Article Text

Abstract
Objectives: To describe the histological changes in acute enthesopathy in early spondyloarthropathies (SpA).
Methods: Clinically evident acute enthesopathy was confirmed by magnetic resonance imaging and ultrasonography in four cases of plantar fasciitis and one case of patellar tendon enthesitis. Ultrasound guided biopsy of insertional points was carried out with a Jamshedi needle. Control tissue was obtained from two subjects undergoing spinal grafting surgery. Standard histochemistry and immunohistochemistry analysis using the avidin-biotin immunoperoxidase complex method employing markers against CD3, CD8, CD34, and CD68 was used to determine cellular infiltrates at the insertion point.
Results: The enthesis architecture was abnormal in the SpA group, with increased vascularity and cellular infiltration compared with normal subjects. The predominant infiltrating cell at the enthesis fibrocartilage was the macrophage, but there was a paucity of lymphocytes at the insertion point.
Conclusion: These preliminary findings have implications for a better understanding of the pathology in early SpA.
- enthesitis
- spondyloarthropathy
- magnetic resonance imaging
- histology
- ABC, avidin-biotin immunoperoxidase complex
- AS, ankylosing spondylitis
- FOV field of view
- FS, fat suppressed
- NSA, number of signals averaged
- SE, spin echo
- SpA, spondyloarthropathies
- TBS, Tris buffered saline
- TE, time to echo
- TNFα, tumour necrosis factor α
- TR, repetition time
Statistics from Altmetric.com
- ABC, avidin-biotin immunoperoxidase complex
- AS, ankylosing spondylitis
- FOV field of view
- FS, fat suppressed
- NSA, number of signals averaged
- SE, spin echo
- SpA, spondyloarthropathies
- TBS, Tris buffered saline
- TE, time to echo
- TNFα, tumour necrosis factor α
- TR, repetition time
The enthesis is the point of insertion of ligament, tendon, or joint capsule to bone. Inflammatory involvement of the enthesis or enthesitis is a characteristic feature of the spondyloarthropathies (SpA) and is regarded as the primary lesion, especially in ankylosing spondylitis (AS).1,2 Several studies have reported the histological findings from sites of spinal enthesitis in SpA, where inflammatory cell infiltration within and adjacent to spinal insertions in chronic AS was noted.3 More recently, some studies reported the histology and immunohistochemical features from the bone adjacent to entheseal sites from the sacroiliac4–7 and synovial joints8 in both early and established disease. These studies confirmed the presence of an inflammatory cell infiltrate containing myeloid cells and lymphocytes. However, there are virtually no data on the histological and microbial status from the actual point of enthesis contact with the bone, where fibrocartilage is abundant, in the early stages of SpA. Knowledge of the histological features from this site is important as fibrocartilage directed autoimmunity is thought to play an important part in both human SpA and animal models of disease.9 Microbes are thought to have a major role in the pathogenesis of SpA, but the microbial status of the enthesis has not been previously reported.
A major obstacle to studying the enthesis, when compared with synovial cavities, is the difficulty in obtaining tissue from these sites. To explore the histological features and microbial status of enthesitis in early SpA, we used a sonographic based biopsy procedure to obtain tissue from clinically symptomatic entheseal sites.
PATIENTS AND METHODS
Ethical approval from the local research ethics committee was obtained before the study. Five male patients who fulfilled the European Spondyloarthropathy Study Group (ESSG) criteria for SpA10 (four HLA-B27 positive), age range (18–36 years) with disease duration ranging between one month and two years, were recruited. The duration of enthesopathy at the biopsied sites was one month, two months, three months (two cases), and one year. The diagnoses were AS (one case), undifferentiated SpA (three cases), and reactive arthritis (one case). All patients had focal tenderness over the insertion point that was biopsied, which was the plantar in four cases and the patellar tendon insertion in one case.
Imaging of enthesitis
Magnetic resonance imaging of clinically inflamed entheses was undertaken using Philips 1.5 T Gyroscanners ACS NT (Philips Medical Systems, Best, The Netherlands). Sagittal T1 weighted spin echo (SE) pulse sequences and T2 weighted turbo SE or fat suppressed (T2 FS) sequences were taken on all patients. The imaging parameters were as follows: an SE sequence with T1 weighted images (repetition time (TR) 382 ms, time to echo (TE) 14 ms, matrix 205×256, field of view (FOV) 160 mm, slice thickness 4.0 mm, slice gap 0.4 mm, number of signals averaged (NSA) 2, and acquisition time 2 min 38 s) was used. T2 SE/FS acquisition parameters were as follows: TR 3296 ms, TE 90 ms, echo train length 1/1, matrix 203×256, FOV 180 mm, slice thickness 4.0 mm, slice gap 0.4 mm, NSA 4, and acquisition time 4 min.
