Article Text

Abstract
Objective: To assess a patient’s out of pocket costs, income loss, time consumption, and quality of life (QoL) due to ankylosing spondylitis (AS) in three European countries and to assess variables predicting these outcomes.
Methods: 216 patients with AS from the Netherlands, France, and Belgium participated in a two year study. Health resource use, days absent from work, time lost, and quality of life (EuroQol) were assessed by bimonthly questionnaires. AS related healthcare and non-healthcare expenditure and income loss were calculated taking into account country-specific regulations. Predictors of costs, time consumption, and QoL were analysed by Cox’s regression.
Results: 209 patients provided data for cost analysis. Average annual healthcare and non-healthcare expenditure was €431 per patient and average annual income loss was €1371 per patient. Healthcare costs were highest for Belgian and lowest for French patients, while non-healthcare costs were highest for Dutch patients. A patient’s total costs were associated with higher age and worse physical function. On average, patients with AS needed 75 minutes additional time a day because of AS. Worse physical function and higher disease activity predicted time consumption. After adjusting for baseline confounders, QoL was worse in Belgian and French than in Dutch patients. Peripheral arthritis, worse physical function, higher disease activity, and loss of income contributed to worse QoL.
Conclusion: AS is time consuming and associated with substantial out of pocket costs. Belgian patients incur the highest healthcare payments. Poor physical function increases patient’s costs and time consumption. Loss of income is associated with lower QoL.
- ankylosing spondylitis
- costs
- patient’s perspective
- ANOVA, analysis of variance
- AS, ankylosing spondylitis
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- EQ-5D, EuroQol 5 dimensions
- HR, hazard ratio
- IBD, inflammatory bowel disease
- QoL, quality of life
- RA, rheumatoid arthritis
Statistics from Altmetric.com
- ANOVA, analysis of variance
- AS, ankylosing spondylitis
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- EQ-5D, EuroQol 5 dimensions
- HR, hazard ratio
- IBD, inflammatory bowel disease
- QoL, quality of life
- RA, rheumatoid arthritis
Traditional outcome measures aim to assess the impact of the disease on the patients themselves. However, in most economic analyses the costs of a particular disease are calculated from a point of view different from the patient’s perspective, such as the societal or the health insurer’s perspective. This is surprising, because not only can an illness have important economic consequences for patients, including out of pocket payments and income loss, but also the disease affects time consumption and quality of life (QoL), leading to intangible costs. Recently we performed a cost of illness study among patients with ankylosing spondylitis (AS) in three European countries, the Netherlands, France, and Belgium. Results of the productivity costs have been published previously1 and the results for the direct healthcare and non-healthcare costs from a societal perspective are published in this issue of the Annals (see p 732). In the present analysis we determine the costs, time consumption, and quality of life (QoL) due to AS, for patients with the disease. Patient’s costs, time consumption, and QoL are compared among three countries. In addition, determinants of these outcomes are explored.
PATIENTS AND METHODS
Patients
Patients were recruited from the rheumatology departments of four hospitals in three European countries, the University Hospital Maastricht and the Maasland Ziekenhuis Sittard in the Netherlands, Hôpital Universitaire Cochin Paris in France, and the University Hospital Gent in Belgium. For detailed description we refer to the related article on the societal costs (see p 732). Patients were included between September 1996 and March 1997 and were followed up for two years.
Questionnaires
For the description of the type and the time points of the clinical and economic assessments see the article on the direct societal costs (p 732). In addition, patients reported in the bimonthly economic questionnaires the days on which they could not perform paid work and the hours of time per day or week lost because of AS. In the six-monthly questionnaires patients had to report changes in job, working status, and income. Also, every two months patients completed the EuroQol 5 dimensions (EQ-5D) questionnaire.
Health insurance system and social security system of the three countries
A description of the healthcare system and social security system from the point of view of the patients’ contributions and income loss due to sick leave or work disability can be found in Appendix 1 of the online version of the article. The three countries have an insurance based social security system. For healthcare, people in the Netherlands have higher premiums and social taxes than both the other countries, while in France and Belgium a patient’s contributions for healthcare visits or procedures and a patient’s contributions for drugs are considerably higher. In France, patients with a severe chronic disease (such as severe AS) can be exempted from such contributions, whereas this possibility does not exist for patients with AS in Belgium. For sick leave and work disability the benefits in the Netherlands are in general more favourable than in both other countries.
