Article Text

Abstract
Inflammation of synovium is one of the hallmarks of rheumatoid arthritis (RA). Analysis of synovial tissue has increased our understanding of RA pathogenesis, aided in identifying potential therapeutic targets and has been used in the response and mechanistic evaluation of antirheumatic treatments. In addition, studies are ongoing, aimed at the identification of diagnostic and prognostic biomarkers in the synovium. This paper outlines the currently used procedures for sampling and processing of synovial tissue, and presents a standardised recommendation to support multicentre translational research.
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is characterised by chronic inflammation of the synovium, leading to invasion of synovial tissue into the adjacent cartilage matrix and bone. This in turn results in joint destruction, deformity and disability, and thus severe morbidity.1 Analysis of synovial tissue has increased insight into RA pathogenesis, aided in identifying potential therapeutic targets and has been used in the evaluation of current and new antirheumatic treatments.2,–,19 Moreover, present studies are addressing the question as to whether synovial biomarkers might be used as diagnostic and prognostic markers in patients with early arthritis.
During the past 15 years investigations of the changes in synovium after experimental antirheumatic treatment have increased. Drug development is an expensive process and financial resources to evaluate therapeutic effects of new compounds are restricted. Clinical outcome measures often require a long follow-up time and large patient cohorts, but the number of eligible patients with active disease available to participate in clinical trials is usually limited. Ethical considerations may also minimise the number of patients who may either be exposed to placebo or put at risk with new experimental drugs in an early stage of drug development. It is also expected that the number of new compounds to be tested will markedly increase in the next decades. Therefore, an alternative approach of testing based on relatively small proof-of-principle studies is essential. This has led to the concept of small, high ‘density of data’ clinical trial designs that include synovial biomarkers to facilitate ‘go/no-go decisions’ in an early stage of drug development.19
Biomarkers are characteristics that can be objectively measured and evaluated as an indicator of normal biological or pathological processes, or pharmacological responses to a therapeutic intervention.20 21 Immunohistological features of rheumatoid synovial tissue, in particular macrophage infiltration as well as expression of tumour necrosis factor α (TNFα) and interleukin 6 (IL-6), correlate with measures of disease activity, independently of disease duration.22 By including synovial biomarkers it may be possible to diminish the time and the number of patients needed to screen for the potential efficacy of new compounds.19 23 For example, we have shown that the absolute number of macrophages in the synovial sublining is a highly sensitive measure of change after effective treatment of RA (which is independent of the compound's primary mechanism of action) and correlates well with clinical improvement.24,–,30 Measurement of synovial macrophages has proved to be a reliable tool to screen for local biological effects in early-stage drug development for RA and is less susceptible to placebo effects than clinical evaluation.19 In addition, examination of serial synovial biopsy samples may provide insight into the specific mechanism of action of given therapeutic agents.
Most data are available for clinical trials in patients with RA, but preliminary results suggest that this approach might also be used in, for instance, psoriatic arthritis.31 Identification of new biomarkers in synovium by gene-expression profiling is currently under development.32,–,34
For multicentre translational research, standardisation of methodology is an essential prerequisite. Here, we review the current procedures for sampling and processing of synovial tissue, and present a standardised recommendation for clinical trials.
