Article Text

Abstract
Aim To investigate the association between smoking and psoriatic arthritis (PsA) among patients with psoriasis and its interaction with the HLA-C*06 allele.
Methods In this exploratory case–control study, smoking status was determined at the time of the diagnosis of arthritis for PsA patients and at their first study visit for psoriasis patients, when they were confirmed not to have PsA. The proportions of patients exposed to smoking were compared in patients with PsA to those with psoriasis alone. A logistic regression model was constructed to test the independent association of smoking and PsA after adjusting for potential confounders. The statistical interaction between HLA-C*06 and smoking was tested through a regression model.
Results The proportions of current and past smokers were higher in the psoriasis group compared with the PsA group (30.2% vs 23.4% and 26.7% vs 22.3%, p=0.001, respectively). On multivariate analysis being a current smoker versus a lifetime non-smoker remained inversely associated with PsA (OR 0.57, p=0.002), while past smoker versus lifetime non-smoker status was no longer significant. In a subgroup analysis, smoking remained inversely associated with PsA only among patients who were HLA-C*06 negative. Regression analysis revealed that the interaction between smoking status (ever smoked vs lifetime non-smoker) and HLA-C*06 was statistically significant (p=0.01).
Conclusion Smoking may be inversely associated with PsA among psoriasis patients. This association is not present among HLA-C*06-positive individuals.
Statistics from Altmetric.com
Psoriatic arthritis (PsA) is an inflammatory arthritis that develops in up to one-third of patients with psoriasis.1 As the majority of patients develop inflammatory arthritis following the onset of psoriasis,2 PsA may be considered a more severe phenotype of the psoriatic disease that occurs due to a greater number of susceptibility genes or environmental factors.3
The association between smoking and psoriasis has been established in several studies.4,–,7 It has also been suggested that the effect of smoking may be modified in the presence of HLA-C*06. Their co-existence was associated with a significantly higher risk of developing psoriasis compared with the presence of each factor individually.8 We have recently reported that the prevalence of smoking was decreased among PsA patients compared with psoriasis patients without arthritis.9 There are several potential biological mechanisms underlying this observation. First, smoking was found to have a protective effect against ulcerative colitis, a disease that bears some clinical and genetic similarities to PsA.10,–,12 It has been suggested that decreased expression of interleukin (IL) 1β, IL-8 and altered response of Toll-like receptor pathways to infectious agents among smokers may explain this association.13 14 Another mechanism that may explain the protective effect of smoking is through the activation of the nicotinic receptor. Nicotine can activate the α7 nicotinic acetylcholine receptor that inhibits intracellular pro-inflammatory pathways that are associated with the development of arthritis.15 16
In this exploratory case–control study we aimed to investigate further our previous observation of an inverse association between smoking and PsA among psoriasis patients using a larger sample of patients.
Methods
Setting
In this case–control study, two groups of patients were compared.
Cases
Adult prevalent PsA patients were part of the University of Toronto PsA cohort. The cohort was established in 1978 as part of an ongoing prospective study. The clinic serves as a primary, secondary and tertiary referral centre for PsA patients from the greater Toronto area and southern Ontario. As classification criteria for PsA were not available until 2006, the diagnosis of PsA was based on the presence of psoriasis and inflammatory arthritis and the exclusion of other types of arthritis. However, 98% of the patients in the clinic satisfy the CASPAR criteria for classification of PsA.17 The patients are followed in the clinic according to a standardised protocol.2 Data are tracked in a computerised database.
Controls
Psoriasis patients without arthritis were recruited from the University of Toronto psoriasis cohort that was established in 2006. The cohort was described in detail prevously.18 Briefly, all potential study subjects have a diagnosis of psoriasis confirmed by a dermatologist and have been assessed by a rheumatologist to exclude a diagnosis of PsA. The cohort aims to study risk factors for the development of PsA. Patients are recruited mainly from dermatology clinics and phototherapy centres in the greater Toronto area but also from family practice clinics and through advertisements in flyers and local media. All participants are followed according to the same protocol as in the PsA cohort and are assessed annually for symptoms or signs of arthritis. If inflammatory arthritis is diagnosed, the patient is considered to have developed the outcome of interest and is censored. This process ensures that all of the psoriasis cohort's patients are free of arthritis. For the purpose of this study psoriasis patients who developed PsA during the follow-up period were removed.
The study was approved by the university health network research ethics board and all patients gave their informed consent.
