Article Text

Abstract
Objective To score systemic activity at diagnosis and correlate baseline activity with survival in a large cohort of patients with primary Sjögren syndrome (SS).
Patients and methods We include 1045 consecutive patients who fulfilled the 2002 classification criteria for primary SS. The clinical and immunological characteristics and level of activity (EULAR-SS Disease Activity Index (ESSDAI) scores) were assessed at diagnosis as predictors of death using Cox proportional hazards regression analysis adjusted for age at diagnosis. The risk of death was calculated at diagnosis according to four different predictive models.
Results After a mean follow-up of 117 months, 115 (11%) patients died. The adjusted standardised mortality ratio for the total cohort was 4.66 (95% CI 3.85 to 5.60), and survival rates at 5, 10, 20 and 30 years were 96%, 90%, 81% and 60%, respectively. The main baseline factors associated with overall mortality in the multivariate analysis were male gender, cryoglobulins and low C4 levels. Baseline activity in the constitutional, pulmonary and biological domains was associated with a higher risk of death. High activity in at least one ESSDAI domain (HR 2.14), a baseline ESSDAI score ≥14 (HR 1.85) and more than one laboratory predictive marker (lymphopenia, anti-La, monoclonal gammopathy, low C3, low C4 and/or cryoglobulins) (HR 2.82) were associated with overall mortality; these HRs increased threefold to 10-fold when the analysis was restricted to mortality associated with systemic disease.
Conclusions Patients with primary SS, who present at diagnosis with high systemic activity (ESSDAI ≥14) and/or predictive immunological markers (especially those with more than one), are at higher risk of death.
- Sjögren's Syndrome
- Disease Activity
- B cells
Statistics from Altmetric.com
Introduction
Sjögren syndrome (SS) is a systemic autoimmune disease that principally affects women between the fourth and sixth decades of life, who present with sicca symptomatology of the main mucosal surfaces.1 The clinical spectrum of SS extends from dryness of the main mucosal surfaces to systemic involvement (extraglandular manifestations) and includes a large number of manifestations. Therefore, the therapeutic management of patients with primary SS is based principally on the management of both sicca and systemic manifestations.2
Systemic features may be the presenting manifestation or appear after the disease is diagnosed, and clearly mark the disease prognosis. Ioannidis et al3 were the first to propose a prognostic classification of primary SS; severe parotid involvement, vasculitis, hypocomplementaemia and cryoglobulins have been identified as the main factors reported in prospective studies.3–6 A practical message is that patients with this clinical/immunological ‘high risk’ pattern should receive a closer follow-up and, probably, earlier and more robust therapeutic management.
The development of the European League Against Rheumatism (EULAR)-SS Disease Activity Index (ESSDAI)7 by the EULAR Task Force on SS has represented a step forward in the evaluation of systemic SS. The ESSDAI includes specific organ-by-organ definitions and allows homogeneous evaluation of systemic features in a large series of patients.8 ,9 However, no study has evaluated the potential association between systemic activity scored at disease diagnosis and survival in patients with primary SS. The identification, at diagnosis, of markers prospectively associated with a poor prognosis could play a significant role in identifying patients requiring a closer follow-up.
The aim of this study was to score systemic activity at diagnosis using the ESSDAI and correlate the baseline ESSDAI with survival in a large cohort of Spanish patients with primary SS.