Healthcare resource use and time consumption
AS related healthcare and non-healthcare resource use, absence from paid work due to sick leave or chronic work disability, and time consumed due to AS were assessed. Effects of spinal and extraspinal (peripheral arthritis, inflammatory bowel disease, psoriasis, uveitis) manifestations of AS and of the side effects of drugs were included. Patients received extensive instruction on how to complete the questionnaires, especially how to interpret AS related and non-AS related resource use at the start of the study and with each repeat questionnaire. For detailed description of resources included in healthcare use and in non-healthcare use see the article on direct societal costs (p 732). In addition, absence from paid work due to sick leave (expressed as number of working days absent from paid work) was assessed in the bimonthly economic questionnaires, and changes in working hours, work disability, and income were assessed in the six-monthly economic questionnaires. Finally, time loss because of disease comprised the number of hours the patients spent daily in resting and exercising at home, time lost because of in- or outpatient health care, time lost because of participation in group physical exercise or swimming group, and time lost because of AS related absence at paid work. If a patient mentioned admission to hospital or healthcare visits and reported at the same time absence from paid work, the time absent from work was subtracted from the total loss of time. Resource use, absence from work, and time consumption were not ascertained by comparison with other data sources.
Definition and sources of costs
Costs were calculated from the patient’s perspective. Expenditures for healthcare related resources are called healthcare patient costs. Expenditures for non-healthcare resources are called non-healthcare patient costs and income loss refers to loss of income because of days absent from paid work (sick leave) or chronic work disability. Total patient costs comprise the sum of healthcare, non-healthcare patient costs, and income loss.
For the healthcare patient costs the official country-specific patient contributions were used for each unit of healthcare resource.2–9 Specific national regulations on reimbursement of costs were taken into account. For example, Dutch and Belgian patients with AS can be granted reimbursement for physiotherapy for an unlimited number of sessions a year. For alternative medicine, we assumed that patients only visited recognised doctors for which there is reimbursement for a regular visit. During the period of our study, Dutch patients had to pay the first €45.45 per year of healthcare costs and €3.6 per day in hospital. A patient’s out of pocket costs were not corrected for differences in social contributions among countries. Patients with additional private insurance had difficulty in reporting the additional premium because this was often included in the total premium for the entire family. Moreover, the kind and level of additional financial advantage for the patient (complete reimbursement, reimbursement higher or lower than a maximum limit, reimbursement of provisions not included such as alternative medicine or extra number of physiotherapy sessions) was very variable. Therefore we proposed that the premium for the private insurance would balance out the exemption from personal contributions.
For the non-healthcare patient costs, a patient’s reported financial contributions were used whenever available. If these were missing, costs as reported by other patients from the same country for the same resource were used. For travel costs the variable costs per kilometre, based on the country-specific mean fuel prices over the period studied, were used. For help from private paid household help, the country-specific mean wage of a female manual worker was used as reported for 1998 by Eurostat (€11.00 per hour in the Netherlands; €10.25 per hour in France, and €12.00 per hour in Belgium).10 All known sources of reimbursement to the patient were taken into account.
Where applicable, taxes were included in the costs prices. All costs were expressed in euros (31 December 1998 currency). The currency of one euro was set at NLG 2.20, FF 6.56, and BEF 40.34. On the same date €1.00 was worth $1.17.
An overview of the sources used to calculate a patient’s out of pocket costs can be found in Appendix 2 of the online version of this article.
