Article Text

Abstract
Cryopyrin-associated periodic syndrome (CAPS) is a rare, heterogeneous disease entity associated with NLRP3 gene mutations and increased interleukin-1 (IL-1) secretion. Early diagnosis and rapid initiation of IL-1 inhibition prevent organ damage. The aim of the study was to develop and validate diagnostic criteria for CAPS. An innovative process was followed including interdisciplinary team building, item generation: review of CAPS registries, systematic literature review, expert surveys, consensus conferences for item refinement, item reduction and weighting using 1000Minds decision software. Resulting CAPS criteria were tested in large cohorts of CAPS cases and controls using correspondence analysis. Diagnostic models were explored using sensitivity analyses. The international team included 16 experts. Systematic literature and registry review identified 33 CAPS-typical items; the consensus conferences reduced these to 14. 1000Minds exercises ranked variables based on importance for the diagnosis. Correspondence analysis determined variables consistently associated with the diagnosis of CAPS using 284 cases and 837 controls. Seven variables were significantly associated with CAPS (p<0.001). The best diagnosis model included: Raised inflammatory markers (C-reactive protein/serum amyloid A) plus ≥two of six CAPS-typical symptoms: urticaria-like rash, cold-triggered episodes, sensorineural hearing loss, musculoskeletal symptoms, chronic aseptic meningitis and skeletal abnormalities. Sensitivity was 81%, specificity 94%. It performed well for all CAPS subtypes and regardless of NLRP3 mutation. The novel approach integrated traditional methods of evidence synthesis with expert consensus, web-based decision tools and innovative statistical methods and may serve as model for other rare diseases. These criteria will enable a rapid diagnosis for children and adults with CAPS.
- Fever Syndromes
- Epidemiology
- Health services research
- Multidisciplinary team-care
Statistics from Altmetric.com
Introduction
Cryopyrin-associated periodic syndrome (CAPS) is a rare, heterogeneous disease entity. It encompasses a spectrum of clinical phenotypes associated with gain-of-function mutations in the NLRP3 gene encoding cryopyrin, a key regulatory protein, resulting in constitutive increased interleukin-1 (IL-1) secretion.1 ,2 While previously considered three distinct clinical diseases including familial cold autoinflammatory syndrome (FCAS), Muckle-Wells syndrome (MWS) and chronic infantile neurological, cutaneous and articular syndrome (CINCA)/neonatal-onset multisystem inflammatory disorder (NOMID), the discovery of a common causative gene mutation led to an amalgamation into the entity CAPS.3 NLRP3 gain-of-function mutations were shown to result in characteristic, yet diverse clinical symptoms of systemic and organ-specific inflammation and raise of inflammatory markers, most importantly C-reactive protein (CRP), serum amyloid A (SAA) and the neutrophil protein S100A12.4 ,5
CAPS is rare, affecting an estimated one to three in a million children and adults worldwide; no gender or ethnic predilection has been identified.6 CAPS-related inflammation causes fever, fatigue and organ irritation at the early stages, while long-standing uncontrolled inflammation results in irreversible organ damage. This includes sensorineural hearing loss, amyloidosis, vision loss, skeletal deformities and cognitive disability. Early diagnosis and inflammatory control is critical to prevent irreversible organ damage. In clinical practice, establishing the diagnosis of a rare disease, such as CAPS, is challenging resulting in significant delay to diagnosis.7 This delay or even complete lack of recognition can be attributed to different factors including limited ability of healthcare providers to recognise and diagnose a rare disease, the involvement of multiple subspecialists in the care of these complex patients with multisystem involvement and their lack of communication. Commonly, the main subspecialty responsible for the care of a patient is determined by the leading organ manifestation, such as hearing loss, urticaria-like skin rash, conjunctivitis or nephritis in a patient with CAPS.