Enthesis biopsy
For the biopsy procedure, the inflamed insertion points were defined as previously described.11 Lignocaine (1%) was used to anaesthetise the skin and the plantar fascia and adjacent periosteum and bone. A 16 g Jamshedi needle was inserted into the enthesis. When the needle tip was 2–4 mm from the bone the stilette was withdrawn and the biopsy needle was advanced through soft tissue and into the underlying bone. Two passes of the needle were made with one going for enrichment culture and the other for histological assessment.
For microbiological analysis, a sample of enthesis tissue was placed in a dry, sterile container and transported at room temperature immediately to the laboratory. The sample was chopped into fine pieces with a sterile scalpel and placed in the aerobic blood culture bottle of the Vital continuous monitoring blood culture system (BioMérieux UK Ltd, Basingstoke, Hants). Cultures were incubated for 20 days with continuous monitoring, and terminal subculture was carried out by plating onto horse blood agar (Oxoid Ltd, Basingstoke, Hants). Again plates were incubated aerobically and anaerobically at 37°C as well as heated blood agar plates (Oxoid Ltd, Basingstoke, Hants) in 5% CO2 at 37°C for seven days. Plates were carefully inspected for the presence of colonies.
For histological analysis the samples were embedded in methyl methacrylate resin to preserve the tissue architecture. They were then cut and stained using haematoxylin and eosin for morphology assessment, and the fibrous part, fibrocartilage and adjacent bone were viewed. For immunohistochemistry analysis, antigen retrieval of sections was first performed by microwaving in 400 ml of citrate buffer pH 6.0 on high power (800 W) for six minutes as previously described.12 The following antibodies were used: CD3 (pan T cell), CD8 (T cell), CD34 (endothelial cell), and CD68 (macrophage) (all antibodies courtesy of Dr R Jones, Haematological Malignancy Diagnostic Service, Leeds General Infirmary Hospital). Sections were stained using a monoclonal antibody for VS38c (Dako, Glostrup, Denmark) using a standard three stage immunoperoxidase labelling technique using avidin-biotin immunoperoxidase complex (ABC) according to the manufacturer's instructions (Dako, Cambridgeshire, UK). 100 μl of each primary antibody was added to the slide and incubated for one hour. Slides were then washed in Tris buffered saline (TBS), and 100 μl of biotinylated secondary goat antimouse antibody was added, incubated for one hour, and then washed. The ABC/horseradish peroxidase complex was then added to the slides, incubated for 30 minutes, and then washed in TBS. Colour was developed in a 0.02% solution of 3,3`-diaminobenzidine (Sigma D-5637) and 0.15% hydrogen peroxide in Tris buffer (without saline) pH 7.6 for 10 minutes. The sections were washed in water and the staining enhanced with 0.5% copper sulphate in 0.9% sodium chloride for about five minutes, counterstained with Harris haematoxylin, dehydrated in absolute alcohol, cleared in xylene, and mounted with synthetic mounting media.
Control tissue
Normal unaffected entheseal tissue was obtained from the iliac crest at the time of elective spinal surgery bone grafting procedures. Tissue was obtained from two patients (age 60 and 36) who had no iliac crest or pelvic pain or tenderness. After removal of fragments of bone for grafting, muscle insertions were removed and placed in formalin. The samples were processed in the same way as tissue from patients with SpA. Tonsil tissue was used for positive controls. Negative controls were obtained by substituting TBS for the primary antibody on entheseal tissue sections.
