Article Text

Abstract
Background: Synovial biopsies are used to study synovial immunopathology and are increasingly applied for the evaluation of new therapeutic strategies in chronic arthritis. Therefore, it is essential to be informed on the complete spectrum of synovial immunopathology.
Objective: To describe the cellular content, cytokine and cell adhesion molecule expression in synovial tissue from clinically and arthroscopically normal knees.
Methods: Synovial tissue was obtained from 20 normal subjects at the time of knee joint arthroscopy for unexplained knee pain. Tissue sections were studied for basic histopathology and for a range of cell surface markers, cytokines, and cell adhesion molecules by immunoperoxidase staining. Stained sections were evaluated by semiquantitative scoring and digital image analysis.
Results: Normal synovial tissue is composed predominantly of fibrofatty areolar tissue, with a variable thickness of intimal lining, composed of both CD68 positive macrophages and CD55 positive fibroblast-like synoviocytes. Interleukin 1 receptor antagonist (IL1Ra) was frequently detected in the synovial membrane of normal subjects (mean (SD) integrated optical density (IOD)=3809.6 (3893.9)), but both tumour necrosis factor α (TNFα) and interleukin 1β (IL1β) were rarely detected. In addition, cell adhesion molecules were rarely detected in the normal synovial membrane, with the exception of intercellular cell adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1). Osteoprotegerin (OPG) expression was abundant on synovial lining macrophages (mean (SD) IOD=5276 (4716) as well as endothelial cells (mean (SD) IOD=557 (226)), but receptor activator of nuclear factor κ ligand (RANKL) expression was rarely seen.
Conclusions: The normal synovial membrane has a variable architecture, including thickness of the lining and the subintimal cell infiltrate, with little inflammatory cytokine production or expression of cell adhesion molecules. The excess of OPG expression over RANKL and IL1Ra over IL1 may be important for protection against joint damage
- synovial tissue
- knee
- microarchitecture
- ICAM-1, intercellular adhesion molecule-1
- IL, interleukin
- OPG, osteoprotegerin
- IL1Ra, interleukin 1 receptor antagonist
- RA, rheumatoid arthritis
- RANKL, receptor activator of nuclear factor κ B ligand
- TNFα, tumour necrosis factor α
- VCAM-1, vascular cell adhesion molecule-1
Statistics from Altmetric.com
- ICAM-1, intercellular adhesion molecule-1
- IL, interleukin
- OPG, osteoprotegerin
- IL1Ra, interleukin 1 receptor antagonist
- RA, rheumatoid arthritis
- RANKL, receptor activator of nuclear factor κ B ligand
- TNFα, tumour necrosis factor α
- VCAM-1, vascular cell adhesion molecule-1
Synovial biopsies are increasingly used to study synovial immunopathology where single synovial samples have provided valuable information on the mechanisms involved in chronic inflammatory joint diseases such as rheumatoid arthritis (RA), osteoarthritis, reactive arthritis, spondyloarthropathies, and various other inflammatory joint diseases.1–4 Over the past decade, serial synovial samples have provided accumulating evidence on the response of patients with a chronic inflammatory joint disease to disease modifying antirheumatic drug treatment.5,6 Synovial samples have been shown to provide information on factors involved in clinical signs of arthritis7 and clinically relevant situations such as treatment induced remission.8 Moreover, currently, samples can be obtained from both large and small joints.9 All these results support the use of serial synovial samples as surrogate markers in studies evaluating new treatments in small cohorts of patients.5,6
In this situation it is essential to be informed on the spectrum of synovial inflammation. There have been a few publications dealing with the microscopic architecture of the normal synovial membrane.10–20 Where studies did examine normal synovial tissue it was usually as a control for studies on the synovial membranes from patients with RA or osteoarthritis. In addition, the source of this “normal” synovial tissue was often anything but normal, usually obtained at post mortem or from limbs amputated for peripheral vascular disease or musculoskeletal tumours. These studies had small numbers of “normal” subjects,3–10 sometimes from a range of joints rather than a single joint and only evaluated the expression of a limited number of cell surface markers, cytokines, or cell adhesion molecules. In addition, there was little consensus among the studies on the expression of these molecules, particularly in relation to cytokine expression, which may be because of the heterogeneity of the source of the “normal” tissue.
Our research group has been accumulating synovial tissue specimens obtained from apparently normal knee joints at the time of knee joint arthroscopy for unexplained knee pain for several years. This normal synovial tissue bank was used to demonstrate the range of immunopathological features seen in the normal synovial membrane. Thus, the pathophysiological changes in the synovial membrane from patients with a range of inflammatory arthritides could be compared and contrasted with those seen in normal synovial tissue.