Methods of synovial tissue collection
Synovium is easily accessible for biopsy. Currently, three percutaneous, minimally invasive methods for synovial tissue collection are available: blind needle biopsy, ultrasound-guided biopsy and arthroscopic biopsy.35
Blind needle biopsy
Blind needle biopsy is a safe and technically simple method that can be performed in most rheumatology clinics. Special biopsy facilities are not required and it is quite inexpensive. This procedure is mainly performed in the suprapatellar pouch of the knee joint using a Parker–Pearson or Williamson–Holt needle under local anaesthesia.36 37 Multiple samples can be obtained from different locations within the suprapatellar pouch, as well as other joints, such as the shoulder, elbow, wrist and ankle, and with a modified needle even in small finger joints.37
Synovial biopsy samples obtained with a blind needle from clinically inflamed joints correlate well with those taken under vision with arthroscopy38 and in most cases adequate synovial tissue samples can be collected.37 We have performed over 800 biopsies using the Parker–Pearson technique without complications, such as haemarthrosis or infection; sufficient samples were obtained in 85% of the patients.39 Failures occurred mainly in clinically quiescent joints, illustrating the most important limitation of this method. Based on these results it is not advisable to use blind needle biopsy for serial sample tissue collection in clinical trials evaluating therapeutic compounds and it should be reserved for diagnostics or cross-sectional synovial tissue analysis.
Ultrasound-guided biopsy
Ultrasound-guided biopsy is a fairly new technique, which can be performed in both small and large joints, bursae and tendon sheaths under local anaesthesia.40 Under indirect visual inspection this approach allows for collection of sufficient inflamed synovial tissue samples, and has proved to be reliable for histopathological assessment.41 The ultrasound is used to select the best biopsy site based on synovial proliferation and vascularisation (using Doppler mode), after which synovial tissue is acquired percutaneously using a portal and a forceps.40 Although the portal is fixed, a long, semirigid or flexible forceps ensures sampling from all joint compartments.42
Ultrasound features, such as power Doppler and grey-scale scoring recorded before and during the procedure, can guide the operators to the best sampling sites. Power-Doppler positivity identifies areas with an increased amount of subsynovial infiltration of polymorphonuclear cells and surface fibrin indicating an active synovial inflammation. Nevertheless, absence of a positive power-Doppler signal does not exclude the possibility of synovitis.43 By grey scale, the thickness of the synovial tissue can be evaluated as well as the presence of large villous synovial extroflexions. Ultrasound evaluation is more sensitive than clinical scoring in identifying affected joints in multiple clinical settings (active or subclinical disease of different joints)44,–,46 and is therefore a useful additional tool for choosing the most suitable joint for biopsy, regardless of the technique used to sample it.
This technique is patient friendly, but does have some drawbacks. First, as bony surfaces, such as the patella, might cause ultrasonic interference, this can limit the access area, especially in clinically quiescent joints. Data on sample collection in clinically unaffected joints or in series are as yet not available. Furthermore, evaluations of the safety or validity of samples collected for laboratory techniques other than histopathology and immunohistochemistry (quantitative PCR (qPCR), cell culture, etc) have not been performed. Thus, although this method is appealing, further validation is needed.
Arthroscopic biopsy
Arthroscopic biopsy is safe and well tolerated.39 47,–,51 It is relatively inexpensive, although the costs are significantly higher than for blind needle biopsy, because of the specific training and designated biopsy facility needed to perform arthroscopies.49 The procedure is performed under local anaesthesia with a small-bore arthroscope. Synovial inflammation is visualised and several joint areas are systematically inspected, after which tissue samples can be taken from different sites. In the knee, samples are obtained from the suprapatellar pouch, medial and lateral gutter, patellar gutter, tibiofemoral junction and patellar rim. This procedure can be performed in swollen and non-swollen knee, ankle, wrist and metacarpophalangeal joints.52,–,54 Arthroscopy has a low complication rate. Minimal pain or discomfort during the procedure was reported by 35% of 150 patients with knee synovitis. Minor complications, such as vasovagal reactions and temporary swelling of the joint, were mentioned in less than 10% of the cases.47 In a survey, in which information from 15 682 arthroscopies performed by rheumatologists was collected, the complication rate of haemarthrosis was 0.9%, deep vein thrombosis 0.2% and wound and joint infection both 0.1%.49
Although arthroscopy is more expensive and specific training is needed, it is currently considered the ‘gold standard’. It is possible to sample synovial tissue from different areas in the joint and because of direct vision this method yields adequate samples even in quiescent joints. When synovial biopsy specimens are taken during arthrotomic surgery, serial sampling for evaluation of antirheumatic treatment is rarely possible,40 but this is attainable using an arthroscopic technique. Of importance, inflammation in one inflamed joint is generally representative of that in other inflamed joints54; in clinical trials, serial biopsy samples are obtained from the same joint to minimise variability.
