Article Text

Abstract
There is strong evidence from clinical trials that a ‘treat to target’ strategy is effective in reaching remission in rheumatoid arthritis (RA). However, the question is whether these results can be translated into daily clinical practice and clinical remission is a reachable target indeed.
Objective The study aims to investigate whether in early RA a treatment strategy aiming at Disease Activity Score (DAS) 28 <2.6 is more effective than ‘usual care’ treatment for reaching clinical remission after 1 year.
Methods Two early RA inception cohorts from two different regions including patients who fulfilled the American College of Rheumatology criteria for RA were compared. Patients in the tight-control cohort (n=126) were treated according to a DAS28-driven step-up treatment strategy starting with methotrexate, addition of sulphasalazine (SSZ) and exchange of SSZ by anti-tumour necrosis factor in case of failure. Patients in the usual-care cohort (n=126) were treated with methotrexate or SSZ, without DAS28-guided treatment decisions. The primary outcome was the percentage remission (DAS28<2.6) at 1 year. Time to first remission and change in DAS28 were secondary outcomes.
Results After 1 year, 55% of tight-control patients had a DAS28<2.6 versus 30% of usual care patients (OR 3.1, 95% CI 1.8 to 5.2). The median time to first remission was 25 weeks for tight control and more than 52 weeks for usual care (p<0.0001). The DAS28 decreased with −2.5 in tight control and −1.5 in usual care (p<0.0001).
Conclusion In early RA, a tight control treatment strategy aiming for remission leads to more rapid DAS28 remission and higher percentages of remission after 1 year than does a usual care treatment.
Statistics from Altmetric.com
Introduction
The ultimate goal in rheumatoid arthritis (RA) treatment is to achieve and sustain clinical remission as early as possible in order to prevent joint damage and functional disability.1,–,3 Current treatment approaches include early and intensive treatment, which are believed to be essential to achieve early remission and to provide a better clinical outcome of RA treatment.4,–,11
Several clinical trials have demonstrated that applying a tight control strategy is effective in reducing disease activity, disability and progression of joint damage.7 12,–,14 Tight control in RA is defined as optimising treatment by measurement of disease activity in order to make treatment adjustments to reach a predefined target, notably low disease activity or clinical remission.15,–,17 It is suggested that disease activity measurement in combination with a treatment protocol is more effective than tight control without protocol-driven treatment changes.18 However, the question is whether these results of clinical trials of tight control indeed can be translated into daily clinical practice.
Therefore, two inception cohorts from two different regions were used to study the effect of tight control versus ‘usual care’ in early RA: one tight-control cohort with remission as treatment goal and one usual-care cohort. Cohort data from daily clinical practice are of value to investigate the effects of interventions in daily practice, including the effects of tight control.19 20 The patients included in a clinical cohort are supposed to be representative of the population with RA, and they are treated under daily practice circumstances.
The aim of this study was to investigate in early RA whether a tight control treatment strategy is more effective than treatment according to usual care in reaching remission after 1 year, in daily clinical practice cohorts.
Methods
Study design
For the aim of this quasi-experimental study, patients were selected from two distinct early RA inception cohorts from outpatient clinics in two different regions in The Netherlands, where all patients with RA are treated by clinic based rheumatologists. In the ‘tight control’ cohort, regular evaluation of disease activity was applied in combination with protocolised treatment adjustments aiming for remission.21 In the usual care cohort, patients were treated according to daily clinical practice, with regular evaluation of disease activity but without protocolised treatment adjustments.22 Each patient gave informed consent before the inclusion in the inception cohorts, and the responsible local medical ethics committee had approved the study protocols of both cohorts. The inclusion and the data collection are still ongoing.
Data selection
In both cohorts, patients with early RA were included according to the following inclusion criteria: meeting the 1987 revised American College of Rheumatology classification criteria for RA,23 age ≥18 years, disease duration less than 1 year and no previous treatment with disease modifying antirheumatic drugs (DMARDs) or prednisolone. Patients were included at diagnosis. For the current study, all included patients had a complete Disease Activity Score based on 28 joint counts (DAS28) at baseline, had a minimal follow-up time of 48 weeks and were not in remission at baseline.