Statistical analyses
Results are analysed for patients who completed two years’ follow up and who filled out at least nine of 12 bimonthly questionnaires. For missing values of healthcare resource use in the bimonthly questionnaires, the mean for the same patient of the completed questionnaires was imputed. Demographic and disease characteristics are presented using descriptive statistics. The EQ-5D questionnaire was calculated using the patients’ ratings and transformed into a utility scale ranging from zero (death) to one (perfect health) by applying the York weighting.11 To better represent the overall QoL during the two year follow up, the time averaged EQ-5D was used in the analysis. Differences in the variables among countries were assessed by χ2 for proportions and by analysis of variance (ANOVA) for continuous variables. For healthcare resource use, firstly, the proportion of patients who had used this resource over the period studied was assessed, next the mean annual number of units of each resource was ascertained, and finally, the annual out of pocket costs or time consumed per resource were calculated. Because the distribution of costs and time was skewed not only means but also medians are presented to provide a better illustration of the distribution. Bootstraps with 10 000 replications were computed to assess the 95% confidence of the costs and to assess the 95% confidence interval of the difference in the costs among the three countries.12
Determinants of costs, time consumption, and QoL were explored by Cox’s proportional hazard regression analyses with out of pocket costs, time consumption, or QoL as dependent variable. As independent variables several sociodemographic and baseline disease characteristics were chosen: gender, age, disease duration since diagnosis, educational level (dichotomised into ⩽12 years’ or >12 years’ formal education), presence of peripheral arthritis, presence of inflammatory bowel disease (IBD), the Bath Ankylosing Spondylitis Functional Index (BASFI; range 0–10) measuring physical function, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI; range 0–10) measuring disease activity, and country (dummy). When assessing determinants of the EQ-5D utility score, time averaged BASFI and time averaged BASDAI were used within the independent variables. Because differences of the outcomes among the countries were our primary interest, the dummy country was entered into a first block and all other variables in a second block using a backward elimination likelihood procedure. Interactions between the variables of the final model and country were explored. Cox’s proportional hazard regression analysis is a semiparametric statistical analysis and was chosen because cost and time data had a skewed distribution. Reported hazard ratios (HRs) >1 indicate that the independent variable is associated with an adverse outcome (higher costs, more time lost, or worse quality of life). For example, an HR of 1.5 of a dichotomous variable, indicates a 1.5 times increase in (median) costs or decrease in (median) QoL. All regression analyses were repeated by eliminating patients with extreme values and by including and excluding patients with extraspinal disease.
Bootstraps were performed in Excel and all other statistical analyses in SPSS 9.0.
RESULTS
Patients
In total 216 (135 Dutch, 54 French, and 27 Belgian) patients with AS fulfilled modified New York criteria and started the study. In the course of the follow up five Dutch, one French, and one Belgian patient dropped out. All patients who completed the follow up had filled out at least nine of 12 questionnaires. The proportion of patients with one, two, or three missing bimonthly questionnaires was 84%, and the proportion of missing questionnaires was 10%, of which 25% were missing at random because some patients had not received one of the bimonthly economic questionnaires owing to an administrative error. Table 1 presents, for each country separately, the sociodemographic characteristics of patients who completed the study. A comparison of patient characteristics among countries showed that Dutch patients were older, had on average a lower educational level, and reported worse physical function (BASFI). None of the French patients had concomitant IBD. Of the Dutch patients, 77% had public insurance and 23% private. Of the French patients, 72% were completely reimbursed by the Securité Sociale (Social Security System) and 4% had additional private insurance. Of the Belgian patients, 4% had additional insurance for costs of hospital admissions.
Characteristics of patients completing the study
Healthcare resource use and patient’s costs
The overall mean total annual patient’s costs (healthcare costs, non-healthcare costs, and income loss combined) were €1795 (median €351) per patient (table 2). Income loss accounted for 76% of the total patient costs. For healthcare and non-healthcare costs combined, the non-healthcare costs were the cost drivers, comprising 40% of the out of pocket expenditure for private household help, 15% for transportation costs, and 9% for contributions to societies or exercise or swimming groups. In univariate analysis, total patient’s costs and non-healthcare costs were higher in the Netherlands than in France and Belgium. The Belgian patients had the lowest non-healthcare costs and the highest healthcare patient’s contributions, reflecting the higher resource use but also the higher patient copayments for these cost categories in this country. In multivariate analysis, country was the only variable significantly contributing to the variation in a patient’s healthcare out of pocket costs (table 3). Higher patient’s non-healthcare costs could be predicted by living in the Netherlands but also by female gender and worse physical function (table 3). The association between female gender and non-healthcare costs could be explained by the high costs due to private household help in female patients (data not shown separately). Income loss was associated with worse physical function (BASFI). Finally, total patient costs were associated with worse physical function (BASFI) but also with higher age (table 3). After eliminating from the regression analyses the patients with extreme values or patients with extraspinal disease, the regression coefficients did not change importantly (data not shown separately).