Diagnostic criteria are limited in rare diseases. Their development heavily relies on international collaborative efforts of medical experts. Currently, there are no validated diagnostic criteria available capturing the entire spectrum of CAPS. This entails a significant risk for missing a window of opportunity for the reversal of IL-1-mediated inflammation and prevention of organ damage in CAPS. Therefore, the aim of the study was to develop and validate diagnostic criteria for children and adults with CAPS to enable an early diagnosis and prevent irreversible organ damage secondary to inflammation in CAPS.
Methods
A rigorous and innovative process was followed including: (a) an interdisciplinary, international expert team building of different paediatric and adult CAPS subspecialty experts plus rare diseases methods experts, (b) item generation and refinement: review of CAPS items in actively recruiting registries, systematic literature review, CAPS expert surveys and consensus conferences, (c) item reduction and weighting, (d) diagnostic model building using correspondence analysis and (e) model validation.
Expert team building
The multidisciplinary team had to include international experts in the care of children and adults with CAPS including rheumatologists and other subspecialists. It gathered experts in rare diseases research and methodology from both Europe and North America. Participants were invited based on their clinical and scientific expertise and geographical representation. They remained connected throughout the process including multiple surveys, decision analysis exercises and iterative face-to-face meetings.
Item generation
CAPS items were derived from registries, published literature and expert opinion surveys and meetings. Any sign or symptom or laboratory test used to characterise a CAPS patient or group was considered.
CAPS registry item review: All actively recruiting North American and European autoinflammation registries were reviewed for CAPS diagnosis items including Eurofever (Genoa, Italy), β-confident Canakinumab Registry (Novartis Pharma AG, Basel, Switzerland), Arthritis and Rheumatology Documentation and Information System (ARDIS, Tuebingen, Germany) and AutoInflammatory Disease-Network (AID-NET, Essen, Germany). All included registries have obtained institutional ethics board approval.
Systematic literature review: Published studies were identified through searches of MEDLINE, COCHRANE and EMBASE databases for the period from 1970 to 2013 following the European League Against Rheumatism (EULAR) rules for developing best practices8 (see online supplementary table S1). Keyword, title and abstract information were used. All synonyms of CAPS, CINCA/NOMID, MWS and FCAS were searched. In addition, a search for ‘autoinflammatory diseases’ and synonyms was performed; references and reviews were screened for additional articles. The review was performed as previously described.9 A total of 33 CAPS items were identified combined from the review of the CAPS registries and the systematic literature search.
supplementary tables
Item refinement, reduction and weighing
CAPS expert surveys: Using web-based survey methodology, experts were asked to review all items, add additional items, if applicable, and evaluate each item for its relevance in making the diagnosis of CAPS and applicability for CAPS subtypes including FCAS, FCAS/MWS, MWS, MWS/CINCA/NOMID and CINCA/NOMID (see online supplementary table S2). The survey had to be completed and returned by >80% of participants. Items were considered relevant, if there was ≥80% consensus agreement among experts.
CAPS consensus conference Istanbul, Turkey: Survey results were shared. All putative items were discussed and refined using nominal group technique.10 Refined items were voted on for their relevance for diagnosing CAPS and/or CAPS subtypes. Items were considered relevant, if there was ≥80% consensus agreement among experts.
CAPS consensus meeting in Boston, Massachusetts, USA: CAPS diagnosis items were shared and refined further using nominal group technique. Fourteen final putative CAPS diagnosis items were ranked for their relevance using 1000Minds decision analysis software.11 Experts were presented pairs of CAPS items and asked to identify the item of higher relevance for diagnosing CAPS (eg, sensorineural hearing loss present and amyloidosis absent or sensorineural hearing loss absent and amyloidosis present, all other manifestations being considered equal). The resulting ranking of CAPS items was computed; correlations between expert decisions were calculated.
Diagnostic model development and validation
Multiple correspondence analyses (MCA) were used to assess the multidimensional relationship between putative CAPS diagnosis items and patient diagnoses. MCA allows the optimal representation of a contingency table in low-dimensional space. Items with close relationship to the diagnosis of CAPS were then tested in multivariable logistic regression models resulting in a proposed diagnostic model.