Tight control
Since January 2006, consecutive patients with early RA were enrolled in the Dutch Rheumatoid Arthritis Monitoring remission induction cohort study. The rheumatology clinics of three hospitals in The Netherlands—Medisch Spectrum Twente, Enschede; Ziekenhuisgroep Twente, Almelo/Hengelo; and Isala Klinieken, Zwolle—participated in this study.
Patients visited the clinic at weeks 0, 8, 12, 20, 24, 36 and 52, and every 3 months thereafter. Treatment adjustments were standardised and protocolised, aiming at remission using the DAS28 with DAS28<2.6 as cut point. Patients started treatment with methotrexate (MTX) 15 mg/week upon diagnosis. In case of inefficacy, the consecutive intensification steps with DMARD medication were, at week 8, increase in MTX dose to 25 mg/week; at week 12, addition of sulphasalazine (SSZ) 2000 mg/day; and at week 20, increase in SSZ dose to 3000 mg. In accordance with the Dutch guidelines, anti-tumour necrosis factor (TNF) treatment was prescribed for patients whose DAS28 remained ≥3.2. These subsequent steps included, at week 24, adalimumab 40 mg every 2 weeks; at week 36, frequency increase of adalimumab to every week; at week 52, exchange of adalimumab for etanercept 50 mg per week; after 1 year and 3 months, infliximab 3 mg/kg bodyweight every 8 weeks; and after 1 year and 6 months, frequency increase of infliximab to every 4 weeks.
If the remission target of DAS28<2.6 was met, medication was not changed. In case of sustained remission (≥6 months) the most recently added drug would be tapered.
Non-steroidal anti-inflammatory drugs (NSAIDs), prednisolone at ≤10 mg/day and intra-articular corticosteroid injections were allowed at the discretion of the attending rheumatologist.
Usual care
In the usual-care cohort, patients were visiting (between March 2005 and 2008) the outpatient clinic of the rheumatology departments of the Radboud University Nijmegen or of the Maartenskliniek in Nijmegen, The Netherlands.
In this cohort, all patients were regularly assessed using the DAS28 at weeks 0, 12, 24, 36 and 52, but treatment decisions could be made at any time, according to the discretion of the treating rheumatologist. Patients were treated with conventional DMARDs and/or biologicals following the guidelines for RA.24 25 A common strategy applied was starting with MTX mono treatment, subsequently switching to SSZ or adding SSZ in case of MTX failure, and adding an anti-TNF agent after two or more DMARDs failed, in accordance with the Dutch guidelines. Also, NSAIDs and prednisolone (oral or injections) could be used at the discretion of the attending rheumatologist.
Clinical assessments
The following variables were collected at baselines: age, sex, disease duration, symptom duration, anti-cyclic citrullinic peptidepositivity and rheumatoid factor positivity. Clinical assessments included the DAS28 every 3 months and the Dutch version of the disability index of the Health Assessment Questionnaire (HAQ) every 6 months.26 27 Research nurses assessed the variables needed for the DAS28.26 Other clinical variables assessed were patient rating for pain on a 100 mm Visual Analogue Scale and C reactive protein (mg/l). Changes in DMARD and/or biological treatment and concomitant treatments with prednisolone (oral/intramuscular) and/or NSAIDs were standardly registered during follow-up.
Outcome measures
The primary outcome of this study was the percentage remission (DAS28 <2.6) at 1 year after the baseline. Secondary outcome measures were time to achieve remission, the course over time of the DAS28, the percentage of patients with ‘low’ disease activity (DAS28≤3.2), the mean change in DAS28 and individual core set variables from baseline to 1 year.28
Sample size estimation
Sample size was estimated for the primary outcome measure, percentage remission (DAS28<2.6) at 1 year. It was aimed to detect a clinically relevant difference in remission of 20% between both groups, assuming that tight control would show more effectiveness than usual care. Applying an α of 0.05 (conventionally two-sided) and a 1-β (‘power’) of 0.90, the necessary sample size was estimated to be at least 2×125=250 patients. Consequently, 126 patients were included from the tight control cohort, and 126 from the usual care cohort.
