Article Text

Abstract
Objective To provide Swedish nationwide data on the prevalence of rheumatoid arthritis (RA), including variations by age, sex, geography, demography and education level, and assess antirheumatic treatment penetration.
Methods Patients ≥16 years assigned an RA diagnosis were identified from inpatient (n=96 560; 1964–2007) and specialist outpatient care (n=56 336; 2001–2007) in the Swedish National Patient Register, and the Swedish Rheumatology Quality Register (n=21 242; 1995–2007). Data on prescriptions, demography, vital status and educational level were retrieved from national registers.
Results A total of 58 102 individuals (mean age 66 years; 73% women) assigned an RA diagnosis were alive in Sweden in 2008, corresponding to a cumulative prevalence of 0.77% (women 1.11%, men 0.43%). The 2001–2007 period prevalence was 0.70%. Restriction to patients with ≥2 visits or diagnosis from a rheumatologist/internist reduced the overall cumulative prevalence to 0.68%. Whereas urban/rural differences (crude 0.65–1.00%) were explained by age differences, the age/sex-adjusted prevalence remained higher in patients with ≤9 years education (0.86%) than for those with 10–12 years (0.82%) and >12 years (0.65%). Treatment exposures (76% any disease-modifying antirheumatic drugs (DMARDs) or steroids, 64% any DMARD, 15% biological agents) varied with age; use of biological agents decreased from 22% in 16–59 years olds to 3% in ≥80 years olds. Any DMARD use correspondingly decreased from 71% to 43%. Applying age cut-off points from previous northern European and North American prevalence studies reduced or eliminated between-study differences.
Conclusion This nationwide approach yielded a prevalence of RA similar to previous regional assessments. While displaying only modest geographical variation and no urban/rural gradient, prevalence was associated with educational level. Although most patients received antirheumatic drugs, age was a strong treatment determinant.
Statistics from Altmetric.com
Introduction
Despite increasing insights into the aetiology of rheumatoid arthritis (RA), the disease remains a clinical and criteria-guided diagnosis.1 ,2 In clinical practice, rheumatologists assign the RA diagnosis guided by classification criteria, and initiate treatment. Estimates of the prevalence of RA using the American College of Rheumatology (ACR) criteria suggest a range between 0.5% and 1%, with a higher prevalence in women than men, and at older ages.3,–,9
Available prevalence data mostly derive from studies of a limited number of participants in certain geographical areas, and are typically based on fulfilment of classification criteria through detailed scrutiny, and thus not possible to perform nationally.9 Furthermore, neither the widespread 1987 ACR criteria1 nor the recently presented EULAR/ACR RA criteria2 are intended as all-encompassing RA classification schemes but have been developed for specific purposes (creating more uniform trial populations, and identifying patients with early inflammatory arthritis who may benefit from early disease-modifying antirheumatic drug (DMARD) treatment, respectively). Thus, while many existing prevalence studies have the advantage of detailed diagnostic criteria for case ascertainment,9 they may offer limited insights into the prevalence of RA in clinical practice. Larger studies, using more pragmatic RA case definitions, such as doctor's visits with an RA diagnosis or self-reported RA, do, however, exist.10,–,12
It has been suggested that RA incidence decreased during the last decades of the 20th century8 ,13,–,16 but may have increased in the past 15 years.17 ,18 This prompts investigations of the contemporary prevalence, as well as determinants for the reported differences between this and previous Scandinavian,3 ,4 ,19 British5 and North American studies8 ,10 dating 5–25 years back.
Prevalence estimates based on regional or small national samples have indicated potential variations in RA prevalence across ethnic groups11 ,20 and socioeconomic position11; less is known about the variation in RA prevalence across different population segments as defined by geography, urban/rural residence and educational level, from nationwide studies. Similarly, large-scale assessments of treatment penetration in contemporary patients are scarce but important to identify gaps in care.10 ,21
In Sweden, inpatient and specialist outpatient care visits in the universally accessible healthcare system are recorded in the National Patient Register.22 Since Swedish patients with RA typically are diagnosed and treated by rheumatologists, this register may be useful for nationwide prevalence assessments. A clinical quality register for RA provides an additional capture mechanism,22 ,23 while governmental registers on demographics and drug dispensing provide data for analysis of patient segments as defined through, for example, drug treatment and socioeconomic indices.