Collecting biopsy samples: location in the joint and number of specimens
The rationale for synovial tissue analysis is based on the assumption that changes seen in samples truly represent the inflammatory processes active in the joint and that they correlate with the systemic disease process. It has been suggested that mediators of inflammation and joint destruction might be differently expressed within the joint, especially between the cartilage–pannus junction (CPJ) and the non-CPJ region. However, various studies have shown similar results between CPJ and non-CPJ synovial tissue for T cells,55 56 plasma cells,56 and several matrix metalloproteinases56 57 and granzymes.56 The observations for synovial macrophages are divergent: some studies did not find a difference,55 56 whereas another did.38
In general, sampling tissue only from a small area may result in an overestimation or underestimation of inflammation due to morphological heterogeneity of synovium.58 Hence, to overcome sampling error, a sufficient number of tissue samples from different locations within the joint is required. We advise evaluating samples from at least six to eight different sites within the joint. This allows for a reliable score for T-cell infiltration and activation markers with <10% variance59 and detection of twofold differences in gene expression as measured by qPCR.60 Similar results were recently obtained for ultrasound-guided biopsy.41
Although the knee is an easily accessible joint, in clinical studies evaluating synovial tissue it is often impossible to solely include patients with an actively inflamed knee joint, as this might not be affected at the time. In that case we recommend obtaining serial biopsy samples from another, relatively large, clinically affected joint, such as the ankle or wrist.
Recommendation for arthroscopic and ultrasound-guided synovial biopsy in the knee joint
