Article Text

Abstract
Objective Anticitrullinated protein antibodies (ACPAs) are suggested to identify different subsets of patients with rheumatoid arthritis (RA). The authors compared the clinical and radiological responses to Disease Activity Score (DAS)-steered treatment in patients with RA positive or RA negative for ACPA.
Methods In the BehandelStrategieën (BeSt) study, 508 patients with recent-onset RA were randomised to four treatment strategies aimed at a DAS ≤2.4. Risks of damage progression and (drug-free) remission in 8 years were compared for ACPA-positive and ACPA-negative patients using logistic regression analysis. Functional ability and DAS components over time were compared using linear mixed models.
Results DAS reduction was achieved similarly in ACPA-positive and ACPA-negative patients in all treatment strategy groups, with a similar need to adjust treatment because of inadequate response. Functional ability and remission rates were not different for ACPA-positive and ACPA-negative patients. ACPA-positive patients had more radiological damage progression, especially after initial monotherapy. They had a lower chance of achieving (persistent) drug-free remission.
Conclusion Clinical response to treatment was similar in ACPA-positive and ACPA-negative patients. However, more ACPA-positive patients, especially those treated with initial monotherapy, had significant radiological damage progression, indicating that methotrexate monotherapy and DAS- (≤2.4) steered treatment might be insufficient to adequately suppress joint damage progression in these patients.
Statistics from Altmetric.com
Introduction
Anticitrullinated protein antibodies (ACPAs) are highly specific antibodies for rheumatoid arthritis (RA).1 Patients positive for ACPA have been shown to have higher disease activity,2 3 worse functional ability4 5 and more joint damage2 3 6 7 in observational and/or non-disease activity-steered studies. ACPA-positivity was found to be predictive of not achieving remission.8 ACPA-negative and ACPA-positive RA may be different diseases with different risk factors and clinical course and may require different therapeutic strategies.9,–,11 Possibly, ACPA-positive and ACPA-negative patients also respond differently in a tight control treatment strategy where medication is adjusted based on the aim of achieving low disease activity. Therefore, we compared the changes in Disease Activity Score (DAS) functional ability and radiological damage over time in ACPA-positive and ACPA-negative early patients with RA treated according to the same disease activity steered protocol.
Methods
Patients
Eight-year follow-up data of all 484 patients with known ACPA-status included in the BeSt (Dutch acronym for BehandelStrategieën, “treatment strategies”) study were analysed. This is a multicentre randomised trial designed to compare four treatment strategies in 508 patients with recent-onset RA; initial monotherapy, step-up combination treatment (both starting with methotrexate monotherapy for ≥6 months), initial combination treatment with methotrexate, sulfasalazine and prednisolone and initial combination treatment with methotrexate and infliximab. Treatment was assessed every 3 months and adjusted if the DAS was >2.4. If the DAS was ≤2.4 for ≥6 months, medication was tapered to monotherapy in maintenance dose. Starting 2 years after inclusion, patients on monotherapy maintenance dose, who were in remission (DAS <1.6) for ≥6 months, stopped the last disease-modifying antirheumatic drug (DMARD). Treatment was restarted if the DAS increased to ≥1.6. A more detailed description of the study protocol was published previously.12
Study end points
ACPA-status was determined with the CCP2 test using baseline sera (n=119) and sera collected during the first years of follow-up (n=365). The DAS and Health Assessment Questionnaire (HAQ) were used to assess treatment response. Drug-free remission was defined as DAS <1.6 and not using any DMARD. All available x-rays of hands and feet at year 0-1-2-3-4-5-6-7-8 were scored using the Sharp/van der Heijde Score (SHS) by two independent readers, blinded for patient identity and time order (interobserver, intraclass correlation coefficient 0.96), to assess joint damage. For DAS and DAS components, areas under the curve (AUC) were calculated only for years with complete data. For years with ≤2 missing values, the last observation carried forward was used to calculate the AUC to avoid exclusion of these data.
