Article Text

Abstract
Objectives It is not clear whether heightened pain sensitivity in knee osteoarthritis (OA) is related to sensitisation induced by nociceptive input from OA pathology (‘state’) versus other confounding factors. Conversely, some individuals may be predisposed to sensitisation irrespective of OA (‘trait’).
Methods The Multicenter Osteoarthritis Study is a longitudinal cohort of persons with or at risk of knee OA. We obtained knee X-rays, pain questionnaires and comprehensive assessment of factors that can influence pain sensitivity. We examined the relation of sensitisation and sensitivity assessed by mechanical temporal summation (TS) and pressure pain thresholds (PPTs) to knee OA and knee pain severity. To test whether sensitisation and sensitivity is a ‘state’ induced by OA pathology, we examined the relation of PPT and TS to knee OA duration and severity.
Results In 2126 subjects (mean age 68, mean body mass index (BMI) 31, 61% female), PPT and TS were not associated with radiographic OA (ORs 0.9–1.0 for PPT and TS; p>0.05). However, PPT and TS were associated with pain severity (ORs: 1.7–2.0 for PPT; 1.3–1.6 for TS; p<0.05). Knee OA duration and radiographic severity were not associated with PPT or TS.
Conclusions PPT and TS were associated with OA-related pain, but not radiographic OA after accounting for pertinent confounders in this large cohort. Lack of association with disease duration suggests at least some sensitisation and pain sensitivity may be a trait rather than state. Understanding the relationship between pathological pain and pain sensitivity/sensitisation offers insight into OA pain risk factors and pain management opportunities.
- Osteoarthritis
- Epidemiology
- Knee Osteoarthritis
Statistics from Altmetric.com
Introduction
Causes of pain in knee osteoarthritis (OA) remain poorly understood despite pain being the primary symptom and cause of disability in OA. The structure-symptom discordance in knee OA1–10 suggests that structural pathology alone cannot account for the variation in pain severity experienced.
Increasing attention is being paid to neurobiological mechanisms’ contribution to knee OA pain. Enhanced nociceptive transmission at the spinal dorsal horn related to inflammatory stimuli has been demonstrated in animal models, which may be directly related to OA pathology.11–19 Ongoing tissue injury or inflammation in the joint can lead to increased responsiveness of peripheral nociceptors (peripheral sensitisation) and spinal dorsal horn transmission neurons (central sensitisation), such that nociception may no longer play a protective role.20–22 Alterations in descending inhibitory pathways and facilitated central integration can also contribute to the pain experience. Another possibility is that individuals with greater capacity to develop sensitisation may be at higher risk of experiencing more pain from a particular extent of OA.
If neurobiological changes were induced by OA and contribute to pain severity, it would complement the observation of activity-related pain (ie, apparently nociceptive) early in disease transitioning to chronic pain.23 Several small studies have demonstrated greater sensitisation among persons with painful knee OA compared with pain-free, healthy controls.24–29 However, the differences noted may be related to pain versus no pain rather than specifically to OA itself. Additionally, ‘healthy’ controls may differ in important ways from those with OA, confounding those results. For example, emotional and psychological factors can influence pain processing.30 ,31 Prior studies have been unable to examine duration of OA pathology to determine whether OA itself may induce sensitisation. As such, there is little evidence from human studies about whether sensitisation is a ‘state’ induced by peripheral OA pathology versus a ‘trait’ that is present irrespective of OA pathology, for example, due to genetic or other systemic predisposition present prior to knee OA.
Identifying sensitisation as a mechanism for pain would provide additional targets for pain management in OA, a disease with limited therapeutic options. Understanding whether knee OA pathology or symptom duration drives nociceptive input and the occurrence of sensitisation (ie, sensitisation as a ‘state’) would have implications for timing of treatment and may provide insights into the transition from acute to chronic pain in OA. If, however, sensitisation were a trait (ie, unrelated to OA), it may suggest more global strategies to mitigate effects of sensitisation on pain would be required and lead to a search for biomarkers of host susceptibility.
