Article Text

Abstract
OBJECTIVE To compare four different inception cohorts of patients with early rheumatoid arthritis (RA) with respect to treatment strategies, disease activity, and outcome during a five year follow up period.
METHOD Data from cohorts of patients with early RA, with a standardised assessment at least every six months for five years from four different centres, were included in one database. Owing to slight differences in the individual study designs, linearly interpolated values were calculated to complete the standard follow up schedule.
RESULTS Despite similar inclusion criteria, significant differences in demographic factors and baseline disease activity were found between the different cohorts. During the follow up an aggressive treatment strategy was followed in the Dutch and Finnish cohort, an intermediate strategy in the British cohort, and a conservative strategy in the Swedish cohort. A significant improvement in disease activity was seen in all cohorts, though the most rapid and striking improvement was seen in those receiving aggressive treatment. This resulted in less radiographic destruction in the long run.
CONCLUSION This observational study of cohorts of patients with early RA confirms that early aggressive treatment results not only in a more rapid reduction of disease activity but also in less radiographic progression in the long term.
- treatment strategy
- disease activity
- outcome
- rheumatoid arthritis
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory disease with a variable and capricious course, ranging from episodes with a mild non-destructive polyarthritis, alternated by spontaneous remissions, to a rapidly progressive disabling arthritis, sometimes with widespread systemic features. Although many treatments have been used in the management of RA, pharmacotherapy is still the most important component. Many randomised controlled trials have shown that disease modifying anti-rheumatic drugs (DMARDs) do influence the disease process and retard the radiological destruction, at least in the short term (up to three years).1-11 However, an important drawback in applying DMARDs is the high incidence of patients discontinuing treatment because of a lack of efficacy or the occurrence of adverse reactions. Several studies have shown that DMARDs, at best, are used for a median time of five years.12 ,13 However, as a patient with RA often has to be treated with DMARDs for a period of 20–30 years, different pharmacotherapeutic strategies have been proposed.
The first strategy proposed was the pyramid approach, in which the least toxic DMARD, which often seemed to be also the least effective DMARD, was given after a long period of treatment with non-steroidal anti-inflammatory drugs alone. In the past decade, it has been proposed to start with DMARDs promptly after a diagnosis of RA has been made, aiming at suppressing the disease activity as much as possible.4 ,14-20 This strategy has been given several names, such as pyramid upside down, step down strategy, “sawtooth” strategy, or bull’s-eye strategy. It goes without saying that evaluation of treatment strategies is far more difficult than (short term) clinical trials comparing single or combination DMARD treatment.
To date, reports on comparison of treatment strategies are scarce. In a short term open randomised controlled trial van der Heideet al concluded that suppression of disease activity was much better after immediate introduction of DMARD treatment.16 However, this effect was not reflected in the radiological progression scores. Möttönen et al prospectively studied Finnish patients with early RA and compared their findings with those of a previously described cohort (two year follow up).5 They concluded that in the conservatively treated cohort, disease activity remained higher and radiographic progression was higher than in the aggressively treated cohort. Furthermore, based on the data of the Finnish patients only, they concluded that aggressive treatment was beneficial for at least six years. Stenger et al designed a prospective two year follow up study with an experimental group and a historical control group in order to compare the effects of aggressive and conservative treatment.21 In that study it was concluded that radiographic progression was significantly less after aggressive treatment.
In our study, for the first time, the data of four inception cohorts with early onset RA from four different European countries with divergent pharmacotherapeutic strategies—namely, Finland (F), Sweden (S), the United Kingdom (UK), and the Netherlands (N), are directly compared. Our study aimed at assessing (a) the treatment strategies that were used and to investigate the effect of these treatment strategies on (b) disease activity and (c) outcome.
Patients and methods
POPULATION AND DESIGN
The study group comprised four European inception cohorts with early onset RA from Finland (n=81), Sweden (n=102), the United Kingdom (n=112), and the Netherlands (n=174). All patients fulfilled (for the first years retrospectively) the 1987 ARA (American Rheumatism Association; now the American College of Rheumatology) classification criteria.22 Early onset was defined as disease duration of less than one year. Additionally, patients should not have been treated before with DMARDs or corticosteroids. For the Finnish patients, inclusion was restricted to patients up to 65 years of age. For all cohorts, exclusion only occurred owing to serious comorbidity.