Patients and methods
Patients
The Spanish Group of Autoimmune Diseases (GEAS)-SS Study Group was formed in 2005 with the aim of collecting a large series of Spanish patients with primary SS, and included 20 Spanish centres with substantial experience in the management of patients with systemic autoimmune diseases. The design follows the main previous studies focused on mortality in primary SS3 ,4 and included both incident and prevalent cases; for incident cases, the diagnosis of primary SS was made during the first study visit after January 2005, while for the prevalent cases, the diagnosis was established before January 2005. By January 2014, the database included 1074 consecutive patients (666 prevalent cases) who fulfilled the 2002 classification criteria for primary SS,10 of whom 29 were excluded from the analysis due to a follow-up <180 days. Exclusion criteria were chronic hepatitis C virus (HCV)/HIV infection, previous lymphoproliferative processes and associated systemic autoimmune diseases. Diagnostic tests for SS (ocular tests, parotid scintigraphy and salivary gland biopsy) were performed according to the European Community Study Group recommendations.10 Clinical and laboratory data were collected and computerised according to a standard protocol.8
Definition of variables
The date of disease diagnosis was defined as the date when the physician responsible for the patient's follow-up confirmed fulfilment of the 2002 criteria.10 Systemic involvement was defined according to the ESSDAI,11 which evaluates 12 domains or organ systems. Each domain is divided into three to four levels according to the degree of activity and scored as 0 (no activity), 1 (low activity), 2 (moderate activity) or 3 (high activity). The ESSDAI score at diagnosis was retrospectively calculated by examination of medical records in order to collect disease activity before the date of SS diagnosis.
The end of the follow-up time for each patient was defined according to the last recorded Spanish National Healthcare System visit, which was the principal source of information about their health status. For patients with no information recorded in the last 5 years, two additional sources were used in a capture/recapture model: first, patients were telephoned using the available contact information, and second, we searched the death certificates of the corresponding area of residence. Causes of death were classified by the attending physician into six categories (systemic Sjögren, haematological neoplasia, infection, cardiovascular disease, other causes and unclassifiable) according to the following definitions: we classified a death as caused by systemic disease when a specific organ-specific damage included in the ESSDAI11 was considered as the ultimate/principal cause of death. Deaths due to systemic infection and haematological neoplasia were defined according to previous studies,12 and cardiovascular disease was defined according to a previous study;13 when the physician could not clearly attribute death to a single cause, it was considered as unclassifiable.
Statistical analysis
Descriptive data are presented as means and SD for continuous variables and numbers, and percentages for categorical variables. Time-to-event analyses for death and causes of death are presented as Kaplan–Meier curves. The standardised mortality ratio (SMR) was estimated using the age-matched and sex-matched probabilities of mortality from life tables of the general Spanish population in 2012 for comparison.14 The 95% CIs of the SMR were also calculated. The clinical and immunological characteristics and level of activity recorded in the ESSDAI organ domains were assessed at diagnosis as predictors of death using univariate Cox proportional hazards regression analysis adjusted for age at diagnosis. The level of activity was recorded as no activity versus any type of activity (low/moderate/high) in the analysis. Multivariate Cox proportional hazards regression analysis allowed adjustment for age at diagnosis and the variables that were statistically significant (p<0.05) in the univariate analysis, in order to establish independent variables associated with mortality. Additionally, additional models were fitted including statistically significant ESSDAI domains in the univariate Cox proportional hazards regression analysis and clinical ESSDAI domain activity levels (excluding the biological domain) adjusted for statistically significant biological markers as confounders.
The risk of death was calculated at diagnosis according to the following predictive models: Model A: maximum level of activity achieved in at least one of the ESSDAI organ domains (high, moderate, low or none);11 Model B: baseline numeric ESSDAI score categorised according to the EULAR-SS recommendations15 as no activity, low activity, moderate activity and high activity (scores of 0, 1–4, 5–13 and ≥14, respectively); Model C: number of laboratory parameters associated with mortality in the univariate analysis, which were classified according to the model used by Baldini et al6 into three categories (none, one or more than one); and Model D: number of predictive parameters associated with mortality that were reported by Skopouli et al16 (parotid enlargement, purpura and low C4: none, one or more than one).
Two sensitivity analyses were performed: (1) excluding 10 patients in whom the cause of death was unknown or unclear from the overall death analysis; (2) comparing no or low activity versus moderate or high activity.
The HRs and their 95% CIs obtained in the adjusted regression analysis were calculated. All significance tests were two-tailed, and values of p<0.05 were considered significant. All analyses were conducted using the R V.3.0.3 for Windows statistical software package.