Model development was guided by statistical significance. CAPS expert guidance was considered the gold standard. The proposed diagnostic model was validated in a large, multicentre cohort of children and adults with CAPS and true CAPS controls including systemic juvenile idiopathic arthritis (JIA), Schnitzler syndrome, familial Mediterranean fever (FMF), unclassified fever syndromes, typical Kawasaki disease (KD) and incomplete KD. MCA computed the χ2 statistic between each variable of interest and the outcome and transformed this statistic into a Euclidean distance. The quality of the lower-dimensional representation of the data is derived from singular values and is expressed as the percentage of the total inertia that is explained by each dimension. The total inertia of the data table can be regarded as the weighted average of the squared deviations between the subjects' profiles (the subjects' scores proportional to their total score) and the average score profile representing the amount of variation among the subjects' score patterns.12,13 The model was developed using 1000Minds potentially all pairwise rankings of all possible alternatives (PAPRIKA) methodology and then applied to a validation data set using MCA. The model was then refined and tested as described. For a quantitative interpretation of the correspondence plot results, the χ2 statistics were transformed into Pearson residuals (a standardised χ2 statistic). Subanalyses were performed for all CAPS subtypes and evidence of NLRP3 mutation. Sensitivity analyses were performed and the final diagnostic model was proposed. All analyses were performed using SAS software, V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Expert team
The multidisciplinary CAPS team included a total of 16 paediatric (JBK-D, SO, IK-P, HMH, EW-R, BH, TK, MG, FD, LC) and adult (RG-M, HL, NB, AG) subspecialists and methodology experts in rare diseases research (PNT, SMB) and was supported by two fellows (NTH, MO). The team members were selected based on their exceptional expertise in care and research in autoinflammatory diseases and the clinical severity spectrum of CAPS.
Item generation
The systematic literature review identified a total of 1698 unique records; 47 articles were selected for full-text screening, of which 33 were relevant and underwent validity assessment excluding four. The remaining 29 articles included a total of 794 patients with CAPS and generated a total of 33 putative CAPS diagnosis items (figure 1). The review of the CAPS registries did not yield any additional putative diagnosis items beyond those identified in the systematic literature review.

Systematic literature review of putative cryopyrin-associated periodic syndrome (CAPS) items.
Item refinement, reduction and weighing
CAPS expert surveys: Iterative surveys including the 33 putative CAPS diagnosis items were completed and returned by 100% of participants. In addition, seven new items were generated based on responses of CAPS experts.
CAPS consensus conference Istanbul: All 40 items were discussed, refined and grouped into (1) patient-related items including positive family history of CAPS and evidence of NLRP3 mutation, (2) disease course-related items: symptom onset in infancy, persistent inflammation with/without episodic attacks with worsening symptoms and induction of characteristic symptoms after generalised cold exposure, clinical signs and symptoms of CAPS coupled with laboratory findings of acute phase response, (3) CAPS-typical symptoms: recurrent episodes of systemic symptoms of fever and/or chills/rigors and/or fatigue, diffuse urticaria-like rash (neutrophilic infiltration in skin biopsy will clarify the origin in uncertain cases), recurrent eye inflammation including conjunctivitis with/without other inflammatory ocular findings, sensorineural hearing loss, clinical, laboratory and/or imaging evidence of chronic aseptic meningitis, musculoskeletal signs and symptoms of arthralgia, myalgia, arthritis and/or periarticular swelling, skeletal abnormalities including clubbing and/or frontal bossing and/or epiphyseal bony overgrowth and amyloidosis. A total of 14 CAPS items reached ≥80% agreement among experts.
CAPS consensus conference Boston: Items were reviewed and refined further resulting in the final item list (table 1). All items had achieved ≥80% agreement. Experts then participated in the iterative 1000Minds exercise process resulting in a ranking of items based on their importance for the diagnosis of CAPS. Mean criterion rankings (weighting) were calculated and ranged from 4 to 11. Results demonstrated excellent correlations between experts and for all subtypes.