We evaluated the relation of sensitisation to the pain experience in knee OA in a large, well-characterised cohort of older adults with or at risk of knee OA, and whether duration or severity of OA may be related to sensitisation.
Methods
Study sample
The Multicenter Osteoarthritis Study is a longitudinal cohort comprising 3026 older adults aged 50–79 years at baseline who had or were at risk of knee OA. Subjects were recruited from Birmingham, Alabama and Iowa City, Iowa, and assessed at 0-month, 30-month and 60-month study visits. Details of the cohort have been published elsewhere.32 The study protocol was approved by the institutional review boards at the University of Iowa, University of Alabama at Birmingham, University of California at San Francisco and Boston University Medical Center.
The current sample comprised subjects who attended the 60-month visit, the first visit at which measures of sensitisation were obtained. We excluded individuals who screened positive for possible peripheral neuropathy (N=88).33
Clinical pain assessment
Knee-specific pain severity from the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC) pain questionnaire was categorised as none (0), mild/moderate (1–2) and severe/extreme (3–4) based upon the worst score on the pain questions.34
Each knee was categorised as having frequent knee pain based upon the following question: “During the past 30 days, have you had pain, aching or stiffness in your knee on most days?”
Radiographic and symptomatic osteoarthritis assessment
Bilateral weight-bearing fixed-flexion posteroanterior radiographs and lateral weight-bearing radiographs of the knee were obtained at each study visit.35 ,36 Whole knee radiographic OA (ROA) was defined as presence of tibiofemoral OA (Kellgren-Lawrence (KL) grade ≥2) and/or patellofemoral OA (osteophyte score ≥2, or joint space narrowing score ≥2 with any osteophyte, sclerosis or cyst score ≥1 on the lateral view), or knee replacement.36–38 Whole knee symptomatic OA (SOA) was defined as ROA plus frequent knee pain in the same knee, or knee replacement.
Measures of sensitisation
Pressure pain threshold (PPT), a measure of sensitivity to pain evoked by mechanical stimulation of nociceptors,39–41 has been reliably assessed with pressure algometry,28 ,42 including in knee OA studies.25–29 PPT assessed close to the site of disease (eg, knee with OA) is thought to be a reflection of activity-dependent peripheral sensitisation where pathology in the joint alters pain sensitivity in adjacent normal tissue (skin). When assessed at a distant, normal site (eg, wrist), it is thought to reflect systemic altered pain processing, which may be related to central sensitisation. PPT was assessed by applying an algometer (1 cm2 rubber tip; Wagner, FDIX25) at a rate of 0.5 kg/s on the centre of the patellae bilaterally and distal radioulnar joint (control site; right side unless contraindicated) as the point at which participants indicated the pressure first changed to slight pain. The PPT at each anatomical site was calculated by averaging three trials, and categorised into sex-specific tertiles. Lower PPTs represent a greater degree of sensitisation or increased pain sensitivity.
Mechanical temporal summation, an augmented response to repetitive mechanical stimulation, is a sensitive and valid measure of central pain processing (central amplification), which is a feature of central sensitisation, including in knee OA.29 ,43–45 Mechanical temporal summation was assessed using a weighted 60 g von Frey monofilament at the wrist and patellae (Aalborg University, Denmark). Subjects first provided a numerical pain rating to a trial of four stimulations. Subsequently, the monofilament was applied repeatedly over the skin of the same site at a frequency of 1 Hz for 30 s. Subjects provided a pain rating at the completion of the train of 30 simulations, and 15 s post stimulation. Temporal summation was defined as being present when, compared with the initial trial, the subject reported increased pain following the repeated mechanical stimulation at the site being tested. Similar methods have been used to assess mechanical temporal summation in knee OA and other conditions.45 ,46
Assessors were blinded to clinical and imaging data. Fourteen-day test-retest reliability for PPT was 0.85–0.90 (intraclass coefficients) and for temporal summation was 0.61 (κ; ASE 0.10).