Statistical analyses
Logistic regression analysis was performed to test whether there was a between group difference in the occurrence of remission according to a DAS28<2.6 (primary outcome). Confounder correction was applied by adding potential confounders to the logistic regression model using 10% change in the main effect as selection criterion. Further, it was analysed whether the effect between treatment groups would be dependent of symptom duration (≤18 weeks vs >18 weeks).29
Kaplan–Meier survival curves and Cox proportional hazards regression modelling including confounder correction were used to analyse a between-group difference in time to achieve remission. The course over time of the DAS28 in both groups was analysed using longitudinal linear regression (mixed models), correcting for repeated measurements using an autoregressive covariance structure. Treatment with DMARDs, anti-TNF and prednisolone was described for both groups.
The level of significance was set at a two-sided p value less than 0.05. The statistical analyses were carried out using the Statistical Package for the Social Sciences (version 16.0).
Results
Baseline variables
Both treatment groups were similar at baseline (Table 1) regarding age and gender, as well as for time since diagnosis and baseline DAS28; nearly half of the patients had high disease activity (DAS28>5.1). The symptom duration was lower, while HAQ, patient's rating of pain and patient's global assessment of disease activity were higher in the tight control group.
Demographic and baseline disease characteristics
Remission
After 1 year, 55% of tight-control patients were in DAS28 remission compared to 30% of usual-care patients (p<0.0001), (figure 1A). The OR was 3.1 (95% CI 1.8 to 5.2) adjusted for baseline DAS28; there were no confounders. Accordingly, patients treated according to tight control had about a three times higher odds to have a DAS28<2.6 1 year after the baseline. There were no patients in 6 months remission for whom medication could be suspended.

Remission and disease activity levels after 1 year. (A) Remission (DAS28<2.6) and levels of low (DAS28≤3.2), moderate (3.2<DAS28≤5.1) and high (5.1<DAS28) disease activity at 12 months of tight-control and usual-care groups. (B) Remission at 12 months in tight-control and usual-care groups, by equal subgroups of short (≤18 weeks) and longer (>18 weeks) symptom duration. DAS28, Disease Activity Score based on 28 joint counts.
Symptom duration and remission
The study sample was split in two equal subsamples according to median symptom duration (18 weeks). In patients with a short symptom duration (n=126), 57% of tight-control patients were in DAS28 remission compared to 43% of usual-care patients (p=0.041), with an OR of 2.2 (95% CI 1.0 to 4.7), (figure 1B). In patients with longer symptom duration (n=126), 52% of tight-control-treated patients and 21% of usual-care-treated patients were in remission (p<0.0001), with an OR of 4.1 (95% CI 1.9 to 8.9).
Low disease activity
In the tight-control group, there were more patients reaching low disease activity (p<0.0001) than in the usual-care group (figure 1A). In the tight-control group, 75% had low disease activity, 22% had moderate disease activity and 3% had high disease activity. In the usual care group, 42% of patients had low disease activity, 49% had moderate disease activity and 9% had high disease activity.
Time to achieve remission
Time to remission (DAS28<2.6) was significantly shorter in the tight-control group than in the usual-care group, with a median of 25 weeks versus a median over 52 weeks (p<0.0001), (figure 2). Already after 8 weeks, the survival curve of the tight control group appeared to diverge.

Time to achieve first remission after 1 year of follow-up. Survival curve of time to reach remission (DAS28 <2.6) for tight-control and usual-care groups over 1 year. DAS28, Disease Activity Score based on 28 joint counts.