The patients of the four cohorts were included between 1985 and 1991. The disease-specific characteristics were assessed at baseline and, subsequently, every six months over a period of five years. Data on these characteristics covered 70–95% of the follow up period.x Rays were taken annually. The following radiographic scores were available: Finland 81, Sweden 87, United Kingdom 79, the Netherlands 84, but for the Swedish, the British, and the Dutch cohort, x rays were available only for the first group of included patients and for the British cohort, also, radiographic follow up was limited to two years. With these restrictions, radiographic data covered approximately 80% of the follow up period. The loss to follow up owing to death amounted for the Dutch cohort to 10 (6%) patients, for the Finnish cohort to three (4%) patients, and for the Swedish cohort to six (6%) patients. For the British cohort these figures were not available.
ASSESSMENTS
Several disease-specific characteristics were assessed. Morning stiffness was given in minutes. Joint swelling was measured as a 44 joint score (F, N) or as a 50 joint score (S, UK). The erythrocyte sedimentation rate (ESR) was measured according to the Westergren method (mm/1st h). Tender joints were assessed by the Ritchie Articular Index (RAI).23 Pain was further assessed by the patients on a (10 cm) visual analogue scale (VAS). The disease activity score (DAS)24 was computed from the RAI, the number of swollen joints, and the ESR. Rheumatoid factor was determined by nephelometry (F, positive if ⩾20 IU/ml; N, positive if >10 IU/ml), by the enzyme linked immunosorbent assay (ELISA) method (S, positive if >20 IE), or by the semi-automated latex method (UK, positive if >60 IE). As the four individual study designs were slightly different, linearly interpolated values were calculated (approximately 15%) to complete the standard follow up schedule.
Outcome was measured by following radiographic progression (hands and feet). In Finland, Sweden, and the United Kingdom, radiographic scores were obtained by the Larsen method with a range of 0–200.25 In the Netherlands, radiographs were scored according to the modified Sharp method1 and therefore not included in the analysis. British radiographic scores (n=79) were only available for the first two years, and therefore analysis included both a short follow up period (that is, the first two years) and a long follow up period (that is, five years).
TREATMENT STRATEGIES
Type of DMARD and reason for discontinuation were recorded in all countries. In Finland and in the Netherlands specific start and end dates were available, whereas in the United Kingdom information on DMARD use was linked with scheduled follow up visits. Treatment strategies were compared with respect to:
The efficacy of the DMARD(s) used: - Low: chloroquine, oral gold, or a combination of these - Moderate: azathioprine, d-penicillamine, intramuscular gold, or a combination of these - High: methotrexate, sulfasalazine, or a combination of these
The lag time - That is, the time between inclusion in the study and prescription of the first DMARD
The cumulative time of DMARD use - That is, duration of DMARD use in the five year follow up period.
The average doses used for the different DMARDs were as follows: chloroquine 250 mg daily, hydroxychloroquine 200–400 mg daily, auranofin 6 mg daily, azathioprine 100 mg daily,d-penicillamine 500–750 mg daily, parenteral gold 50 mg weekly, methotrexate 7.5–15 mg weekly, and sulfasalazine 2000–3000 mg daily.
STATISTICS
For each cohort, median values of the disease-specific characteristics were calculated at baseline and during follow up. (Back)-transformation techniques were applied to obtain confidence intervals. Differences in demographics and in baseline values of disease-specific characteristics were evaluated (p<0.05) by the χ2 test, Wilcoxon two sample test, analysis of variance, or Student's t test. Bonferroni correction was applied (p<0.05/6 or p<0.05/3). The course of the disease activity during the first year was characterised by the “curvature”, as a positive curvature indicates a rapid reduction, a negative curvature is associated with a slow reduction, and a zero curvature means a steady or (linear) development, according to the following formula: curvature = (value at 12 months − value at 6 months) − (value at 6 months− value at baseline)
These curvatures were used within each cohort (Wilcoxon signed rank statistic; p<0.05) to determine whether or not there was a rapid reduction in disease activity, and between the cohorts (Kruskal-Wallis test; p<0.05) to compare the extent of reduction of disease activity. Differences between two cohorts were further evaluated using Bonferroni corrected p levels.
Radiographic scores (Larsen) were square root transformed and analysed by individual linear regression with duration. The slope of the regression line was taken as the progression rate of the patient. Analysis included both a short follow up period (the first two years) and a long follow up period (all five years). Again, differences between cohorts were tested by the Kruskal-Wallis test (p<0.05) and further evaluated using Bonferroni corrected p levels.