These national and virtually complete registers are linkable, providing an opportunity to assess the prevalence of RA on a national level, including subgroup variations in prevalence and treatment. The aim of this study was to estimate the contemporary prevalence of RA in Sweden, overall and by age, sex, county of residence, socioeconomic indices (living area, education level), and to estimate the penetration of drug treatments (non-biological DMARDs, biological agents, steroids), on 1 January 2008.
Methods
Patients with a clinical visit listing an RA diagnosis were identified in inpatient and outpatient specialist care in the National Patient Register (1964–2007) together with patients listed in the Swedish Rheumatology Quality Register (SRQ; 1995–2007; online supplementary figure S1).22 Register linkage was performed using each Swedish resident's unique personal identification number. Ethical approval for the study was granted by the Regional Ethics Committee, Karolinska Institutet, Stockholm, Sweden.
The Swedish National Health Service
On 31 December 2007, Sweden had a population of 9.2 million with 7 513 694 (83%) ≥16 years (http://www.scb.se). The Swedish healthcare system is tax funded and offers universal access, while prescription drugs are provided free of charge above a threshold of SEK 1800 annually (≈€180).24 In Sweden, patients with inflammatory rheumatic diseases such as RA are typically diagnosed and treated by rheumatologists rather than by general practitioners. Care for RA represents a mix of combined outpatient and inpatient facilities, with the vast majority of rheumatologists working at hospital-based inpatient and outpatient facilities rather than as private practitioners.
Definition of RA
In the base case analysis, any visit listing an RA diagnosis was used to define RA. In sensitivity analyses, prevalence was calculated according to alternative case definitions based on diagnosis origin (any/rheumatology or internal medicine department), number of visits with an RA diagnosis (any/≥2), use of antirheumatic drugs and a visit in the last 7-year period (2001–2007). Biological and non-biological antirheumatic treatment data were retrieved from the nationwide Prescribed Drug Register and the Swedish Biologics Register ARTIS (online supplementary data).23
Census data, place of residence and education
Data were retrieved from Statistics Sweden to ascertain whether patients were registered in Sweden and alive on 31 December 2007. Data on county and place of residence were also retrieved and categorised using a nine-graded scale employed by Statistics Sweden. The categories include main cities (Stockholm, Gothenburg and Malmo), larger cities, suburbs of the main cities, commuting areas, industrial areas, sparsely populated areas and three types of other areas defined by their population size (>25 000, 12 500–25 000, <12 500).
Education level was categorised into ≤9, 10–12 and >12 years of schooling. As no population statistics were available on education level in 2007 for individuals ≥75 years at http://www.scb.se, and many 16–29-year-old people may not have completed their education, the education level analyses were restricted to the 30–74 years age range.
Statistics
Data were analysed using SAS (version 9; SAS Institute, Cary, North Carolina, USA). Prevalence was calculated overall, by sex, age, place of residence, county and education level. For prevalence by place of residence, county and education level, both crude and standardised estimates were computed (standardised to the age and sex distribution in the Swedish general population). To facilitate between-study comparisons, prevalence calculations were also performed using age restrictions employed in previous studies.3,–,5 ,8
Results
During the study period a total of 123 363 patients with at least one hospital admission or outpatient visit listing an RA diagnosis were identified from the register sources, excluding patients with juvenile disease onset. Of these, 58 102 patients were alive and registered in Sweden on 1 January 2008 (ninpatient=32 777, noutpatient=48 644; nSRQ=18 201). Sixty-nine per cent of all patients were ≥60 years in 2008 (mean age 66 years; SD 15) and 73% were women. Large overlap was seen between the register sources for prevalent patients, with the SRQ Register adding only 702 patients (1.2%) not identified in the National Patient Register (supplementary figure S1).