Results
Baseline characterisation
Baseline characteristics are summarised in table 1. The cohort consisted of 1045 patients, including 982 (94%) women and 63 (6%) men (female:male ratio, 16:1), with a mean age at diagnosis of 54.0±15.1 years (range, 14–88 years). At diagnosis, 997 (95%) patients presented with dry mouth, 995 (95%) with dry eye, 905/981 (92%) had altered ocular diagnostic tests (Schirmer's test and/or rose Bengal staining), 682/789 (86%) altered parotid scintigraphy and 452/516 (88%) a salivary gland biopsy showing focal lymphocytic infiltration. The main immunological features at diagnosis were antinuclear antibodies ≥1/80 in 947/1043 (91%) patients, anti-Ro/SS-A in 773/1041 (74%), rheumatoid factor in 538/1012 (53%), anti-La/SS-B in 476/1038 (46%), low C4 levels in 123/991 (12%), cryoglobulinaemia in 79/748 (11%) patients, low C3 levels in 96/992 (10%) and monoclonal gammopathy in 77/818 (9%).
Variables at diagnosis as predictors of death of a Spanish cohort of 1045 patients with primary SS*
Survival
One hundred and fifteen (11%) patients died after a mean follow-up of 117.4 months (range 6–388 months), of which 101 were women and 14 men, with a mean age at death of 76.4 years. The main causes of death were cardiovascular disease in 35 patients, infections in 21, systemic disease in 18, haematological neoplasia in 10 and other causes in 21; in the remaining 10 cases, the cause of death was unknown or unclassifiable. The SMR for the total cohort (adjusted for age and gender with the general Spanish population) was 4.66 (95% CI 3.85 to 5.60).
Figure 1A shows the survival curve of the entire cohort; survival at 5, 10, 20 and 30 years was 96.0%, 90.5%, 80.9% and 60.4%, respectively. The following baseline variables at diagnosis were associated with death in the Cox regression analysis (table 1): male sex (HR 2.98, p<0.001), altered parotid