Patient selection
PsA patients included in the study were registered in the PsA clinic between 1978 and 2010. Psoriasis patients included in the study were registered in the psoriasis cohort between 2006 and 2010. PsA patients without psoriasis or those who developed the skin manifestation following the onset of arthritis were excluded. PsA and psoriasis patients within the database with available information about their smoking status at the time of the diagnosis of PsA and at their first study visit, respectively, were included in the study.
Determination of smoking status
Smoking status was categorised as current smoker, past smoker and life-time non-smoker. A smoker was defined as a person who smoked one or more cigarette per day for at least 1 year.
At enrolment, all study participants were asked to report their current smoking status and what was their smoking status at the time of the diagnosis of PsA (for PsA patients) and at the time of the diagnosis of psoriasis (for psoriasis patients). Patients were also asked to report the number of cigarettes and smoking years at the above defined time point.
The reference dates for the determination of smoking status were the time of diagnosis of PsA (for PsA patients) and the first study visit (for psoriasis patients). These dates were chosen because information about potential confounders was available only from the first assessment date.
Information about potential confounders was retrieved from the database including age, sex, duration of psoriasis, severity of psoriasis and alcohol consumption. Similar to smoking status, the reference dates used to determine alcohol consumption were before the diagnosis of PsA (for PsA patients) and at first study visit (for psoriasis patients). Alcohol consumption was categorised as daily (one or more alcoholic beverage a day), social (one or more alcoholic beverage a week) and non-drinker. As smoking is known to be associated with the severity of psoriasis, patients were categorised as those with severe psoriasis (psoriasis area severity index (PASI) ≥10), and mild psoriasis (PASI <10) based on the maximal PASI score in the first 3 years of follow-up.
HLA-C*06 allele typing
HLA-C*06 is the strongest genetic risk factor for psoriasis.19 The interaction between HLA-C*06 and smoking may play a role in the susceptibility to psoriasis.8 We therefore investigated whether the effect of smoking is modified by this allele. Human leucocyte antigen (HLA) typing was performed routinely for all individuals enrolled in the PsA or psoriasis cohorts for whom DNA was available. For HLA typing, extracted genomic DNA was amplified by PCR using locus-specific primers for the HLA-C locus. PCR amplicons were identified by sequence-specific oligonucleotide probes using the reverse line blot technique (RELI sequence-specific oligonucleotide HLA typing kits).20
Statistical analysis
Baseline descriptive statistics were computed with continuous variables summarised by their means and SD and categorical variables were summarised by proportions. The proportions of exposure to smoking were compared between the PsA and psoriasis patients through calculation of the OR and the corresponding 95% CI.
In order to avoid bias due to ecological trends in smoking, we performed an additional analysis in a subset of the study population that included 404 PsA and psoriasis patients matched by age (within 5 years) and gender. Each psoriasis patient was assigned a reference year that was derived from the year of onset of PsA for the corresponding case. From the available information we were able to infer the years of exposure to smoking for 381 of the matched psoriasis patients. We then performed a conditional logistic regression for matched pairs data to determine the association between smoking status and PsA compared with psoriasis.
A logistic regression model was constructed with disease status as the outcome. The model included smoking status and the following potential confounders as covariates: age group (stratified by 10-year intervals); sex; duration of psoriasis (stratified by 5-year intervals); alcohol consumption and severity of psoriasis. Multivariate logistic regression analysis was used to assess the independent association between smoking and PsA. A sensitivity analysis was performed to assess whether the exclusion of patients with missing information on psoriasis severity and alcohol consumption from the multivariate analysis affected the results by the removal of these variables from the regression model.
Only Caucasians were included in the analysis of the interaction between HLA-C*06 and smoking to minimise population stratification bias. The proportions of exposure to smoking were compared between PsA and psoriasis after stratification by HLA-C*06 status using a likelihood ratio test. A logistic regression analysis was performed to assess the statistical interaction between HLA-C*06 and smoking.
The significance level was set at 0.05 for a two-sided test. Statistical analysis was performed using SAS 9.2 statistical software.
Results
Overall, 728 PsA and 404 psoriasis patients with complete information were included in the study. Most of the PsA patients had enrolled in the cohort over the past decade (19.9% from 1978 to 1989, 26.2% from 1990 to 1999 and 53.9% from 2000 to 2010). Overall, 257 PsA patients were not included in the analysis due to missing information about their smoking status. The majority of these patients were evaluated at the establishment of the PsA cohort; at that time such information was not routinely collected. Comparison of the excluded PsA patients with those included in the study revealed no significant differences in demographic and clinical characteristics apart from gender. The proportion of women was slightly higher among the PsA patients with missing information (49.8% vs 40.8%). The median time interval from the onset of PsA until the first assessment in the clinic was 3 years.