Prevalence of RA
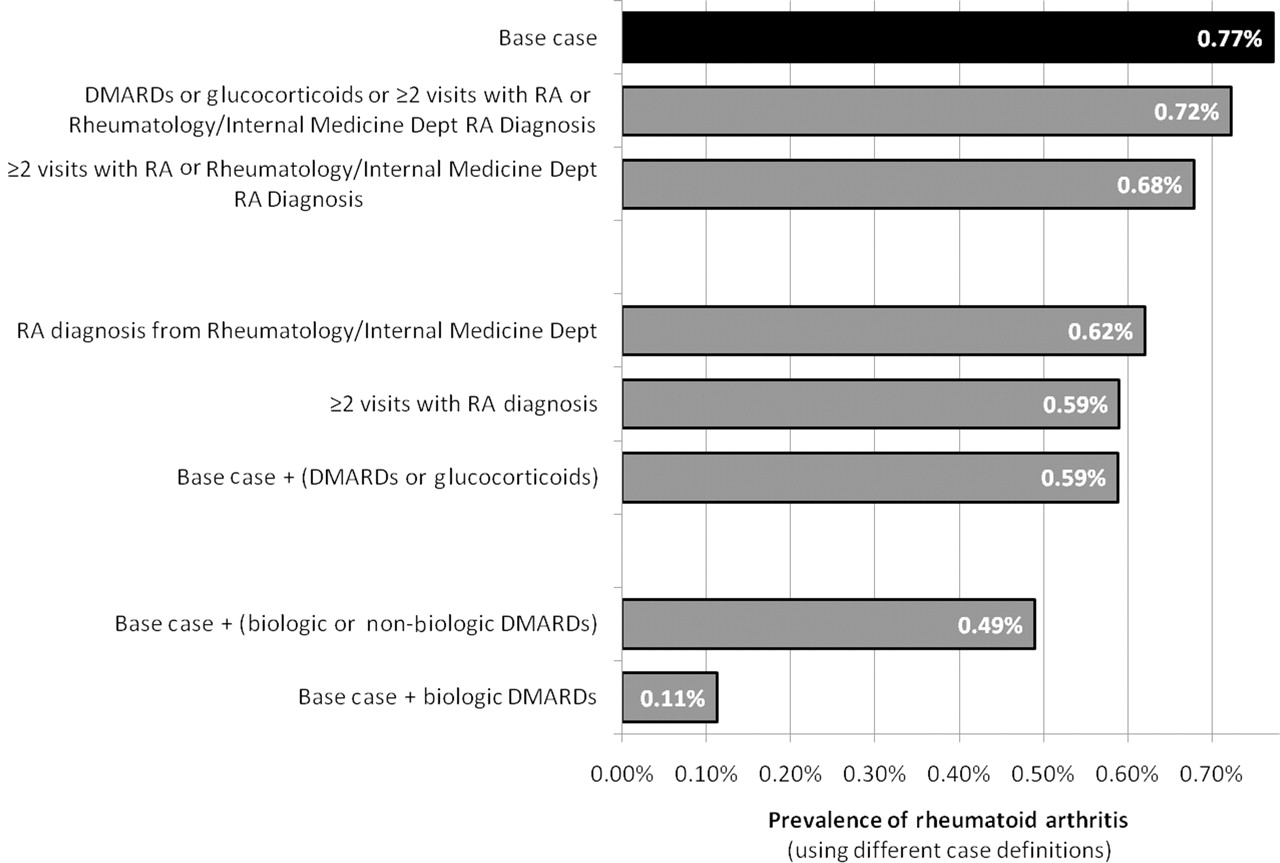
The base case nationwide cumulative prevalence of adult onset RA in 2008 was 0.77% (58 102/7 513 694). The robustness of this estimate is shown in figure 1 with resulting prevalence when additional criteria were required to be fulfilled (sex-stratified in supplementary figure S2). The prevalence estimate was only marginally affected from the base case (0.77% to 0.72%) if requiring either of ≥2 visits, diagnosis from a rheumatology/internal medicine department, or antirheumatic drug use. The prevalence estimate changed to 0.68% when the analysis was restricted to patients with ≥2 visits listing an RA diagnosis or diagnosis from a rheumatology/internal medicine department.

Prevalence of rheumatoid arthritis (RA) using different criteria for case ascertainment. Biological disease-modifying antirheumatic drugs (DMARDs): etanercept, adalimumab, infliximab, rituximab, abatacept, anakinra (from the Swedish Biologics Register ARTIS, 1999–2007, and the Prescribed Drug Register: 2005–2007). Non-biological DMARDs: methotrexate, sulfasalazine, leflunomide, azathioprine, antimalarial agents (ATC P01B), gold (ATC M01CB01), ciclosporin (from the Prescribed Drug Register, 2005–2007). Population base: 7 513 694 people ≥16 years registered in Sweden 31 December 2007 (http://www.scb.se). Sex stratified data shown in online supplementary figure S2.