Comparison among countries of the annual healthcare resource use and annual out of pocket costs per patient
Determinants of patient’s out of the pocket costs assessed by Cox’s regression analyses
Time consumption
Table 4 illustrates the amount of time patients with AS lose because of disease for different time categories. Excluding the time lost because of sick leave, patients with AS lose on average 1.25 hours a day because of the disease. More than 75% of this time loss is due to time needed for additional daytime rest and time to exercise; 71% of patients reported taking regular rest at home and on average patients rest for 40 minutes a day; 62% of patients reported exercising regularly at home and on average a patient exercises for 19 minutes a day. An average visit to a healthcare provider consumes two hours of a patient’s time, a visit to the physiotherapist one hour, and attending group physical exercises takes on average two hours. Technical procedures last on average one hour. It is of note that travel and waiting time are included, if applicable. There were no important differences in the amount of disease related time consumption across countries. Worse physical function (BASFI) (HR=1.12; 95% CI 1.03 to 1.20) and higher disease activity (BASDAI) (HR=1.15; 95% CI 1.04 to 1.27) were predictors of the amount of total time lost. In addition to personal time lost, 7.6% of patients reported needing regular help from family or friends. Time invested in AS by family or friends was 4.6 minutes a day if averaged over all patients with AS, but 60 minutes (median 35) a day if averaged over patients requiring this type of help (in each country 7.5% of patients).
Annual time consumption (hours per patient) due to AS for different categories of time loss
Relation with QoL
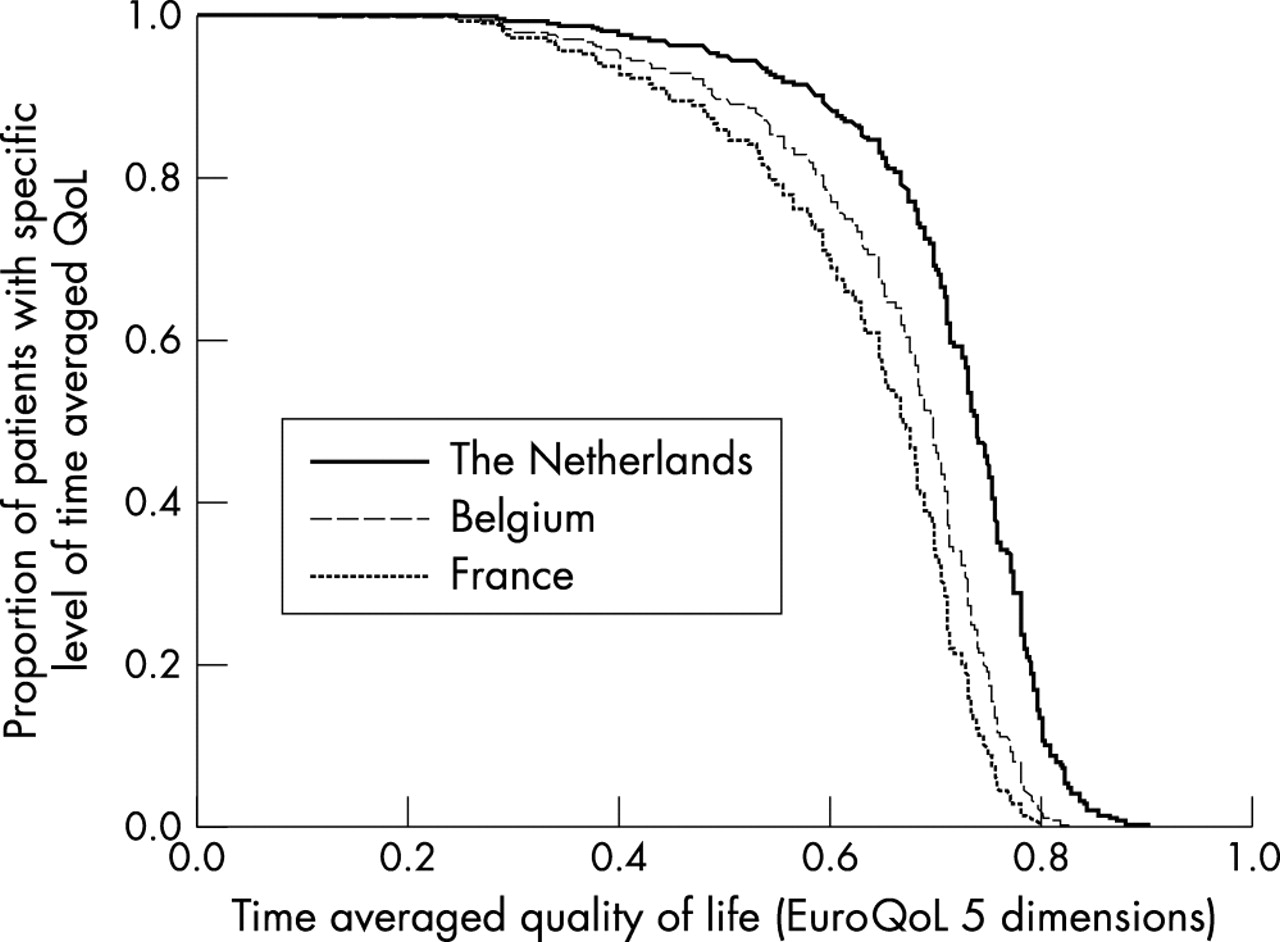
There was no difference in time integrated QoL (assessed by EQ-5D) in univariate analysis across the countries. However, after adjusting for sociodemographic and disease characteristics, QoL was worse in France and Belgium than in the Netherlands. As can be seen in table 5, lower education, presence of peripheral arthritis, worse physical function, and higher disease activity were additional determinants of a worse quality of life. An interaction was seen between educational level and country and also between the presence of peripheral arthritis and country. The effect of education on QoL was stronger in the Netherlands and the effect of peripheral arthritis on QoL