Based on the experience of different partners involved in the European League Against Rheumatism Synovitis Study Group and the aforementioned studies, we present a consensus statement on synovial tissue collection and subsequent handling that can be used as a guideline for future research. We will describe synovial biopsy of the knee as this joint has easy access and an inflamed knee joint is microscopically representative of other clinically affected joints. The same principles apply to biopsy of other joints with some minor modifications.
Synovial tissue sample collection by arthroscopic biopsy
To perform arthroscopies clinicians have to be welltrained and a dedicated arthroscopy room needs to be available.49 Required instruments are shown in figure 1. Contraindications, such as anticoagulant use, haemostatic disorders, cutaneous lesions and allergies, should be ruled out beforehand.
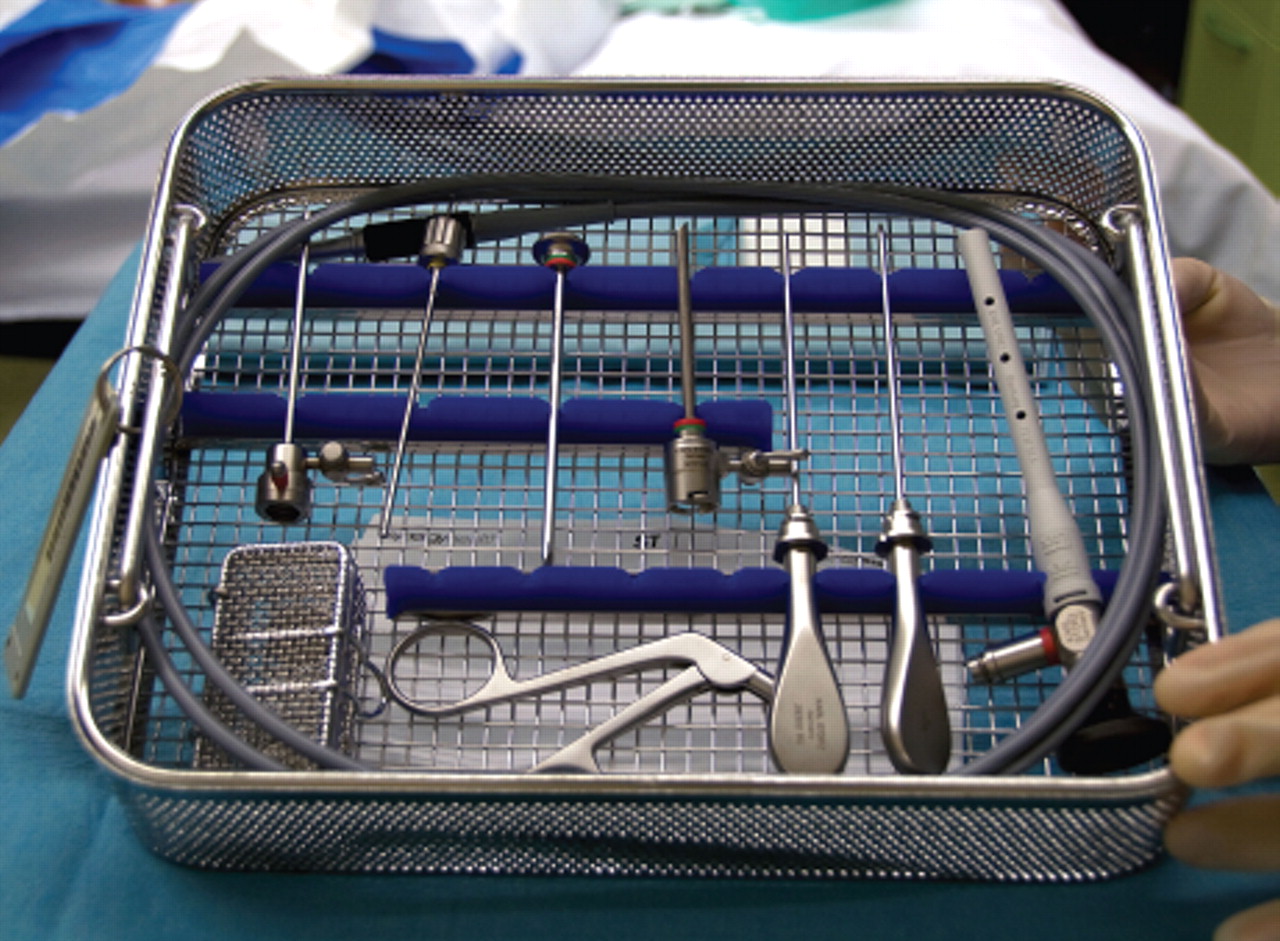
Arthroscopic synovial biopsy instruments. Standard knee arthroscopy set consisting of (left to right): 3.2 mm arthroscope sheath (infrapatellar portal), 2.3 mm rigid grasping forceps, sharp obturator (suprapatellar portal), 3.9 mm biopsy portal (suprapatellar portal), sharp obturator/metal handle (infrapatellar portal), blunt obturator/trocar (infrapatellar portal), 2.4 mm wide-angle Hopkins 30° arthroscope. This also includes a 2.5 mm fibre optic light cable and an automatic valve.
For the procedure the patient will lie down on his back on a trolley or operating table. The patient may be screened from the field of operation or provided with a face mask and cap, and the whole procedure is undertaken under sterile conditions. After skin disinfection with iodine (performed twice, starting from the point of incision up to 25 cm proximally and distally) the patient is covered with sterile draping.