Course over time of the DAS28
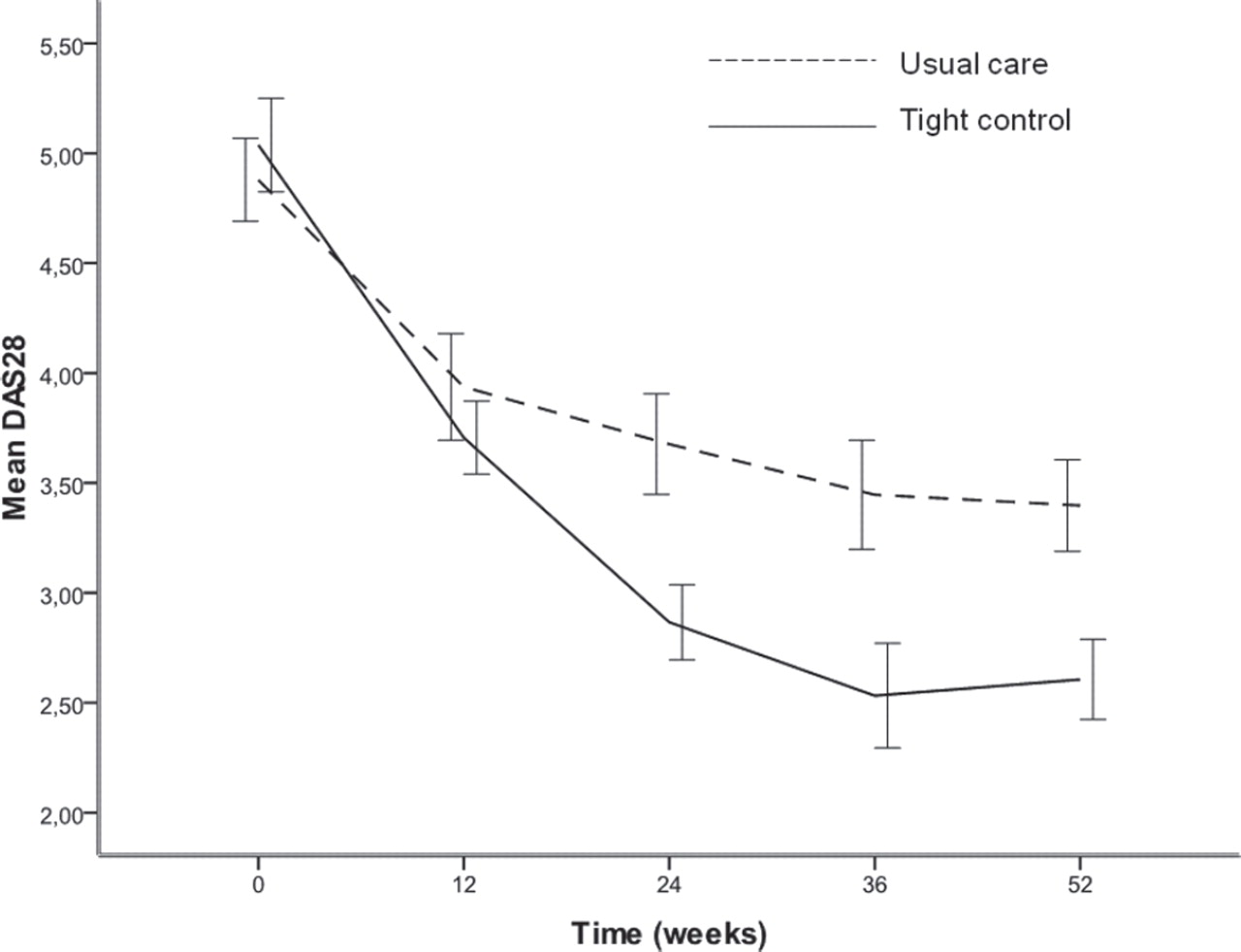
Figure 3 depicts the course over time of the DAS28 in both groups. It can be seen that the decrease in DAS28 was similar for both groups in the first 12 weeks of treatment, but after 12 weeks the decrease continued in the tight-control group. Also according to the mixed models analysis, the course over time of DAS28 was significantly different between both groups (p<0.0001).
{kind=link}
{kind=link}
{kind=link}
Mean (SEM) decrease of DAS28 in tight-control and usual care groups over 1 year. DAS28, Disease Activity Score based on 28 joints.