We refer to these measures as ‘sensitisation’ hereafter, but acknowledge that they may also reflect heightened pain sensitivity.
Potential confounders
Potential confounders included age, sex, body mass index (BMI), race, study site, KL grade, patellofemoral OA, knee injury, depressive symptoms (Center for Epidemiologic Studies Depression Scale47), catastrophising (from the Coping Strategies Questionnaire48), use of analgesics (non-steroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase (COX-2) inhibitors, opiates, acetaminophen) and widespread pain (validated standard homunculus49).
Statistical analyses
Our OA and pain outcomes were ROA, SOA, frequent knee pain and knee pain severity. We compared the two lower sex-specific PPT tertiles to the highest sex-specific tertile (referent group), and compared presence of temporal summation with its absence for each of these OA and pain outcomes. Dichotomous outcomes (ROA, SOA, frequent knee pain) were evaluated using logistic regression. Knee pain severity (3-level outcome) was assessed using proportional odds logistic regression. For knee-based outcomes, generalised estimating equations were used.50 All analyses were adjusted for potential confounders (age, sex, BMI, race, clinic site, KL grade, patellofemoral OA, knee injury, depressive symptoms, analgesic use and catastrophising). Because widespread pain may be an intermediate in the causal pathway (ie, sensitisation → widespread pain → OA-related pain), our main analyses did not adjust for this variable as it could induce bias; we included it in sensitivity analyses.
If sensitisation were a ‘state’ induced by OA pathology, sensitisation would be expected to be more prevalent in those with longer duration and/or severity of ROA or SOA. To address this, we categorised duration of ROA for each knee based upon the first study visit at which ROA was identified: at the baseline visit (‘longest duration’), 30-month visit (‘middle duration’) or 60-month visit (‘shortest duration’); those without ROA at the 60-month visit were categorised as no OA. We similarly categorised duration of SOA based upon the first study visit at which ROA and knee pain (ie, frequent knee pain and WOMAC ≥4/20) were identified. Severity of ROA was categorised according to KL grade. We compared the mean adjusted PPT and likelihood of temporal summation across the categories of OA duration and severity using multiple linear regression and logistic regression, respectively.
All analyses were performed using SAS V.9.1 (SAS Institute, Gary, North Carolina, USA).
Results
There were 2126 subjects and 4266 knees eligible for this study (figure 1). The majority of subjects were female, obese and Caucasian, and the mean age was 68 years (table 1). Sixty-five per cent of subjects had ROA, 375 knees were replaced, and a third had no pain on the WOMAC scale. PPT at each anatomical site varied widely among subjects. Temporal summation was present in 41% of subjects.
Baseline participant characteristics

Flow chart of subject disposition. The Multicenter Osteoarthritis (MOST) Study. RA, rheumatoid arthritis.