RESULTS
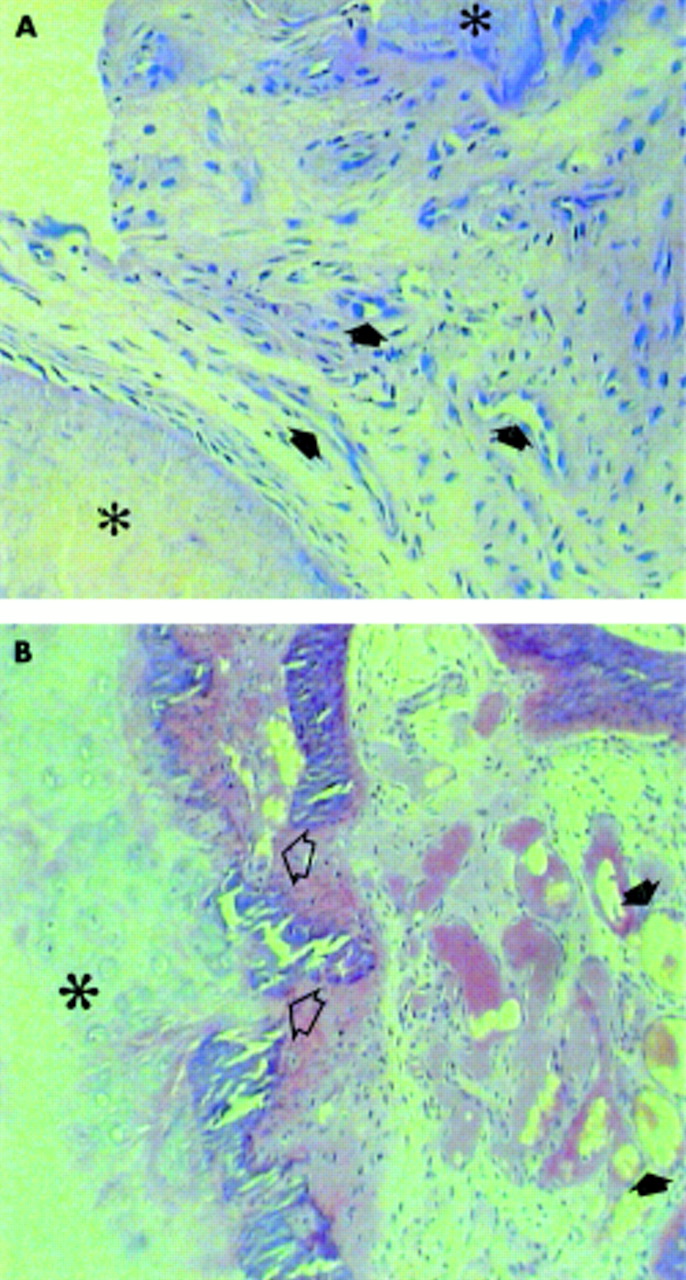
The biopsy was well tolerated and no complications were noted at one year follow up. The enrichment cultures showed no growth either by the continuous monitoring system or on the agar plates after six weeks' culture in any of the samples. Histologically, all of the biopsy specimens comprised enthesis fibrous tissue, fibrocartilage, and a small region of adjacent bone. Disruption of the normal enthesis architecture within its fibrous part was evident, with disorganisation of the normal fibrillar architecture and increased vascularity and cellular infiltration evident in all cases (fig 1A). The enthesis fibrocartilage itself was relatively intact in all cases (fig 1B). Defects between the fibrocartilage and adjacent bone, with focal loss of bone and direct contact between the fibrocartilage and the underlying bone spaces, were seen in two cases (fig 1A). The subenthesis bone was disorganised with increased vascularity and fibrous tissue proliferation in one case (fig 1B). The control tissue showed normal fibrocartilage and adjacent bone without architectural distortion or cellular infiltration.
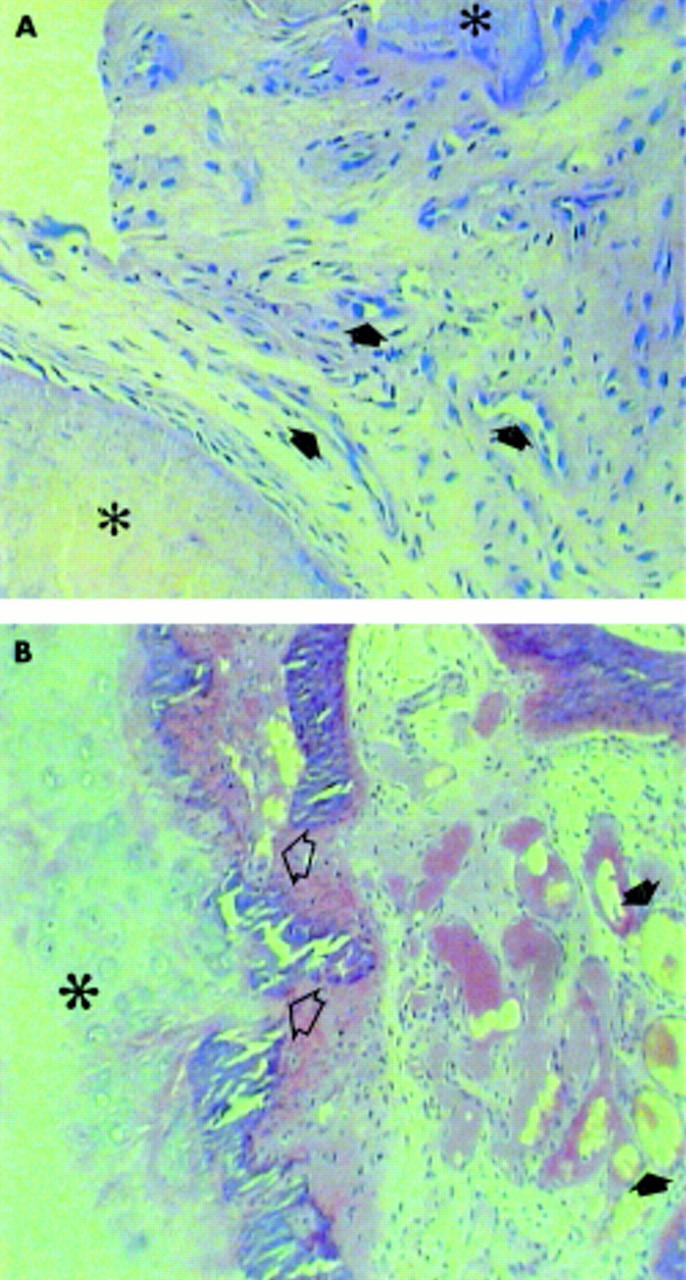
Histology of the plantar fascia employing haematoxylin and eosin (H&E) staining. (A) The sample shows an inflammatory cell infiltrate in the fibrous part of the enthesis with increased vascularity at that site (arrows). The adjacent bone is marked by asterisks. (B) In this sample the osseous part of the enthesis adjacent to the fibrocartilage is disrupted, but the fibrocartilage itself is relatively intact (asterisk). Focal bone defects at sites of fibrocartilage contact with normal bone have been reported in normal insertions (open arrows). There is an inflammatory process in the bone adjacent to the fibrocartilage with increased vascularity (arrows) and proliferation of stromal tissue.