Arthrocentesis of the knee joint is performed using the lateral suprapatellar portal and local anaesthetic (20 ml lidocaine 1% or 10 ml marcaine 0.5%) can be injected intra-articularly via the same needle. First, the joint capsule, subcutaneous tissue and skin are infiltrated with 10 ml lidocaine 2% at the sites, where the lateral suprapatellar and lateral infrapatellar portals will be placed. After a skin incision of 0.5 cm just laterally below the patella, the trocar with obturator is introduced into the joint cavity via this lateral infrapatellar portal. The obturator is withdrawn and replaced by the rod-lens needle scope connected to the camera to allow inspection of the joint. An irrigation system with a three-way stopcock is connected to the camera; this is used for joint lavage (10 ml lidocaine 1% per litre saline). A second incision of 0.5 cm above the patella provides space for the lateral suprapatellar portal, where the trocar with obturator is introduced for outflow of irrigation fluid and synovial tissue biopsy sampling.
When all instruments are in place the five different regions (suprapatellar pouch, medial and lateral gutter, tibiofemoral junction and CPJ) are systematically inspected with special attention paid to synovial tissue covering the cartilage, the amount of vascularisation and villous formation. Biopsy samples are taken from at least six to eight different sites within the joint (for each analysis method—such as immunohistochemistry, qPCR, microarray, etc) with a 2.3 mm grasping forceps, starting at the suprapatellar pouch, going down via the medial gutter, towards the infrapatellar region, the tibiofemoral region and, finally, the CPJ near the patellar rim (figure 2). All specimens are placed on a non-woven, wet (0.9% saline) gauze and each set of at least six is prepared for storage by a laboratory technician (for further sample handling, see below).

{kind=link}
{kind=link}
Knee arthroscopy. Synovial tissue biopsy using a small-bore arthroscope (infrapatellar portal) and grasping forceps (suprapatellar portal).
When the biopsy is complete, irrigation is continued until the irrigation fluid drained from the joint is clear. The suprapatellar portal is removed and 10 ml marcaine 0.5% (or bupivacaine 0.25–0.5%) may be injected intra-articularly via the infrapatellar portal for prolonged anaesthesia, after which the infrapatellar portal can be removed. Both incision sites are closed with Steri-Strips, surgical clips, nylon 3.0 sutures or Ethilon 4.0 sutures, if necessary.
The skin is cleaned with alcohol and sterile gauze dressing is laid over the incisional wounds. An elastic stocking is placed around the knee, which can be worn during the first day. Instructions are given about restrictions in daily activities and suspicion of complications. If sutures are used, they should be removed 1 week after the arthroscopy.
Ultrasound-guided synovial biopsy
Although the arthroscopic approach is at present most commonly used, we have included details for the ultrasound-guided biopsy procedure of the knee joint as well. An ultrasound machine with a multifrequency linear transducer and power-Doppler mode is needed and the same sterile precautions and procedures for disinfection, as described for the arthroscopic biopsy above, are employed. Using the ultrasound view, the best point of entrance for the portal is identified, usually on the lateral margin of the suprapatellar recess, which helps to eliminate ultrasonic interference from the cortical margin of the patella. The skin, subcutaneous tissue and joint capsule are anaesthetised with 10 ml lidocaine 2%. Next, a 14 gauge (2.2 mm) catheter needle with a steel wire is inserted into the joint, followed by a 7 F (2.3 mm) percutaneous sheath introducer led intra-articularly by the wire. Through this guide the portal is placed in position. The sheath introducer is removed, after which a forceps can be introduced through the portal. All steps are performed under ultrasound vision. This portal is connected to an irrigation system with a three-way stopcock for joint lavage during the procedure. Regions of synovial hypertrophy are identified under grey-scale and power-Doppler guidance and both a 2.0 mm rigid and a 2.3 mm longer, flexible forceps are used to ensure sampling of representative tissue from all joint compartments (suprapatellar, medial and lateral). A total of six to eight specimens for each analysis technique is obtained and placed on a non-woven, wet gauze. Irrigation is continued until the joint fluid is clear; no sutures are needed for the point of entrance. As described for the arthroscopic technique, the skin is disinfected, a compression bandage is worn by the patient during the first day and postbiopsy instructions are given.