{kind=link}
{kind=link}
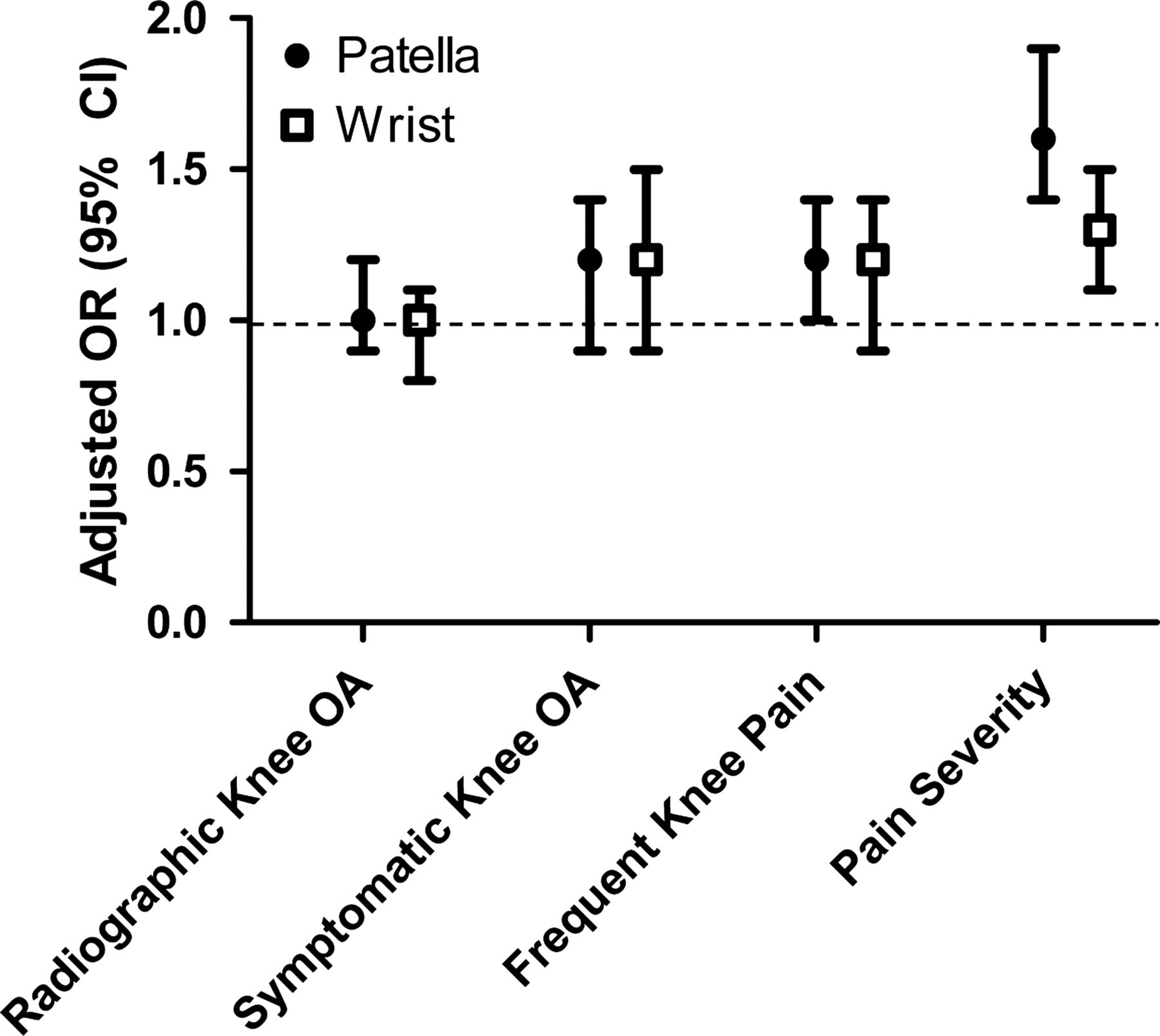
Relation of temporal summation to presence of radiographic whole knee osteoarthritis (OA), symptomatic whole knee OA, frequent knee pain and knee pain severity.
Neither PPT at the patella nor PPT at the wrist were associated with ROA. The odds of having ROA were 0.9 (95% CI 0.7 to 1.1) and 1.0 (95% CI 0.8 to 1.2) at the patella and wrist, respectively, for those in the lowest PPT tertile (ie, those most likely to have sensitisation) compared with those in the highest (table 2). However, PPT was related to knee pain. There was a dose-response relationship between PPT tertiles with presence of SOA, frequent knee pain and greater knee pain severity; those in the lowest PPT tertiles were most likely to have each of these outcomes (table 2). For example, those in the lowest PPT tertile had 2.0 times (patella) and 1.7 times (wrist) higher likelihood of having greater knee pain severity than those in the top tertile. The effect estimates were similar between the patella and wrist.