The PsA patients were on average 10 years younger and had a shorter duration of psoriasis (table 1). These differences are related to the use of different reference dates for the determination of smoking status: the year at onset of PsA (ranged from 1951 to 2010) for the PsA group versus first study visit for the psoriasis group (ranged from 2006 to 2010). PsA patients had more severe psoriasis as reflected by maximal PASI scores. There were no differences in the male to female ratio. Among the psoriasis patients, seven (1.7%) were using biological agents and 23 (5.7%) were using immunosuppressive agents.
Demographic and clinical characteristics of the study population
Comparison of smoking status between PsA and psoriasis
The proportions of current smokers and past smokers were higher in the psoriasis patients than the PsA patients (current smokers 26.7% vs 22.3% and past smokers 30.2% vs 23.4%, p=0.001, respectively, table 2). The psoriasis group had also smoked, on average, for more years than the PsA group; however, these results may be attributed to the mean older age of psoriasis patients. There was no difference in the mean number of cigarettes smoked per day between the PsA and the psoriasis group; however, this information was available only for a much smaller sample, particularly in the PsA group (N=217).
Smoking characteristics among psoriasis and PsA patients
Analysis for matched pairs data
We performed an analysis for matched pairs that was aimed at determining whether the association between smoking and PsA was due to trends in smoking in the general population. Of the 404 matched pairs of PsA and psoriasis patients we were able to infer the smoking status at the reference year for 381 psoriasis patients. The results confirmed the inverse association between current smoking and PsA compared with psoriasis patients. In the conditional regression analysis ‘current smoking’ was less common in PsA compared with psoriasis patients (OR 0.57, 95% CI 0.39 to 0.82, p=0.002). In contrast, the prevalence of past smokers was higher in patients with PsA compared with those with psoriasis (OR 1.92, 95% CI 1.2 to 3.07, p=0.007). This change in the direction of the association for the ‘past smoking’ group may be related to the different reference dates considered for the determination of the status of smoking in the analysis presented in table 2.
Multivariate regression analysis
A multivariable logistic regression analysis was performed to adjust for potential confounders (table 3). After adjustment, current smoker compared with life-time non-smoker remained inversely associated with PsA (OR 0.57, 95% CI 0.41 to 0.81), while past smoker versus life-time non-smoker was no longer significant (OR 0.81, 95% CI 0.56 to 1.12). The increase in OR in the ‘past-smoker’ group suggests a confounding effect of one or several of the covariates included in the model. These results were not appreciably changed after the removal of alcohol consumption and psoriasis severity from the regression model to allow the inclusion of patients with missing data in the analysis.
The association between smoking status and PsA* (N=654) compared with psoriasis alone (N=401) by logistic regression analysis, adjusted for age, sex, level of education, alcohol consumption, duration and severity of psoriasis