scintigraphy (HR 2.81, p=0.043), lymphopenia (HR 1.63, p=0.034), anti-La antibodies (HR 1.51, p=0.034), C3 levels <0.82 g/L (HR 1.93, p=0.034), C4 levels <0.11 g/L (HR 2.06, p=0.016), monoclonal gammopathy (HR 1.81, p=0.047) and cryoglobulins (HR 2.58, p<0.001). Multivariate analysis identified male gender, cryoglobulins and low C4 levels as variables independently associated with death (table 1).

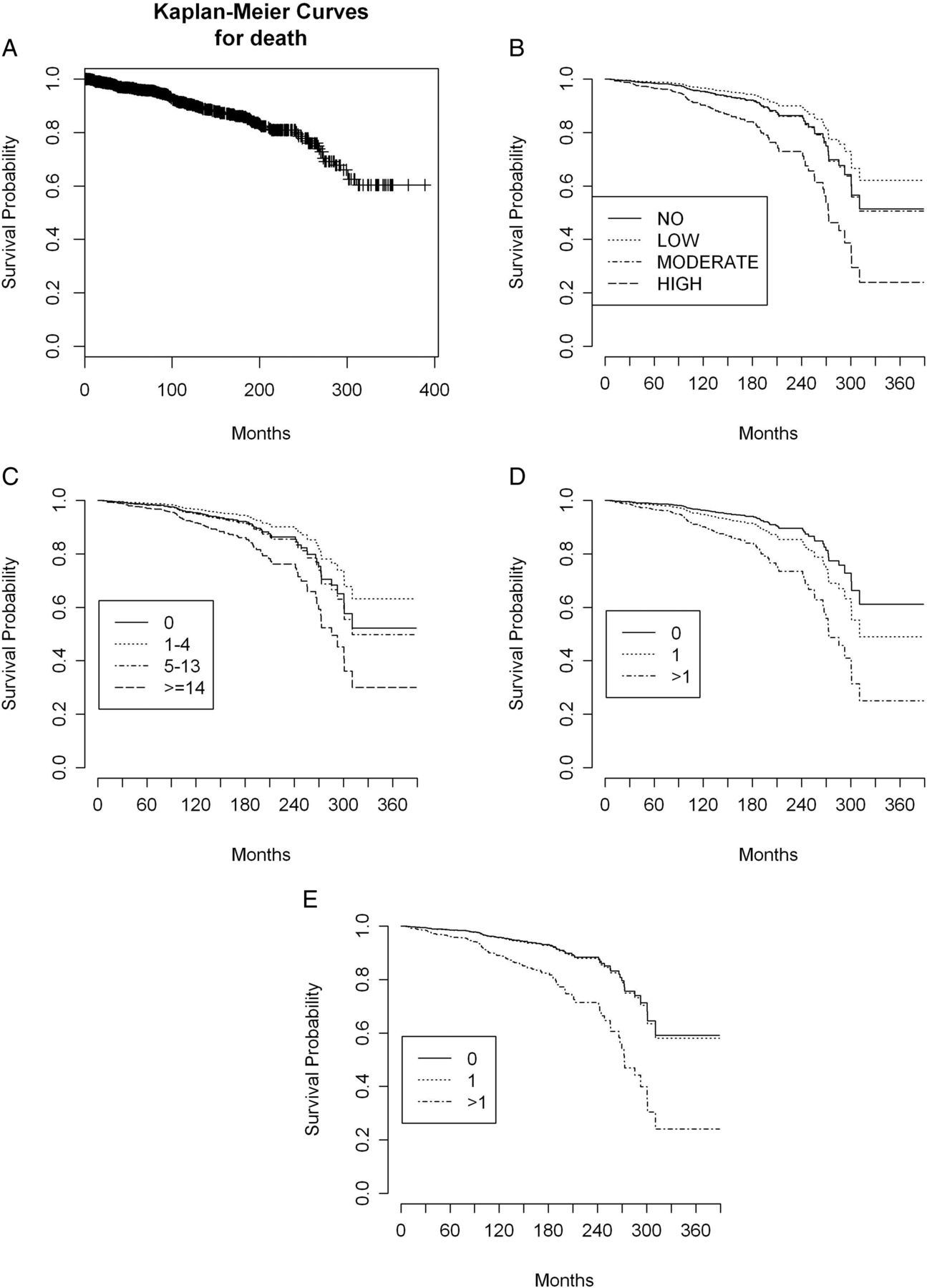{kind=link}
(A) Survival curve of the entire cohort. (B) Survival curves adjusted for age at diagnosis according to the maximum level of activity achieved in any of the 12 EULAR-SS Disease Activity Index (ESSDAI) domains (none, low, moderate, high) for overall death (Model A). (C) Survival curves adjusted for age at diagnosis according to categorisation of the baseline ESSDAI score according to the EULAR-SS Task Force proposal (scores=0, 1–4, 5–13 and ≥14) for overall death (Model B). (D) Survival curves adjusted for age at diagnosis according to the number of laboratory parameters associated with mortality in the univariate analysis (none, one or more than one) for overall death (Model C). (E) Survival curves adjusted for age at diagnosis according to the number of predictive parameters associated with mortality, reported by Skopouli et al16 (none, one or more than one) for overall death (Model D).
ESSDAI and survival
The mean ESSDAI score at diagnosis of the entire cohort was 5.89 (SD 6.73); patients who died had a baseline score of 7.80 in comparison with 5.65 for survivors (p>0.05). The highest scores at baseline were for patients who died from infections (14.90, SD 12.50) or from systemic disease (13.33, SD 11.92). The mean baseline ESSDAI for patients who died from haematological neoplasia, cardiovascular disease and other causes was 6.20 (SD 6.37), 4.06 (SD 5.33) and 4.90 (SD 6.39), respectively (table 2).