Statistical analysis
Baseline characteristics and clinical parameters were compared using the χ2 test, Student t test or Mann—Whitney U test. HAQ and DAS components over time were compared using linear mixed models with ACPA-status and time as categorical variables and HAQ or DAS component, respectively at baseline, adjusted for baseline gender, smoking habits, age and SHS with a Toeplitz covariance structure. Spearman's correlation coefficient test was used to analyse the correlations after 8 years. ORs for achieving (drug-free) remission of restarting medication and of joint damage progression were calculated for ACPA-positive patients using logistic regression analyses, adjusted for gender, smoking habits, baseline age, DAS and SHS. ORs were converted to RRs to find a more accurate estimation of the effect size.13
To examine the influence of treatment strategy, we used generalised estimating equations with an auto-regressive covariance structure, time as categorical variable, baseline SHS, DAS, age, gender, smoking habits, ACPA-status, treatment strategy and ACPA* treatment strategy with yearly damage progression as outcome. To assess the possible difference in the association between disease activity and joint damage progression for ACPA-positive and ACPA-negative patients, we used generalised estimating equations with these components but with treatment strategy replaced by yearly AUC DAS or AUC DAS component (with baseline DAS component instead of baseline DAS).
Results
Treatment response
ACPA-positive patients had a lower baseline DAS and HAQ and a higher SHS. Disease activity over time was similar in both ACPA groups (figure 1a). Functional ability was not different for ACPA-positive and ACPA-negative patients (p=0.9) (figure 1b). This similar treatment response in both ACPA-groups was seen both in patients initially treated with methotrexate monotherapy and with combination treatment, (p=0.8 and p=0.9) (supplemental file online 1). ACPA-positive patients did have a significantly higher (4.5 mm/h) erythrocyte sedimentation rate (ESR) (figure 1c). Disease activity and functional ability showed a moderate correlation after 8 years: rs:0.5 (p<0.001). The rates of achieving remission at least once or ≥1 year consecutively were not different: RR of 1.0 (95% C.I. 0.9 to 1.1) and 0.9 (0.7–1.1), respectively. ACPA-positive patients were less likely to achieve drug-free remission, with a RR of 0.4 (0.3–0.7) and more likely to lose remission and having to restart DMARDs: RR 2.3 (1.4–3.0). Similar results were seen for patients who were ACPA and RF positive or negative.

(A) DAS, (B) HAQ, (C) ESR, erythrocyte sedimentation rate, (D) patient VAS, visual analogue scale global health, (E) Ritchie Articular Index and (F) Swollen Joint count over 8 years for anticitrullinated protein antibodies (ACPA)-positive and ACPA-negative patients. ACPA, anticitrullinated protein antibodies; DAS, Disease Activity Score; HAQ, Health Assessment Questionnaire.
The median number of treatment steps (2 (IQR 1–4) vs 1 (1–4)) that patients had failed on and the proportions of patients who had dropped out before year 8 were not significantly different for ACPA-positive and ACPA-negative patients in the whole cohort or when stratified for initial treatment strategy.
Joint damage progression
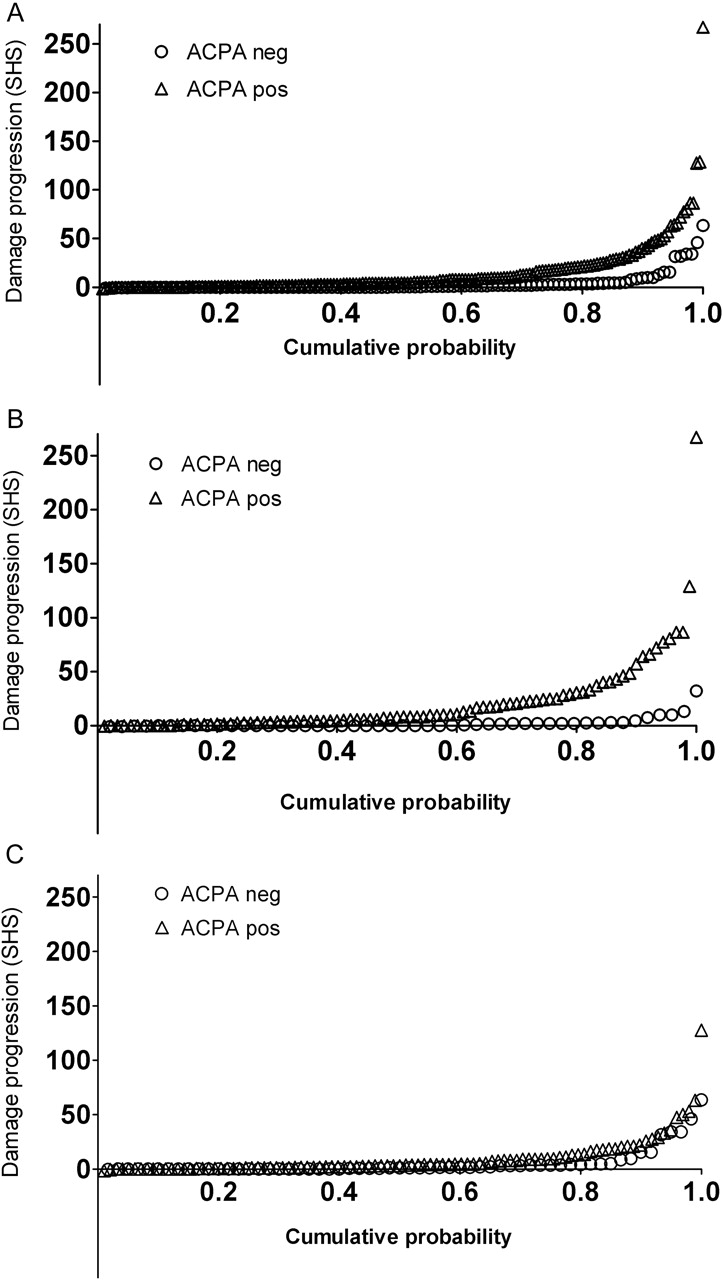