Decrease in DAS28 and core set variables
Table 2 shows the average changes from baseline to 1 year of individual core set variables and the DAS28. In all core set variables, except for the acute phase response (erythrocyte sedimentation rate and C reactive protein), the improvements were significantly larger in the tight-control group.
Average change from baseline to 1 year in core set variables
Medication use
Patients in the tight-control group started with MTX (table 3). After 1 year, 50% of the patients were still on MTX mono treatment, and 30% received a combination of DMARDs, nearly always MTX and SSZ. After 1 year, 12% of the patients in the tight-control group received anti-TNF, and 9 (7%) patients started adalimumab every week. Intra-articular injections with methylprednisolone were given to 25% of the patients who received one to three injections.
Medication use in tight-control (n=126) and usual-care (n=126) groups
Patients treated according to usual care usually started with MTX or SSZ mono treatment (table 3). After 1 year of follow-up, most patients were still on DMARD mono treatment; about 19% had switched to another DMARD, and 16% of the patients had two DMARDs. After 1 year, anti-TNF treatment had been given for 6% of the patients. Oral prednisolone was given to 20% of the patients in a median dose of 15 mg/day, and 54% of the patients received one to three intramuscular injections with methylprednisolone 120 mg.
Drug survival and adverse events
In the tight-control group, 120 patients started MTX and 12 (10%) patients stopped MTX again. Nine of them switched to another DMARD, and three patients restarted MTX. Reasons for stopping MTX were toxicity (n=9), patient's wish (n=2) and an unknown reason (n=1).
In the control group, 94 patients started MTX during the year, and 10 (11%) patients stopped again, for toxicity (n=6), inefficacy (n=1) and other reasons (n=3). Of the 44 patients who started SSZ, 22 (50%) stopped using SSZ, usually because of toxicity (n=19).
Discussion
According to the results of this study, a tight control treatment strategy aiming for remission leads to more patients being in remission more rapidly than treatment according to usual care in early RA. After 1 year, remission (DAS28<2.6) was reached in 55% of patients in the tight-control group as compared to 30% of patients in the usual-care group. Concordantly, the tight control strategy resulted in a larger decrease of DAS28, more patients having low disease activity, and larger improvements in functional ability and patient assessments of pain and disease activity. The tight control regimen could well be tolerated and did not appear to cause additional toxicity; 88% of the patients still used MTX after 1 year. Tight control performed nearly equally well in patients with shorter (≤18 weeks) and longer symptom duration, but the performance of usual care was much less in patients with longer disease duration.
This quasi-experimental study was performed using daily practice data of two early RA cohorts. The results of this study are in accordance with those from tight control randomised controlled trials Tight Control of Rheumatoid Arthritis (TICORA), Computer Assisted Monitoring of Rheumatoid Arthritis (CAMERA).12 13 Also, the quasi-experimental study of Goekoop et al compared tight control treatment with usual care and showed a better response after 1 year for tight control.14 The results from the current study are valuable, as they contribute to the robustness of the finding that tight control is effective and feasible for the treatment of early RA in daily practice. In this study, it is also pointed out that, in usual care, early treatment (≤18 weeks symptom duration) is more effective than later treatment (>18 weeks).29 The negative effect of longer symptom duration on outcome could be encountered by using intensive DMARD treatment, as applied in the tight control strategy. But both in ≤18 weeks and in >18 weeks subgroups, tight control was significantly more effective than usual care.
Notably, a beneficial effect on disease activity is reached through medication in the therapeutic regimen, not by measurement and target setting per se. The difference between the two groups in this study was in the strictness of the rules when to prescribe which medication. Therefore, it can be deduced that adding a treatment protocol to the measurement and goal setting is needed to optimise the effects of tight control. The main differences in treatment strategy between the groups were that, in the tight-control group, nearly all patients started with MTX, while MTX start was delayed in the usual care group, and that combination treatment and anti-TNF was more frequently used in the tight-control group.