Women had a higher prevalence than men in all age groups, but the prevalence ratio decreased from 3.6 (95% CI 3.1 to 4.3) in the youngest to 1.8 (95% CI 1.7 to 1.9) in the oldest age group (figure 2; overall prevalence ratio 2.3 (95% CI 2.3 to 2.4)).

Prevalence of rheumatoid arthritis (RA) in Sweden by age (1 January 2008; n=58 102). Cases defined as ever having a visit in inpatient or outpatient specialist care with a diagnosis of RA, or a listing in the Swedish Rheumatology Quality Register.
Antirheumatic treatment penetration
Of all prevalent patients in 2008, 76% had been treated with biological agents, non-biological DMARDs or glucocorticoids in the previous 3-year period (table 1).
Antirheumatic drug treatment in patients with any visit for rheumatoid arthritis
The penetration of biological agents was 15% in the base case (18% if requiring ≥2 visits with an RA diagnosis, 17% if requiring diagnosis from a rheumatology/internal medicine department, and 16% if requiring either one of these criteria). The corresponding percentages for any DMARD treatment were 64% (base case), 74%, 71% and 69%, respectively.
Use of biological agents (base case definition of RA) was strongly associated with age, with a penetration of 22% in the 16–59 year (3854/17 808), 18% in the 60–69 year (2922/15 849), 10% in the 70–79 year (1359/13 509) and 3% in the ≥80 year age group (373/10 936; supplementary figure S3). When two or more visits with an RA diagnosis or diagnosis from a rheumatology/internal medicine department were required, the corresponding penetration levels were similar (24%, 20%, 11% and 4%). Marked geographical variation in penetration of biological agents was also observed, with a twofold variation across counties, as described elsewhere.21
For any DMARD treatment (biological or non-biological) there was also an age gradient, with the penetration decreasing from 71% in 16–59 year (12 655/17 808), 71% in 60–69 year (11 240/15 849), 63% in 70–79 year (8539/13 509), to 43% in ≥80 year old patients (4669/10 936). The penetration levels were similar if requiring two or more visits with an RA diagnosis or diagnosis from a rheumatology/internal medicine department (76%, 75%, 68% and 48%).
Period prevalence 2001–2007
Of all identified patients, 91% of the base case cohort had at least one visit listing RA between 2001 and 2007, resulting in a period prevalence of 0.70% (52 612/7 513 694). Of patients ≥80 years old, 83% had a visit recorded in the selected period. Among those with at least one visit during 2001–2007, the overall biological agents penetration was 16% and the DMARD penetration 69%.
Place of residence and county
The crude overall prevalence of RA increased from a low of 0.65% in the most urban areas to a high of 1.00% in the most sparsely populated areas of Sweden (figure 3). A consistent positive gradient was seen from more to less urban areas. After standardising the estimates to the population age and sex distribution, the range decreased to between 0.73% and 0.86%. No clear north–south or east–west gradients could be seen either before or after age standardisation (supplementary figure S4).

Prevalence of rheumatoid arthritis by place of residence (n=58 102; nationwide prevalence 0.77%; 1 January 2008).
Education level
After age adjustment, the education level distribution was similar for the general and the RA population in 30–74 year olds: 20% vs 22% ≤9 years, 46% vs 49% 10–12 years and 33% vs 29% >12 years education. The age- and sex-standardised prevalence of RA was highest, intermediate and lowest in population segments with ≤9 years (0.86%), 10–12 years (0.82%) and >12 years of schooling (0.65%), respectively. The gradient was most pronounced in the oldest patients (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of rheumatoid arthritis by education level and age (n=39 551). No population statistics on education level for people aged ≥75 years; 15–29-year-old people excluded as many may not have completed their education.
Age restrictions
Restricting the analysis to ages 20–74 years as in a previous Swedish study that only provided an overall estimate (0.51%),4 the prevalence was 0.65% (supplementary figure S5). Restricting the analysis to 20–79-year-old patients as in a previous Norwegian study (prevalence 0.44%)3 yielded a prevalence of 0.72%. Lastly, when restricting the analysis to 35 years and older, as in a previous American study (prevalence 1.07%),8 we estimated a prevalence of 1.06%.