ACPA-positive patients showed more radiological damage progression than ACPA-negative patients (figure 2a). The RR for progression >5 points (SHS) was 3.8 (95% C.I. 2.5 to 5.0), 3.7 (1.9–6.3) for >15 points, 3.2 (1.4–6.4) for >25 and 6.2 (1.5–20.3) for >35 points. Similar results were seen from patients who had been in remission for ≥1 year (online supplemental file 2) and for patients who were ACPA- and RF positive or negative. ACPA was a predictor of joint damage progression independent of RF.

{kind=link}
{kind=link}
Probability plots of joint damage progression over 8 years for anticitrullinated protein antibodies (ACPA)-positive and ACPA-negative patients, (A) All patients, (B) initial treatment monotherapy (groups 1 and 2), (C) initial combination treatment (groups 3 and 4).
The association of ACPA-status with joint damage progression was significantly influenced by initial treatment strategy (monotherapy or combination treatment) (figure 2b,2c). The difference in SHS between ACPA-positive and ACPA-negative patients initially treated with combination treatment was 1.7 points smaller than the difference in SHS for ACPA-positive and ACPA-negative patients initially treated with monotherapy (p<0.001). Second, the association was influenced by disease activity. ACPA-positive patients showed 1.8 points more increase in SHS per point of the DAS (p=0.001), 0.1 points per mm/h ESR (p=0.003), 0.2 per tender joint (p=0.02) and 0.1 per swollen joint (p=0.005). The association with visual analogue scale (VAS) global health was not influenced by ACPA-status. Joint damage and functional ability at year 8 did not show a significant correlation.
Discussion
Response to DAS-steered treatment was similar in ACPA-positive and ACPA-negative patients in terms of reduction of disease activity including remission percentages and improvement of functional ability, although ACPA-positive patients had a higher ESR over time. ACPA-positive patients did show more joint damage progression, in particular, in patients treated with initial methotrexate monotherapy. ACPA-positivity, also, was a predictor for not achieving and for losing drug-free remission. To our knowledge, we are the first to report on disease activity in ACPA-positive and ACPA-negative patients in a disease activity-steered treated cohort. In previous non-disease activity-steered studies of patients with similar disease duration, ACPA-positive patients did show higher disease activity.2 3 In a study of 273 patients with recent-onset RA with 6 years of follow-up,7 similar functional ability was found for ACPA-positive and ACPA-negative patients after correction for disease activity and RF, but ACPA-positive patients had more joint damage, which is in line with our results. The relatively short follow-up period may account for these findings, as radiological joint damage shows a weak correlation with functional ability in the first years after the diagnosis of RA but a moderate correlation after 12 years, while disease activity shows a stable, moderate correlation with functional ability from baseline onwards.14 In our tight controlled cohort, we found a moderate correlation between functional ability and disease activity but no significant correlation with radiological joint damage after 8 years. Longer follow-up will show whether radiological joint damage will significantly contribute to functional disability with longer disease duration.
