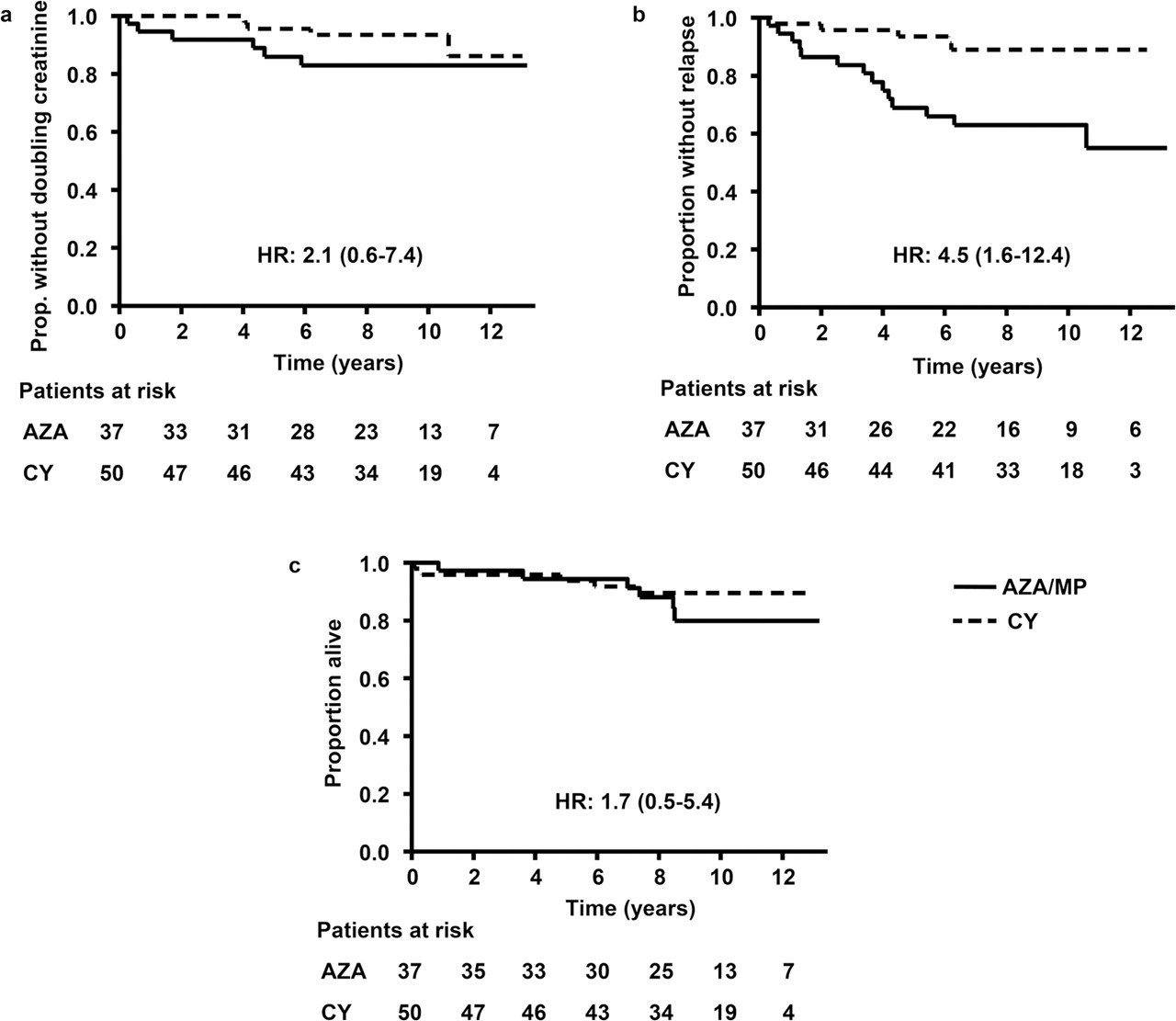
In February 2009, the median follow-up was 9.6 years (range, 0.1–13.2). In total, six (7%) patients were lost to follow-up because of migration (n=3) or of the patient's choice to quit the study (n=3). During follow-up, 10 (11%) patients reached sustained doubling of serum creatinine, and 19 (22%) patients had a renal relapse. Renal relapses consisted of doubling of serum creatinine (nephritic flare) in seven patients, proteinuric flares in 11 patients and a combination of both in one patient (table 1). No significant differences were found between the AZA/MP and CY group in the proportion of patients with sustained doubling of serum creatinine. Renal relapses occurred significantly more often in the AZA/MP group (figure 1), especially proteinuric flares.