Items and definitions for diagnostic criteria for CAPS
Diagnostic model development
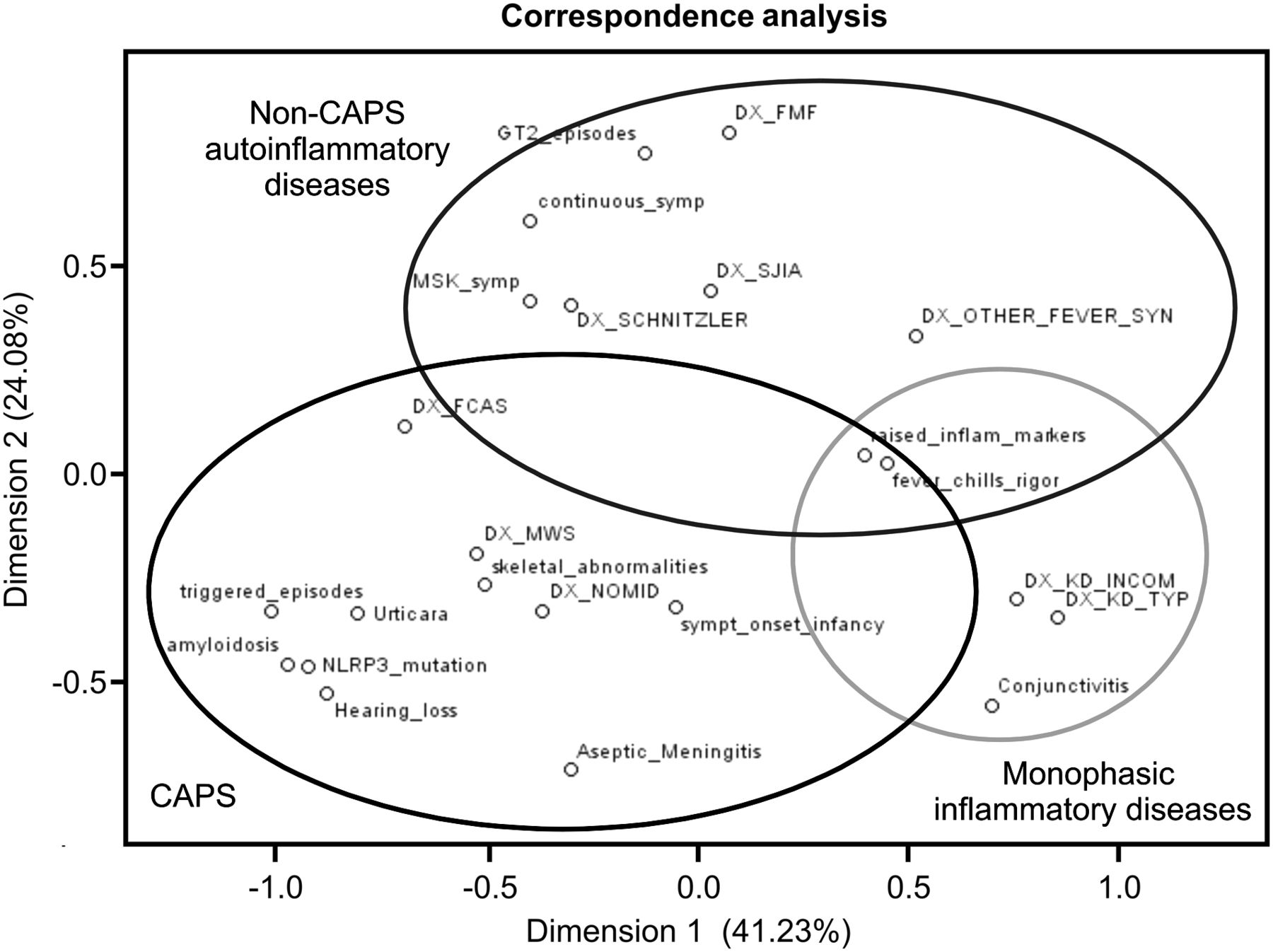
The unique multicentre, multinational cohort included 284 paediatric and adult patients with FCAS (30), MWS (164) and CINCA/NOMID (90). The CAPS control cohort consisted of 837 children and adults with either systemic JIA (100), Schnitzler syndrome (13), FMF (178), unclassified fever syndromes (93), typical KD (280) or incomplete KD (173). Multiple correspondence analysis was performed (see online supplementary tables S3, S4 and S5) including items from table 1 and identified three distinct entities: CAPS, non-CAPS autoinflammatory diseases and monophasic inflammatory diseases (figure 2). Correspondence analysis was successful in representing the contingency table in low-dimensional space with an overall retention of 78.78% (% total inertia) for a two-dimension solution (see online supplementary table S3) as determined by trace analysis for dependencies (χ2=2696.6, df=78, p<0.0001) and test for dimensionality (axis inertia >16.7%). The quality of representation of a particular row or column has been provided as contributions to the total χ2 statistic (see online supplementary table S4) and Pearson's residuals (see online supplementary table S5).