Results
BASELINE DESCRIPTION OF THE FOUR COHORTS OF PATIENTS WITH EARLY RA
Table 1 presents baseline values of demographic variables and disease-specific characteristics. Between the four cohorts, several significant differences were seen. At inclusion, the Finnish patients were younger and more often female. Both in the Finnish and in the British cohort fewer patients were rheumatoid factor positive. The longest duration of morning stiffness was reported by the Finnish patients. The Swedish patients had the lowest number of painful joints (RAI), whereas patients' reported pain (VAS) was higher for both Swedish and Dutch patients. Dutch and British patients had the highest number of swollen joints. Thus the DAS (swollen joint count, RAI, and ESR) was also significantly higher for the British and the Dutch patients. At baseline, radiographic damage of the Finnish patients was significantly less than that of the Swedish and British patients.
Baseline demographics and disease-specific characteristics (significant differences1-150 are bold)
TREATMENT STRATEGIES
Corticosteroid use
The percentages of patients using corticosteroids (dose 5–10 mg daily) were comparably low in the British, Finnish, and Dutch cohorts (2.7%, 3.7%, and 7.5%, respectively) and somewhat higher in the Swedish cohort (15.7%). After five years these figures were 22.3%, 32.5%, 31.6%, and 30%, respectively.
Efficacy of the DMARDs used
By comparing DMARD use during the follow up period (table 2), it can be seen that in Finland, the United Kingdom, and the Netherlands most of the time moderately to highly effective DMARDs were given, whereas in Sweden mostly mild to moderate DMARDs were prescribed.
Disease modifying antirheumatic drug (DMARD) use
Lag time
The time between inclusion and the prescription of the first DMARD, called the lag time, was calculated. The median lag time (and interquartile range) was for Finland, Sweden, the United Kingdom, and the Netherlands respectively zero months (0–0), three months (0–14), three months (0–36), and zero months (0–0.2).
The cumulative time of DMARD use
In the five year follow up period all Finnish patients were treated with DMARDs. For the Netherlands, Sweden, and the United Kingdom, the percentages of patients not treated with DMARDs were 6%, 33%, and 35% respectively. It appeared that Finnish and Dutch patients were treated with DMARDs for 78% and 67% of their follow up period respectively, whereas the Swedish and the British patients received DMARDs for approximately 40% of their follow up period.
From a consideration of the efficacy of the given DMARD(s), the lag time, and the cumulative time of DMARD use, we concluded (table 3) that in the Finnish cohort and in the Dutch cohort an aggressive treatment strategy was followed, whereas in the British cohort an intermediate treatment strategy and in the Swedish cohort a conservative treatment strategy was followed.
Classification of treatment strategies
DISEASE ACTIVITY
Figure 1 presents the course of the disease activity over the five year follow up period (median values and 95% confidence intervals). As the four cohorts had significant differences in baseline (median) values, curvatures were used to evaluate change in disease activity. In all four cohorts the main reduction of disease activity was seen in the first year.

The course of the disease during the five year follow up period (median values and 95% confidence intervals). ESR = erythrocyte sedimentation rate; VAS = visual analogue scale; RAI = Ritchie Articular Index; DAS = disease activity score.
In both the Finnish and the Dutch cohorts it seemed that during the first year of the disease all the disease-specific characteristics showed a significant (p<0.01) rapid reduction of disease activity at six months—that is, early in the course of the disease. For the British cohort, only morning stiffness was rapidly reduced (p<0.01).
Additionally, significantly more (Bonferroni corrected; p<0.0083) reduction of morning stiffness occurred in the Finnish cohort than in the Swedish cohort. The reduction of disease activity, measured by the swollen joint score, the ESR, or the DAS was greater (Bonferroni corrected; p<0.0083) for both the Finnish and the Dutch cohorts than for the Swedish cohort. No difference was found for variables related to pain (namely, RAI and VAS).