The Kaplan–Meier curve showing the proportion of patients: (a) free of sustained doubling of serum creatinine, (b) free of renal relapse and (c) alive; AZA/MP group versus CY group. AZA/MP, azathioprine/methylprednisolone; CY, cyclophosphamide.
Long-term follow-up of the first Dutch Lupus Nephritis Study
During the follow-up, four (5%) patients reached ESRD (AZA/MP (n=2), week 14 and 431; CY (n=2), week 298 and 596). Furthermore, 11 (13%) patients died (table 1). Causes of death were comparable between treatment groups (AZA/MP (n=6): sepsis (week 45 and 442), stroke (week 187 and 363), sudden death (week 383) and cancer (week 440); CY (n=5): heart failure (week 6 and 308), stroke (week 17), sepsis (week 250) and cancer (week 377)). In total, four (5%) patients developed cancer during follow-up (AZA/MP (n=2), non-Hodgkin's lymphoma and breast plus colon cancer; CY (n=2), cervical carcinoma and unknown primary tumor with liver metastases). The number of female patients who reached menopause or who became pregnant, the number of pregnancies and the number of patients with infections during follow-up were comparable between both treatment groups (data not shown).
Aside from the patients who switched immunosuppressive treatment because of renal relapse or failure, six patients switched immunosuppressive treatment because of other reasons: four switched from AZA to mycophenolate mofetil (MMF) because of intolerance of AZA, one switched from AZA to chemotherapy (including CY) because of non-Hodgkin's lymphoma, and one switched from CY to chemotherapy because of colon cancer.
Laboratory assessments during follow-up
The changes in laboratory values during the 10-year follow-up are shown in figure 2. Serum creatinine, proteinuria and the percentage of anti-dsDNA positive patients decreased compared to pretreatment values (p<0.05). No significant differences in the course of these laboratory values were found between the AZA/MP and CY group. Furthermore, serum levels of C3 and C4 increased during treatment (p<0.05). Although complement levels remained somewhat lower in the AZA/MP group, no significant differences in the course of C3 and C4 were found between treatment groups in multilevel analysis.

{kind=link}
{kind=link}
Laboratory values (medians unless otherwise indicated) during 10-year follow-up; AZA/MP group versus CY group: (a) serum creatinine, (b) proteinuria, (c) anti-dsDNA positivity, (d) C3, (e) C4. anti-dsDNA, anti-double-stranded DNA antibodies; AZA/MP, azathioprine/methylprednisolone; CY, cyclophosphamide; C3, complement factor 3; C4, complement factor 4.
Parameters at last follow-up
At last visit, no significant differences between the AZA/MP and CY group were found in serum creatinine (median, 92 vs 81 µmol/L; median follow-up 9.6 years) or proteinuria (median, 0.20 vs 0.30 g/day; median follow-up 8.1 years). Furthermore, immunosuppressive treatment regimens at last follow-up were comparable between both groups. Most patients were still taking low doses of AZA combined with prednisone (52%). Other immunosuppressive regimens included AZA alone (6%), prednisone alone (13%), MMF combined with prednisone (12%), MMF alone (1%) and others (3%), while 13% of patients had discontinued all immunosuppressive drugs.
At last follow-up, more patients in the AZA/MP group were taking ACE inhibitors compared to the CY group (72% vs 47%, p=0.020; all antihypertensive drugs: 92% vs 70%, p=0.030). The number of antihypertensive drugs (both groups: median 1), systolic and diastolic blood pressure (AZA/MP: median 120 and 80 mmHg vs CY: median 120 and 77 mmHg), and the number of patients receiving statins (AZA/MP: 28% vs CY: 22%) were comparable between treatment groups. Furthermore, no significant difference was found in proteinuria at last visit between patients with and without ACE inhibitor use (data not shown). Finally, the percentage of patients taking ACE inhibitors at time of a renal relapse was comparable between both treatment groups (AZA/MP: 86% vs CY: 100%; proteinuric flares, AZA/MP: 80% vs CY: 100%).