On immunohistochemistry analysis the predominant immune cells at the enthesis were CD68 positive macrophages, which were seen in all cases (fig 2A). Macrophage infiltration was mainly at the sites of increased vascularity and cellularity shown in fig 1. One sample showed a degree of fibrocartilage infiltration by macrophages (fig 2B). Neither the fibrous part of the enthesis nor the fibrocartilaginous parts were infiltrated by lymphocytes as CD3 (fig 2C) and CD8 (fig 2D) in any of the samples. Altered vascularity in the fibrous part of the enthesis was confirmed by increased CD34 staining in all of the acute enthesitis biopsy specimens (fig 2E). The degree of bone tissue present within the biopsy specimens was not sufficient for an immunohistochemistry analysis of that site to be done. There was no inflammatory cell infiltration in the entheseal control tissue. Antibody reactivities were confirmed on the positive control tonsil tissue.

{kind=link}
{kind=link}
Immunohistochemistry using the ABC method showing the presence of macrophages in the enthesis in fibrous tissue at enthesis (open arrows) (A) and in the entheseal fibrocartilage (B) with prominent CD68 positive staining. There is no CD3 (C) or CD8 (D) positive lymphocytic infiltration at these sites. The increased vascularity within the enthesis is demonstrated by CD34 positivity (open arrows) (E).
DISCUSSION
Because of the predilection of human SpA for sites that are rich in fibrocartilage (insertional points and the sacroiliac joint), it has been suggested that AS may be caused by autoimmunity against this structure.13 There are limited histological data on the pathology at the fibrocartilage in early human SpA. The findings in this study show that the predominant infiltrating cell at the fibrocartilage in human SpA is the macrophage. As in the case of other diseased sites in SpA viable replicating microbes could not be recovered.
In studies performed in chronic AS, Bywaters reported prominent macrophage mediated fibrocartilage destruction,14 which is similar to our findings in early disease. Our biopsy specimens were small and insufficient to allow analysis of the underlying bone, but the observations of Bywaters and others have shown prominent lymphocytic infiltration within bone.7 One possible explanation for this is that autoimmunity in SpA might be primarily directed against a bone antigen.
The enthesopathy pathology in SpA responds well to anti-tumour necrosis factor α (TNFα) treatment.15 As macrophages are the principal source of TNFα, it is possible that this may underline the good response of enthesopathy to TNF blockade. The reported methodology for detecting TNFα protein in the tissues has used frozen tissue methods. We sought to preserve tissue architecture in our study so samples were fixed before histological analysis. It was not possible to optimise immunostaining for TNF in resin embedded tissue. However, frozen tissue samples are presently being obtained to determine the cytokine profiles at these sites and to employ polymerase chain reaction methodology to determine if viable microbes are present.
In conclusion the histological changes of acute enthesitis show that there is a paucity of lymphocytes at the actual insertion, and the predominant infiltrating cell type adjacent to enthesis fibrocartilage is the macrophage. Macrophages have a critical role in innate immunity and their presence at the enthesis fibrocartilage in early disease supports emerging concepts for SpA pathogenesis.16
Acknowledgments
Dr McGonagle's work is funded by the Medical Research Council of the UK. Dr Marzo-Ortega holds an Arthritis and Rheumatism Campaign (ARC) grant. Professor Emery is an ARC professor of rheumatology.