PATIENTS AND METHODS
Patients
Synovial membrane biopsy specimens were obtained from a group of patients attending a sports medicine day surgical facility for knee arthroscopy for unexplained knee pain, as previously described.4 All patients were examined by one author (MDS), who took a history of any arthritis, carried out a physical examination, and assessed the laboratory and radiological investigations. In addition, all subjects were re-evaluated at five years after knee arthroscopy to determine whether any arthritis had developed in the previous five years.
Immunohistochemical labelling
Twelve synovial biopsy specimens were obtained from each patient, and were processed as frozen tissue as well as formalin fixed and paraffin embedded tissue. Immunohistochemical labelling was performed by a three step immunoperoxidase technique, using 3-amino-9-ethyl-carbazole as colour substrate, as previously described.8,21 Primary monoclonal antibodies included anti-CD3 and CD38 from BD Biosciences, San Jose, CA, USA; CD55 (Serotec Ltd, Oxford, UK); CD68 (EBM11 clone) and antihuman von Willebrand factor (factor VIII) all from Dako Australia (Botany Bay, New South Wales, Australia); CD22 (Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands); granzyme B, intercellular adhesion molecule-1 (ICAM-1), E-selectin, and vascular cell adhesion molecule-1 (VCAM-1) all from Novo Castra Laboratories, Newcastle upon Tyne, United Kingdom; receptor activator of nuclear factor κ B ligand (RANKL) and osteoprotegerin (OPG) from R and D systems, Minneapolis, MN, USA; and anti-interleukin 6 (IL6; B-E8, Biosource, Nivelles, Belgium). All synovial tissue was labelled with each antibody in a single run on the same day. A positive control (synovial tissue from a patient with RA with a known staining pattern) as well as negative controls (omission of the primary antibody and use of an irrelevant antibody of the same immunoglobulin subclass as the primary antibody) were included in each immunohistochemical labelling run.
Histopathological analysis of synovial membranes
All synovial biopsies were processed for standard haematoxylin and eosin staining and were analysed by one trained histopathologist (MC), using a standardised grading system which has been previously described.4 The synovial biopsies were graded in relation to the presence of exudates, details related to the intimal lining, blood vessels, stromal characteristics, and inflammatory infiltrate in the subintimal regions of the synovial membrane, and the presence of crystals or foreign material.
Measurement of immunohistochemical labelling
Both a semiquantitative score and computer assisted digital video image analysis were used to measure immunohistochemical labelling, as previously described.8,21–23 All measurements for each antibody were performed on the same day. Video image analysis was performed by one author (EB), using a Videopro System (Leading Edge Pty Ltd, Adelaide, South Australia), as previously described. Semiquantitative scoring was performed by two authors (EB and MDS), using a five point scale (0–4), as previously described.8,21 Each assessor was unaware of the other assessor’s score and differences in scoring were resolved by consensus. In addition, cellular content of synovial membranes was measured by counting the number of cells in a defined area of the synovial membrane using a graduated lens, as previously described.21
Statistical analysis
Descriptive statistics were generated using a statistical package, SPSS 10.0.
RESULTS
Patients
Twelve men and eight women, with a mean age of 33 years (range 18–54), were studied. None of the patients had clinical, laboratory, or radiological signs of an inflammatory or degenerative arthritis. No patient was taking a non-steroidal anti-inflammatory drug at the time of knee arthroscopy.
Synovial tissue analysis
In general the normal synovial membrane histopathology consisted of fibrofatty tissue, blood vessels, and a variable but small cellular content, with scattered macrophages and mononuclear cells, but no plasma cells.
The intimal lining layer was of variable thickness, consisting predominantly of CD55 positive fibroblast-like cells, with a smaller content of CD68 positive intimal macrophages (tables 1 and 2, fig 1). The mean (SD) thickness of the intimal lining layer was 2.6 (0.5) (range 2–3) with some villi seen in 15 of the synovial biopsies.