Level of activity in each ESSDAI domain at diagnosis
Table 3 summarises the association between organ-by-organ baseline ESSDAI activity at diagnosis and the risk of death. Baseline activity in the constitutional, pulmonary and biological domains was associated with a higher risk of death. Activity in the constitutional, lymphadenopathy, pulmonary, haematological and biological domains was associated with a higher risk of death due to systemic disease, while eight out of 12 ESSDAI domains were associated with death due to infection. No association was found between baseline activity and a higher risk of death related to cardiovascular disease, haematological neoplasia or other causes. The sensitivity analysis excluding 10 patients in whom cause of death was unclassifiable/unknown from the overall death analysis provided similar results (data not shown). Additionally, the sensitivity analysis comparing no/low activity versus moderate/high activity showed differences for the domains with the lowest frequencies for moderate/high activity: the constitutional domain changed from related to unrelated to death, while the renal domain achieved statistical significance (HR 4.71, 95%CI 1.15 to 19.36) (see online supplementary table S1). Analysis of the ESSDAI clinical domains (excluding the biological domain) after adjustment for the statistically significant biological markers in table 1 as confounders found that, in the adjusted models, the association between ESSDAI clinical activity levels and death often disappeared due to the high correlation between ESSDAI clinical domains and biological markers (see online supplementary table S2).
Level of activity in each ESSDAI domain at diagnosis as predictors of death*
Prognostic classification
We tested the usefulness of the four proposed models at diagnosis for predicting death: the maximum level of activity achieved in any of the 12 ESSDAI domains (model A), categorisation of the baseline ESSDAI score according to the EULAR-SS Task Force proposal (model B), the number of laboratory B-cell-related markers6 (model C) and the number of clinical-immunological features16 (model D) present at diagnosis. Table 4 summarises the main results: high activity in at least one domain (HR 2.14, p=0.011), a baseline ESSDAI score ≥14 (HR 1.85, p=0.037), more than one laboratory abnormality (HR 2.82, p<0.001) and predictive markers (HR 2.71, p=0.002) were associated with mortality. Figure 1B–E shows the survival curves of the cohort according to the four models (log rank <0.001 for all adjusted models). HRs increased threefold to 10-fold when the analysis was restricted to mortality associated with systemic disease (table 4, see online supplementary figures).
Discussion
Primary SS is often considered a chronic, non-life-threatening disease, overwhelmingly dominated by dryness, fatigue and pain. However, systemic involvement is increasingly recognised as part of the disease spectrum, since it is present at diagnosis in 70%–80% of patients,8 ,9 and plays a key role in the prognosis of primary SS, with the joints, lungs, skin and peripheral nerves being the organs most frequently involved. Baldini et al6 found severe systemic manifestations in 15% of patients, especially those with an immunological profile suggestive of B-cell activation. These recent multicentre studies, including more than 2500 European patients, confirm that primary SS is, undeniably, a systemic autoimmune disease.
Reported mortality rates in primary SS cohorts have decreased progressively during the last four decades: in 1978, Kassan et al17 reported a rate of 40%, a figure that was reduced to 20%–26% in studies in the 1990s18–20 and to 5%–15% in studies in the 2000s.3–5 ,21 ,22 Mortality is mainly attributed to systemic disease and lymphoma, although all the studies mentioned included all causes of mortality in their analyses. The identification of baseline factors that confer an increased risk of death may be very useful in identifying, at diagnosis, patients who require a closer follow-up and treatment as early as possible. Ioannidis et al3 were the first to propose a prognostic classification of patients with primary SS according to the presence of low C4 levels and/or palpable purpura (type I and type II patients) and this, together with low C3 levels, cryoglobulins and monoclonal band, was confirmed by other European studies.4–6 Our results show that the main baseline features associated with a higher risk of death were systemic activity at diagnosis, cytopenias, monoclonal gammopathy, cryoglobulins and hypocomplementaemia. Cryoglobulins play a central role in this high-risk clinical and immunological presentation for several reasons: the most severe extraglandular manifestations of SS are often related to cryoglobulinaemic disease; cryoglobulins are closely associated with other immunological prognostic markers (hypocomplementaemia, monoclonal band), and patients with cryoglobulinaemia are at a higher risk of developing B-cell lymphoma. Patients with cryoglobulinaemia at SS diagnosis, especially when there is vasculitic involvement, should be closely followed and treated early due to the high risk of adverse outcomes.