Capturing the diagnostic challenge of autoinflammation—discriminating cryopyrin-associated periodic syndrome (CAPS) from other inflammatory diseases using correspondence analysis. Multiple correspondence analyses (MCA) were used to assess the multidimensional relationship between putative CAPS diagnosis items and patient diagnoses in 284 CAPS cases including familial cold autoinflammatory syndrome (FCAS), Muckle-Wells syndrome (MWS) and chronic infantile neurological, cutaneous and articular syndrome/neonatal-onset multisystem inflammatory disorder (CINCA/NOMID) and 837 inflammatory controls. MCA computed the chi-squared statistic between each variable of interest and the outcome and transformed this statistic into a Euclidean distance. CAPS, non-CAPS autoinflammatory diseases and monophasic inflammatory diseases were the three distinct entities identified (see circles). Key variables consistently associated with the diagnosis of CAPS included urticaria-like rash, triggered episodes, sensorineural hearing loss, amyloidosis, musculoskeletal symptoms of arthralgia/arthritis/myalgia, chronic aseptic meningitis and skeletal abnormalities of epiphyseal overgrowth/frontal bossing (p<0.01). Raised inflammatory markers (C-reactive protein/serum amyloid A, (CRP/SAA)) and systemic symptoms of fever/chills/rigor were associated with all three entities.
Key variables consistently associated with the diagnosis of CAPS included urticaria-like rash, cold-triggered episodes, sensorineural hearing loss, amyloidosis, musculoskeletal symptoms (arthralgia/arthritis/myalgia), chronic aseptic meningitis and skeletal abnormalities (epiphyseal overgrowth/frontal bossing) (p<0.001 for all). Raised inflammatory markers (CRP and/or SAA) and systemic symptoms of inflammation (fever/chills/rigor) were associated with all three entities. In contrast, conjunctivitis was closely associated with monophasic inflammatory diseases, while continuous/persistent symptoms and episodic nature of disease had a closer relationship with non-CAPS autoinflammatory diseases. NLRP3 mutation was removed as predefined and amyloidosis due to its rarity.
Stepwise logistic regression was used in an attempt to identify variables independently and significantly (p<0.01) associated with CAPS. They included urticarial-like rash, cold-triggered episodes, sensorineural hearing loss, musculoskeletal symptoms, chronic aseptic meningitis and skeletal abnormalities. However, the resulting multivariable model was found to be dominated by musculoskeletal symptoms revealing evidence of lack of fit (H-L χ2 48.2, p<0.01). These predictors of interest were therefore considered separately or in combination with each other.
Diagnostic model validation
Different combinations of variables significantly associated with CAPS were tested for their association. Different models were explored. The best CAPS diagnosis criteria model included: raised inflammatory markers (CRP/SAA) plus ≥two of six CAPS-typical signs/symptoms including (1) urticaria-like rash, (2) cold-triggered episodes, (3) sensorineural hearing loss, (4) musculoskeletal symptoms (arthralgia/arthritis/myalgia), (5) chronic aseptic meningitis and (6) skeletal abnormalities (epiphyseal overgrowth/frontal bossing) (p<0.001) (figure 3). These last six criteria had similar mean criterion rankings (weighting) ranging between 5 and 9.8 and were pooled together in order to increase ease of use for a clinical setting. The final CAPS diagnosis criteria model had a specificity of 94% and a sensitivity of 81%. It performed equally well for all CAPS subtypes and in subgroups with and without evidence of NLRP3 mutation (p<0.001).