Predictors of renal outcome
Time to occurrence of sustained doubling of serum creatinine
At baseline, the non-Caucasian ethnicity was the only independent predictor of time to occurrence of sustained doubling of serum creatinine in multivariate Cox regression (table 2). Since the number of patients with a repeat renal biopsy who reached sustained doubling of serum creatinine after 2 years was low (n=3), predictor analysis at the time of the repeat renal biopsy (at 2 years after inclusion) was not performed.
Baseline predictors of time to occurrence of sustained doubling of serum creatinine and renal relapse
Time to occurrence of renal relapse
Multivariate Cox regression showed that time to occurrence of renal relapse could not be predicted by the clinical, laboratory or renal biopsy parameters at baseline. However, induction treatment with AZA/MP was independently associated with this event (table 2). At 2 years after inclusion, induction treatment with AZA/MP, higher serum creatinine and higher proteinuria were independent predictors of time to occurrence of renal relapse beyond the second year (supplementary table S1). For baseline to 2-year change, a decrease in AI was the only independent inversely related predictor of time to occurrence of renal relapse after 2 years (table 3).
Predictive value of baseline to 2-year change in laboratory and renal biopsy parameters
Serum creatinine at last visit
At baseline, male gender, non-Caucasian ethnicity, higher age and higher serum creatinine were independent predictors of serum creatinine at last visit in multivariate linear regression (table 4). The adjusted R2 of this model was 0.468. At 2 years, male gender, non-Caucasian ethnicity, higher age, presence of hypertension and higher serum creatinine were independent predictors of serum creatinine at last visit (adjusted R2, 0.446; supplementary table S2). For baseline to 2-year change, the decrease in proteinuria was the only independent inversely related predictor of serum creatinine at last visit (adjusted R2, 0.091; table 3).
Baseline predictors of serum creatinine (log) and proteinuria (square root) at last follow-up
Proteinuria at last visit
At baseline, non-Caucasian ethnicity, higher CI and lower AI were significantly associated with proteinuria at last visit in multivariate linear regression (adjusted R2, 0.230; table 4). At 2 years, anti-dsDNA positivity was the only independent predictor of proteinuria at last visit (adjusted R2, 0.043; supplementary table S2). None of the baseline to 2-year change parameters could independently predict proteinuria at last visit (table 3).
Discussion
In this report, we present the long-term follow-up of the first Dutch Lupus Nephritis Study; an open-label RCT comparing induction treatment with AZA/MP and high-dose ivCY. Previous studies have shown that long-term prospective data are needed to draw conclusions regarding renal outcome after immunosuppressive treatment.2 8 9 The present data show that induction treatment with ivCY was superior to AZA/MP in the prevention of renal relapses, but no significant differences between treatment groups were found in the proportion of patients with sustained doubling of serum creatinine, ESRD or mortality after the median follow-up of 9.6 years. Furthermore, the course of serum creatinine and proteinuria during follow-up as well as serum creatinine and proteinuria at last follow-up were comparable. As discussed previously 11, our main limitation is that the study was underpowered to detect a significant difference in the primary study end point.
Fortunately, the proportion of patients with severe deterioration of renal function was low in our study. These findings indicate that repetition of induction treatment (in case of a renal relapse) or switching to the other treatment arm (in case of treatment failure) could restore renal function in most patients with proliferative LN who experienced a renal relapse.
After initiation of this RCT, several alternative treatments have been evaluated. The Euro-Lupus Nephritis Trial showed that even after the follow-up of 10 years, results with low-dose ivCY were comparable to those with high-dose ivCY.8 Furthermore, the Aspreva Lupus Management Study demonstrated that induction treatment with MMF was as effective as high-dose ivCY,13 although long-term results are not yet published. In addition, the MAINTAIN Nephritis Trial showed that the efficacy of maintenance treatment with AZA was comparable to MMF.14 Still, we think that induction treatment with AZA/MP remains an alternative for those patients in whom fertility should be preserved. Furthermore, AZA allows pregnancy in contrast to MMF.