was stronger in France. When the different categories of patient’s costs, time consumption, or income were added one by one to the independent variables of the regression model, only higher income loss (HR for occurring income loss 1.41; 95% CI 1.04 to 1.92) was significant, with a small but significant deterioration in QoL. No interactions between the variables of the final model and QoL were found. Cox’s analysis permitted computation of survival curves and visualisation of the difference in QoL among the countries. Figure 1 illustrates, for example, that a QoL of 0.7 or better is reported by 60% of Dutch patients as compared with 30% of French patients.
Determinants of time integrated quality of life assessed by time averaged EuroQol-5 dimensions assessed by Cox’s regression analyses
{kind=link}
Survival curve illustrating the proportion of patients reporting a specific level of quality of life (QoL) for each country separately.
DISCUSSION
For the patients, AS is a time consuming disease and associated with substantial out of pocket costs and loss of income. On average, patients with AS need 75 minutes additional time per day because of their disease. Seventy eight per cent of this time is spent on daytime rest and exercises at home. Patients with a worse physical function, higher disease activity, and peripheral arthritis lose more time. Among 84 Dutch patients with rheumatoid arthritis (RA) the average time consumption was 110 minutes a day within the first six years of disease.13 As in our study, this could be mainly attributed to the need for additional rest but also to extra time needed to perform usual daily activities, a type of time loss not registered in our study. Similarly, worse physical function was associated with more time consumption.
Apart from time consumption, patients also have considerable out of pocket expenditure because of their disease and substantial income loss. The mean total annual patient’s costs amounted to €1795 (median €351) per patient, of which 76% were due to income loss because of work disability or sick leave. The inventory of out of pocket costs was rather conservative because some personal extra expenditure, such as extra costs for heating the house and for extra clothing (for example, sportswear), were not included in the questionnaires. Also, we assumed that patients out of pocket costs for alternative medicine equalled a contribution for a regular visit to a doctor. This will possibly be an underestimation of these costs.