Cellular infiltration, expression of adhesion molecules and cytokines in normal synovial membranes. Results depict the mean semiquantitative score (0–4) with standard deviation and range
Cellular infiltration, expression of adhesion molecules and cytokines in normal synovial membranes
{kind=link}
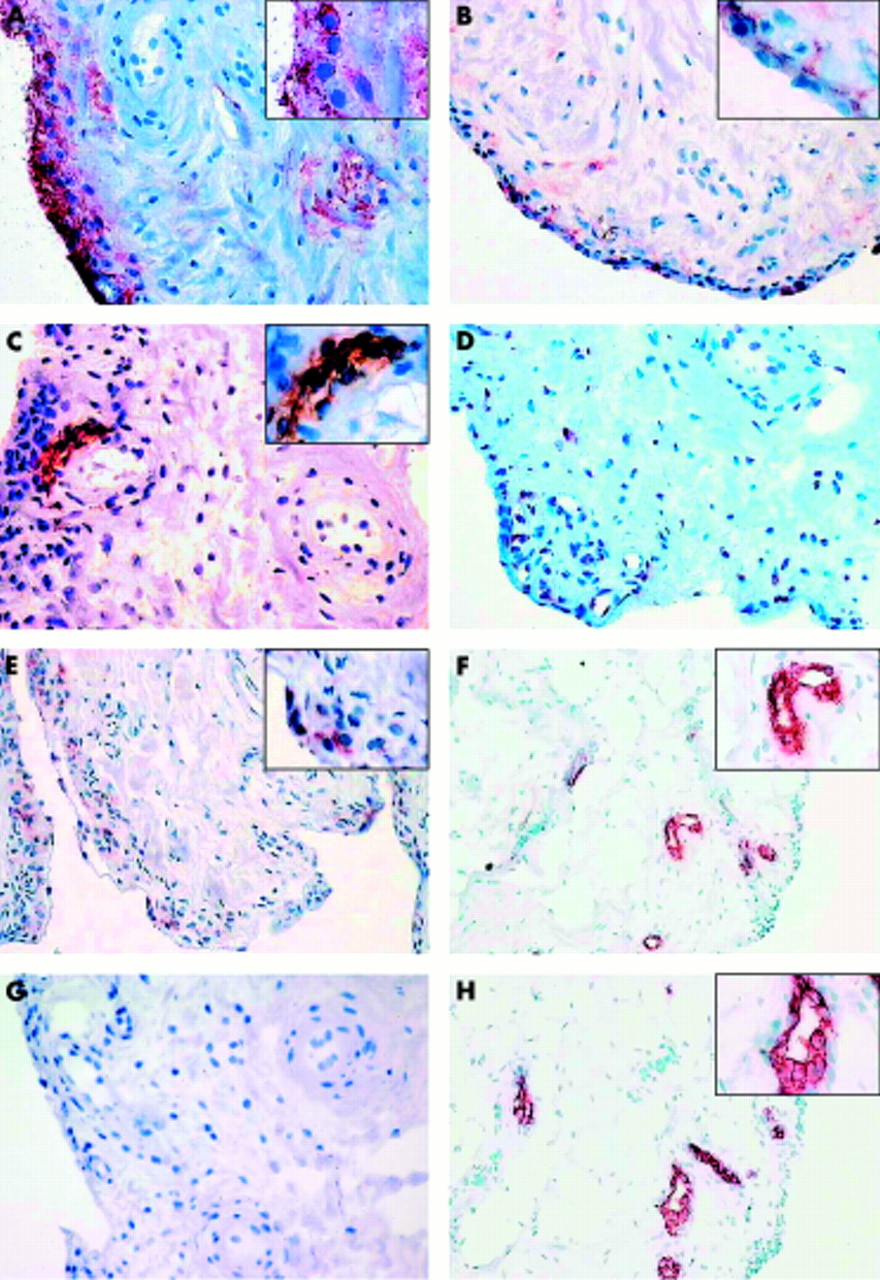
Immunohistochemical labelling of a representative normal synovial membrane stained with (A) anti-CD55 (fibroblast-like synoviocytes), (B) anti-CD68 (macrophages), (C) anti-CD3 (T cells), (D) anti-IL1β, (E) anti-interleukin 1 receptor antagonist (anti-IL1Ra), (F) anti-factor VIII (endothelial cells), (G) anti-RANKL, and (H) monoclonal antibody 805 for OPG. All images are at ×200 magnification except F and H, which are ×100 magnification. All inserts in panels A, B, C, and E are ×400 magnification, while inserts in panels F and H are ×200 magnification.
There was a small amount of blood vessel proliferation in the synovial sublining (0.9 (0.5)) as well as stromal oedema (0.8 (0.6)), and fibrosis (0.8 (0.9)) (all evaluated on a semiquantitative 0–3 scale). There was very little inflammatory infiltrate, although two synovial membranes had a focal and two a diffuse inflammatory cell infiltrate, all of which were graded as minimal (grade 1 on a scale of 0–3). This infiltrate consisted predominantly of macrophages and fibroblast-like cells, with a small number of infiltrating lymphocytes. Few B cells (CD22+) were seen, scarce numbers of CD45RO+ cells, and rarely any plasma (CD38+) cells.