Relation of PPT to presence of radiographic whole knee OA, symptomatic whole knee OA, frequent knee pain and knee pain severity
Similar findings were noted for temporal summation and ROA. The ORs for having ROA among those with temporal summation at the patella was 1.0 (95% CI 0.9 to 1.2) and at the wrist was 1.0 (95% CI 0.8 to 1.1) (figure 2). Although those with temporal summation had 1.2 times higher odds of SOA and frequent knee pain, these were not statistically significant. Temporal summation at each anatomical site was associated with degree of knee pain severity. Those with temporal summation at the patella were 60% more likely to have greater knee pain severity (OR 1.6, 95% CI 1.4 to 1.9, p<0.0001) than those without temporal summation; at the wrist, the OR was 1.3 (95% CI 1.1 to 1.5, p=0.0008).
To test whether OA pathology must be present for some time prior to the occurrence of sensitisation (ie, a ‘state’ induced by OA pathology), we examined whether disease duration was associated with measures of sensitisation. As shown in table 3, this was not the case. There was no significant difference in adjusted mean PPT among the different durations of ROA or SOA. The mean difference in PPT among those with the longest duration of OA (radiographic or symptomatic) ranged from 0.1 lower to 0.1 higher than those without any OA in either knee. The likelihood of having temporal summation also did not increase with increasing duration of either ROA or SOA, with effect estimates centred about the null. Greater severity of radiographic changes, as a proxy for degree of tissue injury and/or inflammation that may lead to sensitisation, was also not associated with PPT or temporal summation (table 4).
Relation of duration of radiographic and symptomatic knee OA to PPT and temporal summation
Relation of radiographic severity of tibiofemoral OA with PPT and temporal summation
Addition of widespread pain to the models resulted in either no or <3% change in effect estimates. Because of the potential for pain to influence mood, we also ran models without depressive symptoms, but the effect estimates were not altered.
We examined correlations between anatomical sites because findings between the patella and wrist were similar. For PPT, correlations between the wrist and patella were 0.61–0.65, with higher correlations ipsilaterally. Correlations between the patellae bilaterally were 0.82. Correlations were lower for temporal summation: 0.53 between the patella and wrist, and 0.61 between patellae bilaterally.
Discussion
We comprehensively examined measures of sensitisation and sensitivity in relation to knee OA in a large well-characterised cohort. Extending the findings of prior studies in this large cohort, we found that PPT and temporal summation were associated with knee OA-related pain as well as greater knee pain severity.29 ,45 ,51 However, we could not demonstrate an association between ROA or SOA duration or severity with these measures. Importantly, in this study, these associations were independent of potential confounders, including psychological factors and widespread pain, suggesting these measures represent a phenomenon that is unique from psychological factors and propensity for generalised pain complaints.
Although prior studies have found differences in PPT and temporal summation in subjects with OA in comparison with predominantly healthy controls, such healthy controls may not be directly comparable with those with knee OA on many fronts. BMI is an important risk factor for pain, yet healthy controls tend to have lower BMI than those with knee OA.52 Healthy controls may also differ in other regards, such as comorbid psychological factors and pain elsewhere in the body, both of which are likely to be more prevalent in those with knee OA. The current study's sample included a mixture of individuals with symptomatic and asymptomatic radiographic OA, whereas other studies often relied on clinical OA, meaning that all individuals were symptomatic, while the controls were pain-free. Studies using healthy controls have therefore primarily assessed the difference between those with OA-related pain versus a pain-free, healthy status, without being able to provide direct insight into the role of OA itself as contributing to those findings.
In contrast to our findings demonstrating a significant relation of sensitisation/sensitivity to pain presence and severity, there was no association of either PPT or temporal summation with ROA and SOA duration or severity. We had hypothesised that disease must be present for a sufficient period of time and/or have a sufficient degree of tissue injury (or inflammation) for sensitisation to occur. However, we found no association between duration or radiographic severity of OA with sensitisation.