Discussion
Our base case nationwide cumulative prevalence estimate in Sweden was 0.77% (2001–2007 period prevalence 0.70%). The estimate was surprisingly robust when adding stricter criteria, such as multiple visits with an RA diagnosis, diagnosis from a rheumatologist or internist, and/or antirheumatic drug treatment. Apart from the expected age and sex gradients, the data indicate that (1) there is a spurious urban/rural gradient of RA with higher prevalence in rural areas reflecting demographic differences rather than true variations; (2) there is no clear north/south gradient in Sweden (spanning 14° latitude); (3) prevalence may be higher in groups with lower education; (4) considerable age differences in treatment penetration exist, with 22% and 71% of 16–59 year old patients receiving biological agents and DMARDs, respectively, compared with 3% and 43% in ≥80-year-old patients and (5) a large part of the between-study variation in prevalence may come from differences in age cut-off points rather than true prevalence variations.
Previous northern European RA prevalence estimates have varied between Sweden (0.51%), Norway (0.44%) and the UK (minimum 0.81%).3,–,5 In 1995, Simonsson et al4 used a postal survey (response rate 62%) in the Swedish county of Halland, followed by clinical examinations. Compared with our study, their design was more likely to capture patients cared for by general practitioners, as well as undiagnosed patients, and less likely to include false positives. Despite this, their estimate was lower than ours (20/3928=0.51% vs 58 102/7 513 694=0.77%). Half of this difference was explained by their age restriction (20–74 years; supplementary figure S5). Eleven per cent of the adult Swedish population was ≥75 years in 2007, and with a prevalence of 2.2%, they constituted 30% of all patients with RA we identified. Excluding this group reduced our estimate from 0.77% to 0.65%.
In 1994, Kvien et al3 assessed the prevalence of RA in 20–79-year-old Norwegians in Oslo county using a hospital register listing patients from 1991 (n=1333) and a postal survey to 10 000 inhabitants (response rate 59%). Their register-based prevalence estimate was 0.44%. Their lower prevalence was also partly explained by exclusion of the oldest (supplementary figure S5). Using their age restriction reduced our prevalence estimate from 0.77% to 0.72%.
In 2000, Symmons et al5 assessed the prevalence of RA in ≥16 year olds in Norfolk using a postal survey (response rate 82%) followed by clinical examinations of positive responders (80% examined). They reported a minimum prevalence of 0.81% (women 1.16%, men 0.44%)—that is, similar percentages as in our study (0.77% overall, women 1.11%, men 0.43%). Their age-specific estimates were, however, consistently higher for both women and men ≥45 years (supplementary figure S6).
It has been suggested that the RA prevalence is significantly higher in North America than northern Europe, based on a comparison with one single US study.8 ,9 Using the same age restrictions (≥35 years) as Gabriel et al used on 425 patients with ACR-criteria classified RA in 1985 in Rochester, Minnesota,8 we found the same prevalence in Sweden (1.07% vs 1.06%). This age-group prevalence was, however, reported to have decreased to 0.85% in 1995.7 In a recent study of ≥18 years olds in Olmsted County, Minnesota, the prevalence was reported to have increased from 0.62% to 0.72% from 1995 to 2005 based on 466 patients with RA.17
Between 1996 and 2000, Lacaille et al used administrative billing data in British Columbia to identify all patients with two or more visits with RA.10 They found a cumulative prevalence of 0.76% compared with 0.68% in our study (requiring ≥2 visits with RA), and a DMARD penetration of 43% compared with our 74%. Another regional register-based study found a prevalence of 0.68% in ≥20-year-old Swedes, with lower prevalence (vs our current study) in ≥80 years olds (women: ≈1.5% vs 2.7%; men: ≈1.0% vs 1.5%) possibly owing to study design differences.12 A prevalence estimate of 0.8% has also been reported in 1993 for ≥16-year-old Finns.19 Much lower prevalence estimates have been reported from South America, southern Europe and Asia.9
Social deprivation and education level have been suggested to influence the prognosis of RA.25 ,26 None of the previous Scandinavian, US or Canadian studies stratified their estimates by social deprivation, while Symmons et al5 could not find any association between living area (within Norfolk) and prevalence. Similar to Symmons et al,5 we found only small differences by place of residence (within Sweden) after age and sex standardisation. We did find indications of an association with education level, at least in older age groups, as did Rasch et al in the USA.11 If true, this might be partly explained by the higher smoking prevalence associated with lower socioeconomic status.27