The normal synovial membrane contains little in the way of proinflammatory cytokines, but a substantial content of IL1Ra, a natural antagonist of IL1 (tables 1 and 2, fig 1).
There was little expression of cell adhesion molecules in either the intimal lining layer or the synovial sublining (tables 1 and 2), ICAM-1 expression was mainly found on endothelial cells, while VCAM-1 was predominantly expressed by fibroblast-like synoviocytes, as assessed by immunostaining of sequential sections of synovial tissue for CD68 (macrophages), VCAM-1, and CD55 (synovial lining fibroblasts). These results are similar to those previously reported in published studies.19,20
There was strong expression of OPG both in blood vessels and synovial lining cells, but little, if any, RANKL expression (fig 1, table 2), resulting in a low RANKL to OPG ratio (table 2).
DISCUSSION
The normal synovial membrane is stated to be a relatively acellular structure consisting of a distinct intimal lining layer of 1–2 cells thickness and a synovial sublining. The latter is relatively acellular, containing scattered blood vessels, fat cells, and fibroblasts, with few lymphocytes or macrophages. This contrasts with inflammatory arthritis, such as RA, where the intimal lining layer is markedly thickened, mainly due to an increase in CD68 positive macrophages, with a heavily infiltrated subintimal region, containing T and B lymphocytes, plasma cells, and macrophages, associated with stromal oedema and proliferation of blood vessels. There is an increased production of a number of cytokines and widespread expression of cell adhesion molecules.5,6,21–23
However, there are few published studies investigating the range of architectural changes, production of cytokines, and anti-inflammatory mediators or expression of cell adhesion molecules in the normal synovial membrane.10–20 This study has shown that while the appearance of the normal synovial membrane as stated in rheumatology textbooks is largely correct, there is considerable variation in cell lining and subintimal characteristics of the synovial membrane between subjects, with some normal synovial membranes demonstrating a modest subintimal cell infiltrate, including T lymphocytes and macrophages, but not B lymphocytes or plasma cells. Although it might be argued that some of these synovial membranes were not from normal subjects, the lack of any pathological condition after a five year follow up of all subjects included in this study would suggest that this explanation of the results of this study is unlikely. Although all patients had unexplained knee pain before arthroscopy, the synovial membrane and articular cartilage were macroscopically normal at arthroscopy, and no patient included in this study had any mechanical derangement within the knee (such as meniscal or cruciate ligament tear). In addition, no patient had any evidence of any type of arthritis at a five year follow up after obtaining synovial tissue at the time of knee arthroscopy. This would suggest that the synovial tissue that we have studied is more homogeneous and closer to normal than that included in previous studies (amputation specimens for sarcoma or peripheral vascular disease, postmortem specimens, etc), although it might still be argued that the source of this synovial tissue (patients without any form of arthritis with unexplained knee pain and a normal knee arthroscopy) is still not from completely normal subjects. There was little expression of proinflammatory cytokines, such as TNFα, IL1β, or IL6, in the normal synovial membrane, but considerable expression of IL1Ra, similar to the findings of some11,15 but not other13,14 published studies. The reasons for this discrepancy in the results is likely to relate to the source of “normal” synovial tissue. The excess expression of IL1Ra over proinflammatory cytokines may be important to maintain an anti-inflammatory environment in the normal joint to protect bone and hyaline cartilage from cytokine mediated damage.
OPG is an alternative, high affinity decoy receptor for RANKL, which blocks the interaction between RANKL and receptor activator of nuclear factor κ B (RANK) and significantly inhibits osteoclastogenesis.5 It has been suggested that the ratio of OPG to RANKL expression in the synovial membrane, especially at sites close to cartilage, may be important in regulating osteoclast formation and regulating bone destruction.5,24 It is therefore likely that the excess OPG expression in the normal synovial membrane with a low RANKL:OPG ratio is necessary for appropriate expression of osteoclast production in the normal, non-inflamed joint. In addition, there is some evidence to suggest that endothelial cell expression of OPG is important in homoeostasis and prevention of vascular calcification.25 This suggests that the marked expression of OPG by endothelial cells demonstrated in this study is important for the normal function of the blood vessels in the normal synovial membrane.
In conclusion, this is the first study to demonstrate the range of relevant structural characteristics of the normal synovial membrane, which may be important for a comparison with the pathological changes found in the chronically inflamed synovial membrane seen in inflammatory arthritides such as RA. In addition, this study suggests that the excess OPG expression over RANKL, and IL1Ra over IL1, plays a part in bone and cartilage homoeostasis.