These sensitisation/sensitivity measures, therefore, do not seem to be directly related to the pathological abnormalities of OA. It is possible that we would need to evaluate knee OA at an earlier stage of disease to identify a relevant time period for development of sensitisation. Even so, if OA pathology was a key factor in inducing sensitisation (ie, if sensitisation were a ‘state’), one would expect longer duration and greater severity of the disease to be associated with greater likelihood of sensitisation. These findings raise the possibility that sensitisation is in fact a ‘trait’ rather than a ‘state’, that is, that hypersensitivity was present before knee OA, related to an individual's predisposition to sensitisation rather than being induced by peripheral nociceptive input from OA pathology. If it were a trait, there might be endophenotypical markers of risk of developing more severe pain related to lower pain thresholds or a heightened capacity to amplify pain signals. The underlying trait in an already-sensitised individual may be unmasked once nociceptive input is received from the pathological joint (ie, enhanced pain sensitivity is only noted upon nociceptive input). Other mechanisms, such as descending inhibitory or facilitatory pathways, may also influence the phenotypical manifestation of sensitisation/sensitivity.
We found similar results for the measures of sensitisation at the patella and at the wrist, and moderate to high correlations between measurements at the different anatomical sites. This may suggest that activity-dependent central sensitisation driven by OA pathology might not have been responsible because its effects tend to be quite local (a single limb) and instead that pain severity was related to generalised lower pain thresholds. However, whether OA in one joint can lead to sensitisation contralaterally and more globally within an individual in chronic diseases is an area that requires active investigation. A prospective study is needed to assess the temporal sequence of change in pain sensitivity and capacity for sensitisation.
While this study has several strengths as discussed above, limitations must also be acknowledged. Obtaining these measures in >2000 individuals necessitated feasible methods of assessing sensitisation/sensitivity. We focused on anatomical sites that were most likely to be of relevance to knee OA and a control site unlikely to be affected by OA. We did not have an automated system for continuous pain ratings during assessment of temporal summation, and therefore could not examine rate of change, which has been shown to differentiate OA from non-OA, and greater pain severity.29 Nonetheless, our measure of temporal summation was significantly associated with pain, lending face validity to this method. Radiographs cannot provide insight into particular pathologies that may contribute to sensitisation. Our study was cross-sectional, as this was the first clinic visit at which these measures were introduced. Therefore interpretation about directionality of relationships must be made cautiously. Causal pathways in OA are complex; we may have inadvertently adjusted for intermediates in the causal pathway that could bias results, but performed sensitivity analyses to evaluate for this and found no substantial changes in our effect estimates.
A number of implications arise from these study findings. First, a simple method of sensitisation/sensitivity assessment may help identify individuals at risk of greater pain severity and who may potentially benefit from centrally acting pain medications; this would need to be tested formally in a randomised trial. Second, despite advances in understanding of pain and greater attention on sensitisation in OA, mechanisms by which sensitisation may occur is yet to be clearly elucidated in humans. Such insights are needed to enable appropriate therapeutic targeting. Third, if sensitisation is related to the transition from acute to chronic pain, identification of new-onset sensitisation may have implications for timing of pharmacological, non-pharmacological and surgical interventions.
In summary, PPT and mechanical temporal summation locally and at a distance, were associated with OA-related pain presence and severity after accounting for pertinent confounders. However, we were not able to confirm the hypothesis that the pathology of OA contributes to sensitisation. Understanding mechanisms of pain hypersensitivity offers a promising strategy for optimising pain management in knee OA.
References
Footnotes
-
Handling editor Tore K Kvien
-
Contributors All authors of this paper have participated in the design of the study, data collection, analysis, interpretation, and writing or providing comments on the manuscript.
-
Funding NIH and Arthritis Foundation.
-
Competing interests The Multicenter Osteoarthritis (MOST) Study was supported by NIA U01 AG18820, U01 AG18832, U01 AG18947, and U01 AG19069. TN's work was supported by NIAMS K23 AR055127 and R01 AR062506, the Arthritis Foundation Arthritis Investigator Award, and NIAMS P60 AR47785.
-
Ethics approval BUMC, UCSF, UIowa, UAB.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This paper is from the Multicenter Osteoarthritis (MOST) Study.