{kind=link}
{kind=link}
{kind=link}
A model for the diagnosis of cryopyrin-associated periodic syndrome (CAPS). The proposed model for diagnosing CAPS including one mandatory criterion, namely raised inflammatory markers, plus at least two of six CAPS-typical symptoms, had a sensitivity of 81% and a specificity of 94%.
Discussion
Criteria enabling physicians worldwide to make a diagnosis of the rare and heterogeneous autoinflammatory disease CAPS were developed and validated by an international team of experts using an innovative approach that integrated published evidence, registry expertise and expert opinion. It resulted in a comprehensive, well-defined list of putative CAPS diagnosis items capturing both the heterogeneous phenotype and the disease severity spectrum in children and adults with CAPS. The iterative review and refinement strategy using nominal group technique coupled with the 1000Minds decision analysis tool allowed for the development of a CAPS diagnosis model, which contained clinical and laboratory variables only, resulting in excellent generalisability. Most importantly, it did not mandate evidence of a disease-causing NLRP3 mutation. It performed well in a large validation cohort of more than 1000 patients with CAPS and controls (p<0.001) achieving a high sensitivity and specificity.
The CAPS diagnosis criteria development followed an innovative, comprehensive process, which integrated diverse clinical expertise with rare diseases research methodology. The process was iterative; items were refined and strict rules of communication and knowledge gain (nominal group technique) were followed. It used an easy-to-use web-based decision tool, the 1000Minds instrument. This item generation and refinement strategy had successfully been used previously for the development of classification criteria for adult scleroderma.14 Both the European and North American rheumatology societies promote its application.
The unique next step in this study was the exploration of the relevance of putative diagnosis items using correspondence analyses. This analysis highlighted the principles of the differential diagnostic challenges when diagnosing CAPS and its subtypes and discriminating these from other autoinflammatory and monophasic inflammatory diseases. It depicted both disease-specific variables and those representing the overlap between illnesses. It then permitted the development of a highly specific, sensitive and, most importantly, clinically relevant diagnostic model for CAPS. This approach may serve as a model for other rare diseases.
The proposed criteria are diagnostic criteria for CAPS and its subtypes. The study suggested that the presence of raised inflammatory markers (CRP or SAA) plus at least two of six CAPS-typical signs or symptoms including (1) urticaria-like rash, (2) cold-triggered episodes, (3) sensorineural hearing loss, (4) musculoskeletal symptoms of arthralgia/arthritis/myalgia, (5) chronic aseptic meningitis and (6) skeletal abnormalities of epiphyseal overgrowth/frontal bossing is highly likely to confirm the diagnosis of CAPS. This was confirmed in the presence and absence of a disease-causing NLRP3 mutation.
There are few diagnostic criteria in inflammatory diseases: The most commonly cited and used criteria are the Jones criteria for acute rheumatic fever15 and the KD criteria.16 Both are derived from clinical expert observation. The KD criteria were refined by the American Heart Association in order to capture the entire disease spectrum, even including children with incomplete features using laboratory markers to confirm the diagnosis.17 The vast majority of criteria for inflammatory diseases are classification criteria; developed within a group of overlapping conditions and aiming to establish well-characterised cohorts for research.18 ,19 Recently proposed classification criteria include the paediatric EULAR/Paediatric Rheumatology INternational Trials Organisation (PRINTO)/Paediatric Rheumatology European Society (PRES) criteria for childhood vasculitis,20 the Eurofever classification criteria for autoinflammatory diseases,19 the FMF criteria21 and the paediatric Behcet's disease classification criteria.22
In daily practice, criteria that enable a rapid diagnosis in rare diseases are urgently needed, in particular, in autoinflammatory diseases resulting in preventable organ damage. While the vast majority of available and stakeholder endorsed criteria sets are classification criteria—developed to identify homogenous cohorts for research studies23—the group of CAPS experts unanimously voted for these criteria being diagnostic criteria emphasising that care providers of children and adults with rare diseases need criteria to enable a rapid and reliable diagnosis.