The interaction between HLA-C*06 and smoking
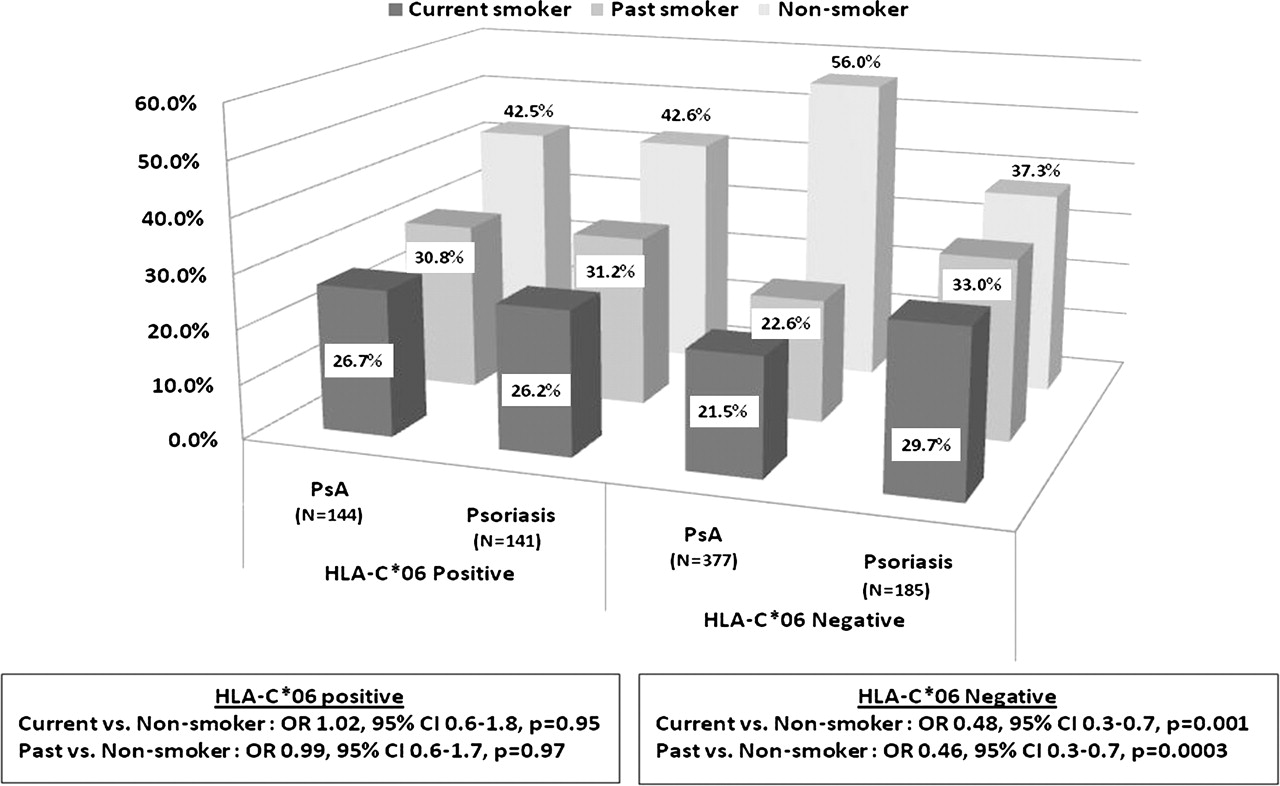
Our group has recently reported that HLA-C*06 was inversely associated with PsA compared with psoriasis patients without arthritis.21 We tested whether the effect of smoking is modified by HLA-C*06 status. Overall 562 PsA and 376 psoriasis Caucasians were included in the analysis. The results are illustrated in figure 1. In a subgroup analysis, the inverse association between smoking and PsA compared with psoriasis was found only among those who were HLA-C*06 negative (current smoking vs non-smoker OR 0.48, 95% CI 0.3 to 0.7, p=0.001 and past smoker vs non-smoker OR 0.46, 95% CI 0.3 to 0.7, p=0.0003). Among those who were HLA-C*06 carriers, there was no significant difference in smoking status between the two groups (current smoker vs non-smoker OR 1.02, 95% CI 0.6 to 1.8, p=0.95 and past smoker vs non-smoker OR 0.99, 95% CI 0.6 to 1.7, p=0.97). The interaction between HLA-C*06 and smoking status was statistically significant in a logistic regression analysis (HLA-C*06-smoking status (ever smoking vs non-smoking) OR 2.1, 95% CI 1.1 to 4.0, p=0.01) suggesting a departure from a multiplicative model.

{kind=link}
Smoking status among psoriatic arthritis (PsA) and psoriasis patients by HLA-C*06 status.
Discussion
In this study we analysed the association between smoking and PsA among patients with psoriasis. The results of the study suggest that active smoking is less common at the time of the diagnosis among PsA patients compared with psoriasis. Furthermore, an interaction between smoking status and HLA-C*06 was identified, as the inverse association between smoking and PsA was present only among patients who were HLA-C*06 negative.
One of the challenges in investigating risk factors for PsA is selecting the appropriate control group. When comparing PsA with healthy controls, it is uncertain whether any significant association is related to the skin or the joint disease. Therefore, psoriasis patients without arthritis comprise a more informative control group. There are few studies that have investigated environmental risk factors for PsA among psoriasis patients. In a study by Pattison et al,22 smoking was less common among patients with PsA compared with those with psoriasis alone; however, it did not reach statistical significance, possibly due to the small sample size. Rakkhit et al 23 found a temporal association between psoriasis, PsA and smoking. They reported that the time to the development of PsA decreases with smoking before psoriasis onset and increases with smoking after psoriasis onset. On the other hand, a recent study from Singapore has found similar proportions of smokers among patients with psoriasis and PsA patients.24 In our study, current smoking was associated with PsA even after adjustment for potential confounders. Previous studies were also limited by a potential misclassification of cases and controls as the exclusion of PsA among psoriasis patients was based on self-report. Misclassification may decrease the power to detect a significant association. One of the strengths of our study is the careful phenotyping of both cases and controls by experienced rheumatologists.