Prevalence studies based on a limited number of participants from a defined area offer the possibility to investigate the contribution of specific classification criteria to the estimated prevalence.5 However, they will not be 100% sensitive to the disease as defined in clinical practice, and offer only limited insights into geographical, urban/rural and socioeconomic variations, or burden of disease as indicated by medication use. The register-based approach employed in our study offers this possibility. A limitation of this register-based approach pertains to the specificity and the sensitivity of the RA capture mechanism. Using the ACR criteria as reference, a false-positive rate of around 10% has been documented in the inpatient section28 and 6–15% in the outpatient section of the National Patient Register (Geborek P, personal communication, and Knight et al29). This leads to overestimation of the prevalence while underestimation may occur if patients are solely treated by general practitioners, or remain undetected. Regarding specificity, we performed analyses using stricter criteria—for example, requiring two or more visits or diagnosis from a rheumatology/internal medicine department. Combined these resulted in an estimate of 0.68%. Regarding sensitivity, most patients with RA are treated by specialists, and private care is uncommon as well as partly covered by both the National Patient and the SRQ Registers. Although regional Swedish data from Skåne show that patients can be found with listings of RA in primary care only, the number is small (≈10% of the total number of patients with RA) and the diagnostic accuracy of such listings remains to be confirmed (Englund M, personal communication).
The recently presented ACR/EULAR2 classification criteria for RA will definitely lead to a change in the time point of fulfilment of the criteria for RA (compared with the ACR criteria). The extent to which they will also have an impact on the cumulative prevalence of clinical RA diagnoses at a population level (as reported in this study) is more difficult to predict, although their impact in the short term is likely to be limited. Nevertheless, the new criteria call for new assessments of RA incidence, as well as RA occurrence (cumulatively and at given time points).
A strength of this study was the availability of nationwide data on inpatient and specialist outpatient care visits, as well as antirheumatic treatment. Using these routinely collected data, prevalence of RA and its treatment is easily estimated, and the large sample size allows for subgroup analyses. The RA capturing mechanism was further strengthened by data from the SRQ Register, although it only contributed 1% of unique patients, indicating a high degree of capture of RA by the National Patient Register.
Another strength was that we did not rely on questionnaires followed by clinical examinations. Symmons et al5 noted that response varied by age, sex and affluence of the residential area, variables which may be associated with RA. Patients with severe disease may also have problems attending clinical examinations, adding to the risk of selection bias. On the other hand, we did not confirm the RA diagnosis through clinical examination, possibly leading to misclassification, nor did we have a chance to capture people who had never presented to outpatient or inpatient care, possibly leading to underestimation.
In summary, while broadly confirming previous prevalence estimates from smaller studies, our study extends these with estimates for subgroups based on urban/rural, geographical and educational background. Despite indications of possible changes in incidence, and despite the observed gradients with educational level, the prevalence of RA appears surprisingly consistent, both within Sweden and across countries. By contrast, even slight differences in age cut-off points underlie a large portion of the difference in reported prevalence. Among contemporary patients with RA, age was identified as a strong determinant for antirheumatic drug treatment.
Acknowledgments
The authors would like to thank all rheumatologists contributing data to the Swedish Rheumatology Quality Registers, and Elizabeth Arkema for language revision.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
-
The ARTIS study group (in alphabetical order) E Baecklund, L Coster, C Dackhammar, N Feltelius, P Geborek, L Jacobsson, L Klareskog, S Lindblad, S Rantapaa-Dahlqvist, T Saxne and R van Vollenhoven.
-
Funding For the maintenance of the register, the Swedish Society for Rheumatology has received funding, independent of the conduct of these scientific analyses, from Schering-Plough, BMS, Wyeth, Abbott Laboratories and Roche.
-
Competing interests The ARTIS Study Group conducts scientific analyses using data from the Swedish Biologics Register ARTIS run by the Swedish Society for Rheumatology.
-
Ethics approval This study was conducted with the approval of the Regional Ethics Committee, Karolinska Institutet, Stockholm, Sweden.
-
Provenance and peer review Not commissioned; externally peer reviewed.