Until now, studies investigating the prognostic factors of death have centred on the epidemiological, clinical and laboratory features at the diagnosis of primary SS. The present study is the first to evaluate the potential association between baseline systemic activity, measured by the ESSDAI score, and mortality. Our results showed no significant differences in the mean ESSDAI score at diagnosis between patients who died and survivors, probably because the majority of patients presented a low degree of systemic activity at diagnosis. However, analysis of the causes of death showed that patients who died due to systemic disease or infections had a twofold greater baseline ESSDAI score compared with patients who died due to causes unrelated to SS, suggesting that high baseline systemic activity may be related to a higher risk of death.
With respect to the organ-by-organ ESSDAI analysis, we found that activity in the constitutional, lymphadenopathy and pulmonary ESSDAI domains at diagnosis was related to poor survival. On the one hand, activity in the two first domains (fever, weight loss, lymphadenopathy) is often seen in patients at high risk of systemic disease and/or lymphoma during the follow-up. On the other hand, pulmonary involvement is one of the main predictors of death in primary SS. SS-related pulmonary disease is clearly associated with worsened quality of life and poorer survival, with a twofold to fourfold increase in the risk of death23 ,24 compared with patients without pulmonary disease. Additionally, we found a statistical trend to reduced survival in patients with renal ESSDAI activity. Patients with glomerulonephritis25 had high rates of adverse outcomes, especially those with cryoglobulinaemic-mediated glomerular damage. The lack of association found in our study is probably due to the small number of patients presenting with glomerulonephritis at diagnosis (<1%). In fact, the sensitivity analysis comparing no/low activity with moderate/high activity found that the renal domain achieved statistical significance (HR 4.71, 95% CI 1.15 to 19.36).
Although the total mean ESSDAI score at diagnosis did not correlate with survival, specific analysis of the subset of patients presenting with a very high level of activity at diagnosis showed a significant association. Patients with the highest level of activity at diagnosis in at least one domain had a higher mortality rate, as did those who had a high baseline score (ESSDAI ≥14) according to the categories proposed by the EULAR Task Force.15 Primary SS may initially present as systemic disease without sicca features, and a positive immunological result will lead to an early diagnosis of SS several years before the onset of an overt sicca syndrome;26 a large number of extraglandular manifestations involving the skin, lungs, kidneys or nervous system, together with symptomatic cytopenias (haemolytic anaemia, severe thrombocytopenia), may appear before sicca symptoms.27 These patients will have a high baseline ESSDAI score even in the absence of significant sicca manifestations.
We found an overall SMR of 4.66. The two causes of death traditionally associated with excess mortality in patients with primary SS in comparison with the general population are B-cell lymphoma and severe organ-specific features (principally interstitial lung disease, renal failure and severe cryoglobulinaemic vasculitis). However, we identified two additional prominent causes of death: infection (this is an unexpected finding that deserves specific analysis in a further study) and cardiovascular disease, which has recently been associated with primary SS.13 ,28 Therefore, our patients with primary SS had excess of mortality due to multiple causes, although the predominant aetiologies were unrelated to SS itself (infections and cardiovascular disease). A possible explanation for the lesser role of autoimmune complications might be the lower frequency of end-stage organ failure caused directly by systemic Sjögren, together with the excellent prognosis of the most frequent type of haematological neoplasia reported in our patients (low-grade mucosa-associated lymphoid tissue lymphoma). As occurs with other autoimmune diseases, such as systemic lupus erythematosus or rheumatoid arthritis,29 ,30 mortality in primary SS is not solely related to the autoimmune disease itself.
Measurement of systemic activity by the ESSDAI at the diagnosis of primary SS is helpful in identifying a specific subset of patients who require closer follow-up, and some general recommendations may be proposed. Patients with a clinical presentation principally limited to the mucosal surfaces (mainly dryness, fatigue and pain) without systemic involvement and/or laboratory prognostic markers (baseline ESSDAI score <5) may require only annual evaluation. By contrast, patients presenting with high systemic activity (ESSDAI ≥14) and/or predictive immunological markers (especially those with more than one) may be closely followed every 3–6 months by a specialist in autoimmune diseases, including a routine physical examination including peripheral lymphadenopathy and enlargement of parotid glands, the liver and the spleen. Measurement of baseline systemic activity by the ESSDAI in patients diagnosed with primary SS is significantly associated with the prognosis.