The interaction between genetic and environmental risk factors has received only minimal attention in genetic studies of psoriasis. It has been suggested that HLA-C*06 may modify the effect of smoking and lead to an increased risk of psoriasis of approximately 11-fold over that for non-smokers without HLA-C*06,8 much higher than the combined effect of both risk factors. In this study we analysed the interaction between HLA-C*06 and smoking. We have found that the inverse association between smoking and PsA is present only among psoriasis patients who were HLA-C*06 negative. These results may explain the lack of association between smoking and PsA in studies that recruited the entire study population from dermatology clinics,23 as opposed to our study that enrolled cases and controls from two different sources although within the same centre. By sampling only patients with severe psoriasis, it is likely that the proportion of HLA-C*06 carriers was high, and the studies were thus underpowered to detect an association between smoking and PsA.
There are several limitations to our study that are inherent to a case–control study. First, recall bias is one of the limitations of a retrospective study. In our study, PsA patients had to report their smoking status at the time of the diagnosis, while the psoriasis patients had to report their current smoking status, therefore it is possible that the information about smoking status was less accurate for the PsA patients. However, the information has been collected systematically in all patients upon their first visit to the clinic, which was usually close to the time of the diagnosis of PsA, and in that way minimised recall bias. The reliability of a retrospective report of smoking status at a specific time point has been extensively investigated. It has been shown that people can reliably recall aspects of first tobacco use occurring on average 30 years before the time of assessment.25 Other types of biases in reports of smoking habits are more difficult to control. They may depend on factors such as sociocultural aspects associated with the acceptability of smoking, previous knowledge about the association between smoking and the disease, and on the amount of emphasis that is laid by the investigator on the smoking question. These sources of potential bias are associated with any case–control study and are acknowledged as one of the limitations.
Another potential threat to the validity of the study is related to ecological trends in smoking habits over time, as different reference dates were used for the determination of smoking status. However, given the trend towards a decline in smoking over the past decades,26 the true difference in smokers between the groups may be underestimated. Furthermore, we have confirmed the inverse association between current smoking at the time of the diagnosis and PsA compared with psoriasis in a subset of patients in a matched-pair analysis.
One of the difficulties in designing a case–control study is the selection of an appropriate control group that would reflect the source population from which the cases have originated. In this study, all of the controls had psoriasis and came from the same geographical region as the cases. As most of the patients came from dermatology clinics they reflect a moderate to severe spectrum of the disease. It has been reported that patients with severe psoriasis are at higher risk of developing PsA,24 27 therefore, this group of psoriasis patients serves as an appropriate control group, although the generalisability of the results may be limited. Our study population was well phenotyped and we were able to adjust for differences between the groups in the statistical analysis. However, we are aware that there may be other confounders that were not considered and may explain the differences in smoking prevalence between the two groups.
Finally, we were unable to analyse the exact temporal relation between smoking and the onset of psoriasis and PsA. There were conflicting results with regard to the association between past smoking and PsA compared with psoriasis patients. In the univariate analysis past smoking was less frequent among patients with PsA; however, in the multivariate analysis the association between past smoking and PsA was not statistically significant, while in the matched-pair analysis past smoking was increased among PsA patients compared with psoriasis patients. These differences in the direction of association may be explained by the lag between reference dates used to determine smoking status. We cannot draw conclusions about the effect of smoking cessation on the risk of developing PsA in patients with psoriasis. This question requires a prospective cohort study design with an appropriate statistical analysis.
In summary, in this exploratory case–control study we have found a signal for an inverse association between current smoking and PsA compared with patients with psoriasis alone. Furthermore, our findings support a possible interaction between HLA-C*06 and smoking. Among patients who are HLA-C*06 positive, the association between PsA and smoking was no longer significant. Additional studies that investigate environmental risk factors for PsA and gene–environment interaction are required to confirm our results.
References
Footnotes
-
Funding The University of Toronto PsA programme is supported by a grant from the Krembil Foundation, as well as by the Arthritis Society SPARCC National Research Initiative. LE is supported by a fellowship grant from the Canadian Arthritis Network and an Abbott PsA Fellowship. VC is supported by a Canadian Institutes of Health Research—clinical research initiative fellowship and the Krembil Foundation. RJC holds a Canada research chair in statistical methods for health research.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the university health network research ethics board.
-
Provenance and peer review Not commissioned; externally peer reviewed.