The proposed CAPS diagnosis criteria are primarily clinical criteria. Clinical criteria are operator dependant and therefore carry the risk of limited sensitivity and specificity, the latter resulting in a risk of ‘overdiagnosing’ CAPS. This risk has to be considered prior to initiating therapies as the liability continues to be with the treating physician. The proposed CAPS criteria were developed by a group of CAPS experts and validated in a large cohort of inflammatory conditions. They will likely best perform when considered by inflammation experts in the context of a suspected systemic inflammatory disease. They have not been validated in potential non-inflammatory mimics, infectious or malignant conditions mimicking of CAPS. Robustness to each of the criteria can be added by symptom diaries such as the auto-inflammatory diseases activity index (AIDAI) questionnaire, pictures of clinical signs to be reviewed at clinic visits, serial blood tests for CAPS-typical inflammatory markers or skin biopsies, when suspecting a neutrophilic dermatitis causing the CAPS-typical urticaria-like rash. In particular when faced with a mild CAPS phenotype, these additional investigations should be considered prior to initiation of targeted therapies.
To our knowledge, the only other initiative aiming to develop and validate diagnostic criteria for inflammatory diseases is the Diagnosis and Classification Criteria for Vasculitis Study that has recruited over 5000 patients—adult vasculitis cases and vasculitis mimic controls—from 129 sites worldwide.24 In both disease entities, vasculitis and CAPS, a rapid diagnosis and initiation of targeted therapy is essential to prevent organ damage from inflammation.
The study has several limitations. The number of CAPS cases and controls was limited and not all possible differential diagnoses of CAPS may have been included, potentially leading to an overestimation of the specificity of the proposed model. However, the group dedicated long, thorough discussions to the identification of clinically relevant control populations. Importantly, the team collected the largest number of CAPS cases and controls studied to date. Not all subspecialists involved in the care of children and adults with CAPS were part of the team. The group did not identify any ear–nose–throat or ophthalmology CAPS experts, which may have caused an underrepresentation of clinical CAPS items generated from these subspecialists. However, missing expertise should have been partially compensated by items generated from the systematic literature review. Also, all team members provide care in an interdisciplinary team and felt that all specific organ-related items were well integrated.
Conclusion
The CAPS diagnosis model is the result of a unique collaborative team approach. It captures all diseases in the spectrum of CAPS and therefore enables a rapid diagnosis and initiation of treatment for children and adults with CAPS, a rare, heterogeneous inflammatory disease. The novel approach integrated traditional methods of evidence synthesis with expert consensus, web-based decision tools and innovative statistical methods and may serve as a model for developing diagnostic criteria for other rare diseases.
Acknowledgments
Travel and accommodation for the Istanbul consensus conference was kindly supported by SOBI. The 1000Minds decision analysis software was kindly provided to the team by the company free of cost. The study team would like to acknowledge the significant administrative contribution of Dr Iris Haug, University Children's Hospital Tuebingen and the support of Brandon Teteruck with the 1000Minds decision analysis software. We would like to thank Dr Guido Junge, Novartis Pharma AG, for allowing the team to include data from the CAPS β-confident registry for item generation and validation.
References
Footnotes
Handling editor Tore K Kvien
Contributors JBK-D, SO and SMB conceived of the study, organised the project, wrote and revised the manuscript; PNT conducted the statistical analyses; IK-P, RG-M, HL, NB, HMH, EW-R, BH, TK, MG, AG, FD and LC participated in the expert surveys and consensus conferences; NTH and MO conducted the standardised literature search and evaluated the papers for scientific content applying to this study.
Competing interests JBK-D performed clinical studies with Novartis and received speaking honoraria from Novartis and SOBI.
Provenance and peer review Not commissioned; externally peer reviewed.