Important differences in patient out of pocket payments among the three European countries were noted. Owing to the characteristics of the national healthcare organisations, with high out of pocket payments in Belgium, patients with AS in that country have substantially more healthcare contributions. Also in France, out of pocket payments are part of the healthcare system. However, in France the system includes exemption from financial contributions for patients with a (severe) chronic disease (such as severe AS), reducing substantially the overall healthcare contributions. In our study, 87% of French patients had this special status. Interestingly, the higher patient contributions in Belgium did not result in lower healthcare use. Strong belief in the effectiveness of medical care and supplier induced demand may help to explain this phenomenon.
Although Belgian patients had the highest healthcare expenditure, they had the lowest non-healthcare expenditure and the lowest income loss, resulting in the lowest total patient costs. In contrast, Dutch patients had high expenditure for aids and adaptations, formal and informal help, and financial contributions to societies or exercise groups. They also had a greater loss of income. These high patient costs were seen despite higher reimbursement rates for aids and adaptations and for formal care and by the relatively more favourable sick leave and work disability benefits in Belgium compared with both other countries. Apparently, the more favourable reimbursement and benefit schedules may be an incentive for resource use, prolonged sick leave, and work disability. Also, different health beliefs and cultural attitudes towards paid employment despite disease may explain some of the differences. In this part of the study, health beliefs, coping with disease, or willingness to pay for health have not been assessed and their possible contribution to differences in healthcare use and sick leave or withdrawal from work cannot be explored.
Country was not the only predictor of the total patient costs. Older age and worse physical function were also associated with higher patient costs. In addition, non-healthcare costs were higher in female patients and this could be attributed to the expenditure for private household help. We found a recent publication on disease related healthcare and non-healthcare out of pocket expenditure in RA among Australian patients with a mean disease duration of 15.6 years.14 Converted to 1998 values by consumer price indices and expressed in euros, the annual out of pocket costs were €968 (SD 1700) per patient, which is considerably higher than in our patients with AS. Similar, however, was that female gender and longer disease duration were associated with higher out of pocket expenditure. Whereas we showed significant differences in patients’ costs among countries, the Australian study showed differences in patients’ costs among groups with different insurance schemes (pensioners paying less and privately insured patients more), reflecting the important influence of organisational aspects on a patient’s costs.
Perceived QoL, as a substitute for the intangible costs, was significantly better in Dutch patients and in those with higher education, no peripheral joint disease, better physical function, and lower disease activity. Although Dutch patients more often had lower education and had somewhat worse physical function, they experienced a better QoL than patients in both other countries. Unknown factors or variables not measured such as health beliefs and coping with disease may be important contributors to QoL. Interestingly, while income was not associated with reduced QoL, income loss due to work disability resulted in a worse QoL.
During the study, none of the patients were treated with one of the new biological drugs. Because worse physical function is a predictor of patient’s out of pocket costs, income loss, time consumption, and QoL and because the new biological treatments have a proven effect on physical function, it seems likely that these drugs can substantially improve economic outcome for the patients.
The limitations of the study have been discussed in the article on the direct costs from a societal point of view (see p 732). It should be noted that the differences in patient’s expenditure among the countries should be interpreted in the light of differences in social contributions and insurance premiums. The higher social contributions and insurance premiums in the Dutch population together with the low patient copayment imply a higher social solidarity in this country. Finally, it was impossible to correct a patient’s costs for additional private insurance (to cover expenditure not included in the insurance package). We suggested that the premium for the additional insurance would balance out the copayments but could not ascertain that this hypothesis was correct.
In conclusion, for patients with AS, the disease is time consuming and associated with substantial out of pocket costs, income loss, and reduction in quality of life. There are striking differences in patient’s costs and the QoL experienced among countries. In all countries, patients with worse physical function lose more time, have the highest total costs, and experience a worse QoL.
Acknowledgments
We thank Willy Peeters for providing information on the Belgian healthcare system, Maryse Meziere for providing additional information on the French patients, Christel Grimbergen, Sandra Boesen, and Erik de Klerk for developing the database.
Supplementary materials
. Web-only Appendices
the 2 Appendices are available here as PDFs (printer-friendly files)Files in this Data Supplement:
- [View Appendix 1] - Description of the health insurance system and social security system in view of patients' contributions and patients' loss of income.
- [View Appendix 2] - Country-specific regulations on patient's out-of-pocket payments.