In contrast to the previously reported findings after the median follow-up of 6.4 years,7 the present long-term follow-up data of the same patients showed that higher CI and lower AI at baseline could independently predict proteinuria at the last follow-up. The predictive value of CI was also reported in previous studies.12 15,–,19, but the results published on AI were conflicting.12 15 17 18 20,–,24 Of note, neither CI at baseline nor after 2 years was predictive for renal relapse in our study. After our publication that the increase in CI was higher in AZA/MP treated patients, concern was raised that this higher increase might indicate poor renal outcome after a longer follow-up,25 but the present analyses demonstrated no significant difference in sustained doubling of serum creatinine (primary study end point) between both treatment groups after the median follow-up of 9.6 years.
The present data confirm our previous finding 7 that a protocolised repeat renal biopsy after 2 years does not provide much additional information with regard to long-term renal outcome after immunosuppressive treatment in patients with proliferative LN. Baseline to 2-year decrease in AI was inversely associated with time to occurrence of renal relapse after 2 years, but CI and AI from repeat renal biopsies could not predict long-term renal outcome. Furthermore, many clinical and laboratory parameters like non-Caucasian ethnicity, male gender, higher age, higher serum creatinine, higher proteinuria and anti-dsDNA positivity were identified as independent 2-year predictors of worse renal outcome after immunosuppressive treatment, indicating that standard repeat renal biopsies do not have much additional value for the prediction of long-term renal outcome in these patients. Though, these results should be interpreted with some caution since appropriate repeat renal biopsies were available from only 39 of the 87 included patients. Non-Caucasian ethnicity was one of the strongest predictors for sustained doubling of serum creatinine, and creatinine and proteinuria at the last follow-up. Therefore, other treatments like MMF should be considered in these patients.26
Since the presence of hypertension has been shown to be an important predictor of poor renal outcome in LN,17 20 21 27 recommendations for treatment of hypertension were given in the study protocol. Although significantly more patients in the AZA/MP group were taking ACE inhibitors or other antihypertensive drugs at last visit, systolic and diastolic blood pressure were comparable between both treatment groups. Furthermore, no significant difference was found in proteinuria at the last follow-up between patients with or without use of antihypertensive drugs.
In conclusion, several prognostic factors of renal outcome after immunosuppressive treatment in patients with proliferative LN are identified in this study. These long-term follow-up data confirm that induction treatment with high-dose ivCY is superior to AZA/MP in preventing renal relapses, but sustained doubling of serum creatinine, ESRD, mortality and renal function at last visit do not differ between both treatment groups. Therefore, induction treatment with AZA/MP can serve as an alternative for CY in patients with proliferative LN who wish to avoid infertility or who have a high risk of premature ovarian failure.
Acknowledgments
The authors would like to thank G Ligtenberg for coordinating the study; C van Straalen for her contribution to the data collection; H C van Houwelingen for his statistical support; S Florquin, I Bajema, R Goldschmeding, C Peutz-Kootstra and E J Steenbergen for scoring the renal biopsies and all patients and members of the Dutch Working Party on SLE who participated in the first Dutch Lupus Nephritis Study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Contributors SA contributed to the analysis and interpretation of data and to the drafting of the article. CG and MB contributed to the acquisition of data, analysis and interpretation of data, and to the drafting the article. RD contributed to the conception and design, acquisition of data and to the critical revision of the article. SB, RS and AV contributed to the acquisition of data and to the critical revision of the article. JB contributed to the conception and design, acquisition of data, analysis and interpretation of data, and to the drafting of the article. All authors read and approved the final article.
-
Funding Funding was obtained from the Dutch Kidney Foundation, Dutch Arthritis Association and NWO-AGIKO scholarship program.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the ethics committees of all participating hospitals.
-
Provenance and peer review Not commissioned; externally peer reviewed.