There also are worries about tight control. Patients would not tolerate the intensivation of MTX (DMARD) treatment and would cycle too quickly through all treatment options. In the tight-control arm of this study, MTX was well tolerated. MTX 1-year drug survival was 88%, and the proportion of toxicity related drug stops was similar to the usual care group. Moreover, anti-TNF was not much needed, and at 1 year, no patients had moved through the complete treatment algorithm. In the usual-care group, the drug survival of SSZ appeared to be poor, and quite much intramuscular glucocorticosteroids was needed as ‘bridge’ or ‘escape’ treatment. The implications of the findings of this study are that aiming for remission is feasible in daily clinical practice and that clinical remission, or rather near-remission, can be our current treatment goal.3 30 In essence, remission should be regarded as the absence of clinical disease activity and absence of progression of joint damage.31 32 Performing tight control places a burden on busy practice. However, the model of tight control in early RA is that many visits and medication changes are performed in the beginning of the disease, with the outlook of reducing the number of visits later. As the name ‘tight control’ indicates, apparently some degree of vigorousness is needed in bringing tight control to a success in daily clinical practice. Further, tight control with protocolised treatment adjustments contributes to a better disease outcome compared to non-protocolised treatment adjustments.15 17 33 A multitude of treatment strategies have shown to be effective in RA, and there is choice as to which could be used in a treatment protocol.1 8 11 16 34,–,36
This study also has its limitations. In this study, DAS28 was used to define remission in early RA. However, patients with a DAS28<2.6 may have residual disease activity, and synovitis may be present in joints not included in the 28 joint count.37 More stringent remission criteria are infrequently met in patients with RA.38 The finding that a DAS28<2.6 can be reached in practice, as we showed, supports the movement to more stringent remission criteria. Another limitation of this study is the follow-up of 1 year. We regard that 1 year is reasonably informative but longer follow-up is needed to get insight into long-term efficacy of tight control, also regarding progression of joint damage. Data on joint damage progression are currently not available. Future research in these cohorts will focus on long-term effects, joint damage progression, safety and performance in patients fulfilling the revised American College of Rheumatology/European League Against Rheumatism classification criteria for RA.19 While as much as 75% of patients were in low disease activity after 1 year, there were still 25% of patients with moderate or high disease activity. This raises two questions for future research: how many patients will attain sustained remission and may reduce medication, and what is an appropriate strategy for patients not able to reach low disease activity?
In conclusion, it was shown that in early RA, a tight-control approach including regular measurement of the DAS28 and protocolised treatment decisions is feasible in daily practice and that it leads to more rapid DAS28 remission and higher percentages of DAS28 remission after 1 year than usual care treatment.
Acknowledgments
The authors are grateful for the support by our research nurses and data management for the collection of data and the participation of our patients.
References
Footnotes
-
Contributors J Fransen and HH Kuper contributed in the study concept. P van Riel and M van de Laar contributed in the cohort and intervention design. L Schipper, M Vermeer and J Fransen contributed in the analysis. LG Schipper, M Vermeer and J Fransen. M Hoekstra, C Haagsma, A den Broeder, M van de Laar and P van Riel reviewed the manuscript.
-
Funding The work of LG Schipper was supported by an implementation grant by Wyeth Pharmaceuticals, The Netherlands. The work of M Vermeer was funded by an unrestricted educational grant by Abbott, The Netherlands. The study sponsors had no influence on the study design, collection, analysis and interpretation of data, in the writing of the report and in the decision to submit the paper for publication.
-
Competing interests The co-authors cooperate in the Dutch Rheumatoid Arthritis Monitoring biological registry, for which funding has been received from the Dutch affiliations of Wyeth Pharmaceuticals, Abbott Pharmaceuticals, Schering-Plough Corporation, Roche pharmaceuticals, UCB Pharma and Bristol-Myers Squibb to enable data collection for the Dutch Rheumatoid Arthritis Monitoring registry.
-
Ethics approval Ethics approval was obtained from the Medisch Ethische Toetsingscommissie Arnhem Nijmegen and the Medisch Ethische Toetsingscommissie Twente.
-
Provenance and peer review Not commissioned; externally peer reviewed.