Our observation that ACPA-positivity is a predictor for not achieving drug-free remission and for relapsing if drug-free remission was achieved, is an extension on similar results after 5 years of treatment.15 The results are also in line with the findings of Balsa et al,5 who found that ACPA-positivity was a predictor for not achieving drug-free remission for ≥5 years and of van der Woude et al16 who found that ACPA-positivity was a predictor for not achieving drug-free remission for ≥1 year. It might be wise to take ACPA-status into consideration when contemplating cessation of medication.
In conclusion, DAS-steered treatment is equally effective in reducing disease activity, achieving remission and improving functional ability in ACPA-positive and ACPA-negative patients with recent-onset RA. Still, ACPA-positive patients had more radiological damage, especially patients initially treated with methotrexate monotherapy. This suggests that in ACPA-positive patients, initial methotrexate monotherapy is insufficient to suppress joint damage progression even if subsequent treatment is DAS-steered. This is in line with our previous findings17 18 and those with the European League against Rheumatism recommendations, which suggest that in patients with poor prognostic factors such as ACPA-positivity, starting with combination treatment might be considered.19 It may also mean that for ACPA-positive patients, the target of DAS ≤2.4 might not be stringent enough. The differences in joint damage progression and systemic inflammation indicate that the inflammatory mechanisms in ACPA-positive and ACPA-negative RA might have different mediators.
Acknowledgments
The authors would like to thank all patients as well as the following rheumatologists (other than the authors) who participated in the Foundation for Applied Rheumatology Research (all locations are in The Netherlands): WM de Beus and M de Buck (Medical Center Haaglanden, Leidschendam); C Bijkerk and AJ Peeters, MD (Reinier de Graaf Gasthuis, Delft); MHW de Bois and G Collée (Medical Center Haaglanden, The Hague); H Boom (Spaarne Hospital, the Hague); JAPM Ewals, RJ Goekoop, YPM Goekoop-Ruiterman and HK Ronday (Haga Hospital, The Hague); AH Gerards and PAHM van der Lubbe (Vlietland Hospital, Schiedam); BAM Grillet (Zorgsaam, Terneuzen); JHLM van Groenendael (Franciscus Hospital, Roosendaal); JMW Hazes (Erasmus University Medical Center, Rotterdam); MH de Jager (Albert Schweitzer Hospital, Dordrecht); MV van Krugten (Admiraal de Ruyter Hospital, Vlissingen); H van der Leeden (retired); WF Lems (VUMC, Amsterdam); MF van Lieshout-Zuidema and JPh Terwiel, MD (Spaarne Hospital, Hoofddorp); C Mallée, KSS Steen, MD and S ten Wolde, MD (Kennemer Gasthuis, Haarlem); M van Oosterhout and AA Schouffoer (Groene Hart Hospital, Gouda); D van Schaardenburg and AE Voskuyl, MD (VU medical center, Amsterdam); PEH Seys (Lievensberg hospital, Bergen op Zoom); PBJ de Sonnaville, MD (Oosterschelde Hospital, Goes); I Speyer, MD, GM Steup-Beekman and ML Westedt, MD (Bronovo Hospital, The Hague); JMGW Wouters, MD and D van Zeben, MD (Sint Franciscus Gasthuis, Rotterdam); The authors would also like to thank all the other rheumatologists and trainee rheumatologists who enrolled patients in this study and all research nurses for their contributions
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding The study was designed by the investigators and was supported by a government grant from the Dutch College of Health Insurance Companies, with additional funding from Centocor Inc. and Schering-Plough. Data collection, trial management, data collection, data analysis and preparation of the manuscript were performed by the authors.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from Leiden University Medical Center Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.