Biopsy samples handling
Biopsy samples are collected on non-woven, wet gauzes and processed promptly by the laboratory technician depending on the method of further analysis.
Tissue samples are fixed in formalin for 24 h, embedded in paraffin and stained with haematoxylin/eosin for routine histology. For immunohistochemistry, eight specimens are stacked together on the bottom of a mould, which is immediately filled with Tissue-Tek optimum cutting temperature (OCT) compound. This is placed in a labelled cryotube and left at room temperature for 2 min for embedding of the tissue. The cryotube is snap frozen in liquid nitrogen for 1 min until the compound turns white and the tubes are stored in liquid nitrogen awaiting further processing.
For PCR, microarray, ELISA or proteomics, samples are usually directly placed in a labelled cryotube, snap frozen and stored in liquid nitrogen. For reliable RNA expression in synovial tissue, it is important to minimise the time between sample acquisition and snap freezing, as RNA is quickly degraded. For RNA isolation, fresh tissue can also be placed directly in RNALater Tissue Protect Tubes containing 1.5 ml RNALater and kept at 4°C overnight (minimum of 16 and maximum of 24 h). The next day, RNALater is removed using a pipette without disrupting the sample, and the tubes containing the samples are transferred to a −80°C freezer; they should not be stored in liquid nitrogen. For PCR and microarray analysis, results depend on the composition of the individual populations of cells present.34
For primary cell culture, synovial tissue samples are directly placed in suitable culture medium, such as serum-containing Dulbecco's modified Eagle's medium (DMEM). Cells are either allowed to grow out of the tissue lump or released from it by enzymatic digestion. Synovial cell populations are then cultured at 37°C in a 5% CO2 incubator.
Whole tissue synovial explant ex vivo cultures can also be established.61 62 This system maintains the synovial architecture and cell–cell contact of the synovium and, therefore, reflects more closely the inflamed joint environment. These cultures release proinflammatory cytokines spontaneously and have been used for proof-of-concept studies testing potential therapeutic targets. To establish explant cultures each biopsy specimen, or sections thereof, is placed in full, serum-containing DMEM or RPMI 1640 medium in 48-well or 96-well plates. The tissue is cultured in the absence or presence of inflammatory stimuli, such as TNFα or IL-1β, at 37°C in a 5% CO2 incubator. After incubation, cell-free supernatants are harvested for quantification of proinflammatory mediators and the wet weight of each tissue section is measured. Samples are either snap frozen and used for RNA isolation or OCT embedded for histological analysis.
If indicated, the presence of urate crystals can be detected by polarisation microscopy in unstained paraffin sections. If a bacterial infection is suspected, synovial tissue samples can be examined by histology, Gram staining, culture and PCR.63
Conclusion
Here, we have provided a standard operating procedure for the synovial tissue biopsy process (collection and handling of tissue samples) to be used in multicentre clinical trials and other forms of multicentre translational research. Although we have mainly focused on RA, this guideline can also be used for studies of other inflammatory joint diseases, such as spondyloarthritis and (inflammatory) osteoarthritis.
In addition to clinical outcome measures, response to treatment can be evaluated by comparing the presence or expression of biomarkers in synovium, such as macrophages in the synovial sublining. Furthermore, synovial biomarkers can be used in dose-finding studies or to stratify patient groups.
This recommendation offers a first step in standardising procedures for innovative, proof-of-principle clinical trials. Standardisation of immunohistochemistry, quantification of immunohistochemical staining, and gene and protein expression in synovial tissue are critical as well.
References
Footnotes
-
Funding This research was supported by the European Community's FP6 funding (AutoCure) and the Dutch Arthritis Association (Reumafonds), the EULAR Synovitis Study Group and the OMERACT Special Interest Group on Synovial Analysis in Clinical Trials. SA, VC, IF and EV-S participated in the University of Glasgow/Academic Medical Center-University of Amsterdam Inflammatory Arthritis Fellowship sponsored by NovoNordisk.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.