Acknowledgments
The authors wish to thank David Buss for his editorial assistance.
Appendix
The members of the SS Study Group, Autoimmune Diseases Study Group (GEAS), Spanish Society of Internal Medicine (SEMI) are:
M. Ramos-Casals (Coordinator), P. Brito-Zerón, S. Retamozo, A. Bové, H. Gheitasi (Sjögren Syndrome Research Group-AGAUR, Laboratory of Autoimmune Diseases Josep Font, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Department of Autoimmune Diseases, ICMiD, Hospital Clínic, Barcelona), R. Solans, J.A. Bosch, M. Ramentol, (Department of Internal Medicine, Hospital Vall d'Hebron, Barcelona), G. Fraile, J. Nava-Mateos (Department of Internal Medicine, Hospital Ramón y Cajal, Madrid), B. Pérez-Díaz, C. Suarez-Cuervo, D. Caravia-Duran (Department of Internal Medicine, Hospital Universitario Central de Asturias, Oviedo), A. Casanovas, M.L. Morera-Morales, T.E. Junco-Russeau (Department of Internal Medicine, Hospital Parc Taulí, Sabadell), F.J. Rascón, L. Pallarés (Department of Internal Medicine, Hospital Son Espases, Palma de Mallorca), R. Qanneta (Department of Internal Medicine, Hospital Joan XXIII, Tarragona), R. Pérez-Alvarez, M. Perez-de-Lis (Department of Internal Medicine, Hospital do Meixoeiro, Vigo), M. Ripoll (Department of Internal Medicine, Hospital Infanta Sofía, Madrid), B. Pinilla, O. Lopez-Berastegui, (Department of Internal Medicine, Hospital Gregorio Marañón, Madrid), M. Akasbi, I. García-Sanchez (Department of Internal Medicine, Hospital Infanta Leonor, Madrid), M.T. Camps, M.M. Ayala (Department of Internal Medicine, Hospital Carlos Haya, Malaga), B. Sopeña, B. Maure (Department of Internal Medicine, Complejo Hospitalario Universitario, Vigo), J.L. Callejas (Department of Internal Medicine, Hospital San Cecilio, Granada), E. Fonseca (Department of Internal Medicine, Hospital de Cabueñes, Gijón), J. Canora (Department of Internal Medicine, Hospital Universitario de Fuenlabrada, Madrid), E. Nadal, C. Merino-Palacios (Department of Internal Medicine, Hospital La Ribera, Valencia), G de la Red (Department of Internal Medicine, Hospital Espíritu Santo, Barcelona), A.J. Chamorro, I. Fernández-Regal (Department of Internal Medicine, Complejo Hospitalario de Ourense, Ourense), I. Jiménez-Heredia, A. Mendizabal (Department of Internal Medicine,Hospital de Manises, Valencia, Spain), B. Adrianov, A. Sisó-Almirall (Primary Care Research Group, IDIBAPS, Centre d'Assistència Primària ABS Les Corts, CAPSE, Barcelona, Spain).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
PB-Z is supported by the Josep Font Research Fellow Award, Hospital Clinic, Barcelona, Spain.
Collaborators The members of the Sjögren Syndrome Study Group of the Spanish Group of Autoimmune Diseases (GEAS), Spanish Society of Internal Medicine (SEMI) are listed in appendix 1.
Contributors Conception and design: PB-Z, MR-C; acquisition of data: all authors; analysis and interpretation of data: PB-Z, BK, MR-C; statistical analysis: BK, MR-C; drafting the article or revising it critically for important intellectual content: all authors; final approval of the version published: all authors.
Funding Supported by Grants ‘La Marató de TV3’ (071810), ‘Fondo de Investigaciones Sanitarias’ (080103/1201009) and ‘Ajut per la Recerca Josep Font, Hospital Clínic de Barcelona’.
Competing interests None.
Ethics approval The institutional review board of Ethics Committee, Hospital Clinic, Barcelona, Spain
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available on request.