OUTCOME AFTER FIVE YEAR FOLLOW UP
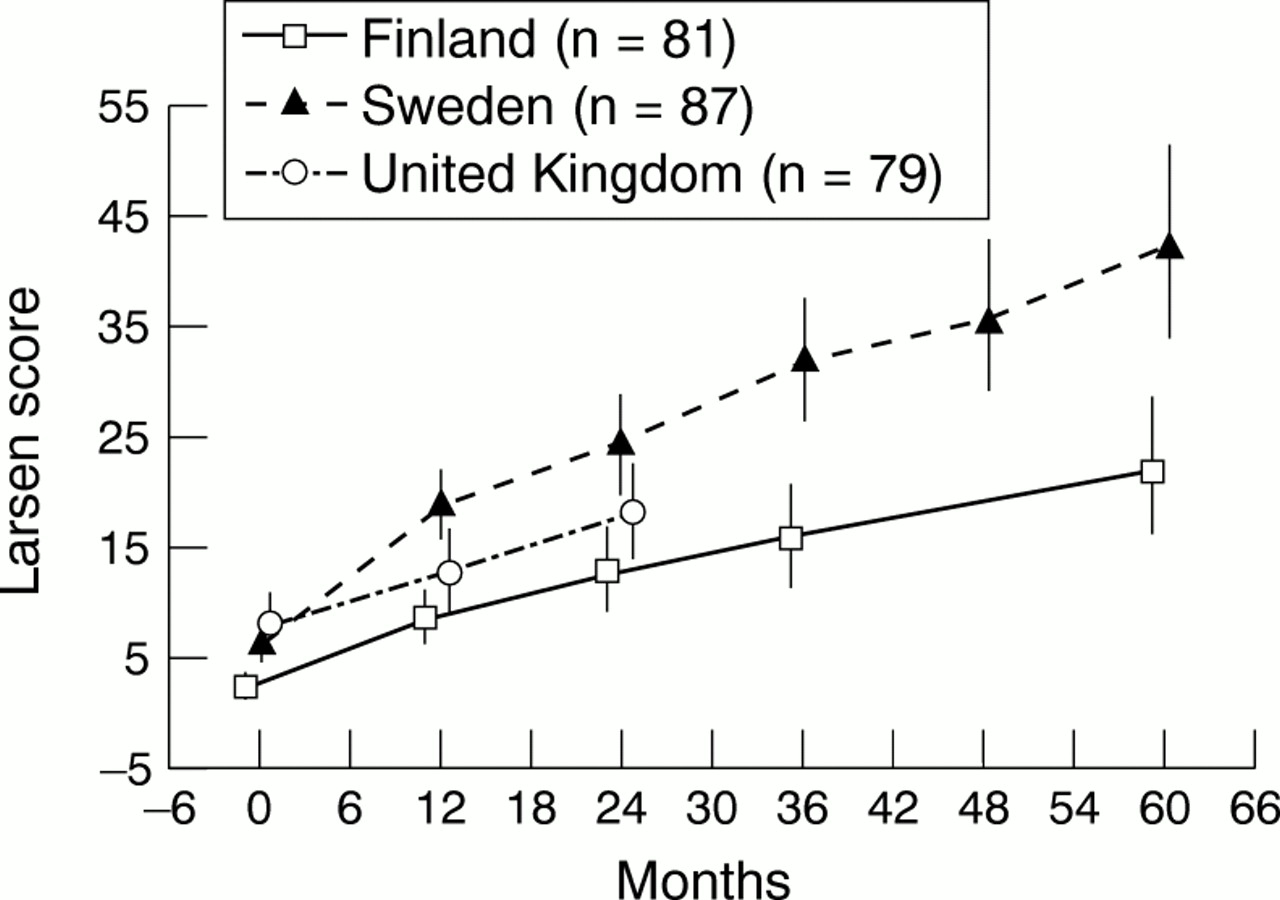
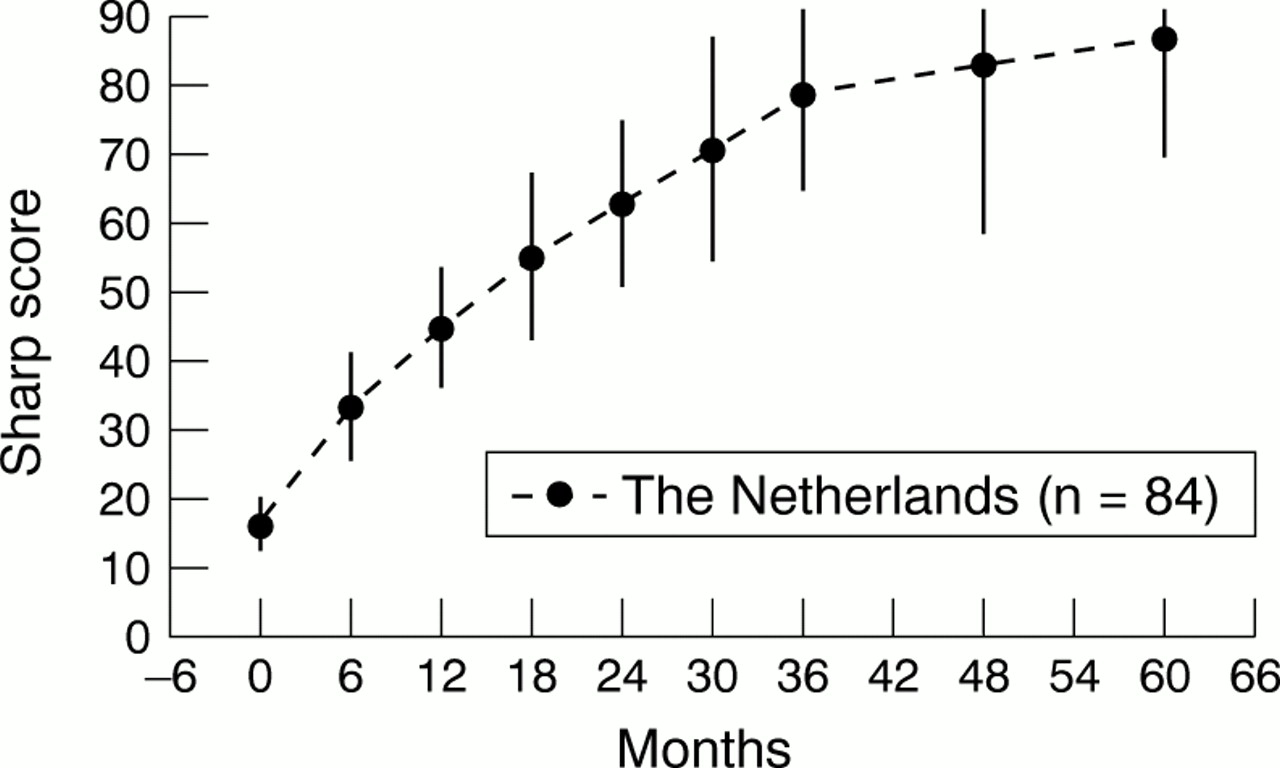
Figure 2 presents the (Larsen) radiographic scores (median and 95% confidence intervals) over the five (or two) year follow up period. Comparison of baseline values (table 1) showed that already at baseline radiographic damage was less in the Finnish cohort than in the other cohorts. Linear regression analysis over the two year follow up showed that the Finnish cohort, compared with the British and Swedish cohorts again showed less radiographic progression, though significance was not reached in either case (p<0.08, p<0.06, respectively). The British cohort had (Bonferroni corrected; p=0.0003) less progression than the Swedish cohort. Over the five year follow up the Finnish cohort had less radiographic progression than the Swedish cohort (Bonferroni corrected; p=0.0034). Because for the Finnish patients, inclusion was restricted to patients aged up to 65, a subanalysis (Bonferroni corrected) with this age criterion was carried out; results were similar. Dutch radiographic (Sharp) scores were not taken into the analysis, but fig 3 presents median scores. As with the Finnish cohort, progression appeared to slow down.

Median radiographic (Larsen) scores (95% confidence intervals).

{kind=link}
{kind=link}
{kind=link}
Dutch median radiographic (Sharp) scores (95% confidence intervals).
Discussion
It is generally accepted that DMARD treatment in patients with RA is effective, at least in the short term. Many controlled clinical trials have not only demonstrated the effects of these treatments on the disease process but also on outcome variables like functional capacity and radiographic damage. However, in the long term these effects are questionable owing to the high incidence of drop out and the toxicity and/or lack of efficacy of the drugs. Over the years, different treatment strategies have been used; in the past decade early, aggressive treatment was emphasised. However, the effectiveness of these different strategies has only been scantily evaluated until now. This is probably because of the need for a study design with large cohorts of prospectively included patients with early RA with known divergent pharmacotherapeutic strategies. In this study we compared the course of the disease during the first five years of the disease in four inception cohorts from different European countries.
When the four cohorts were compared, three main treatment strategies could be distinguished. The aggressive treatment strategy—that is, early intensive treatment with moderately to highly effective DMARDs, was applied to the Finnish and the Dutch patients. The British patients received an intermediate treatment strategy, based on a slow start, followed by extensive use of effective DMARDs. In this cohort, the duration of DMARD use had to be derived from information collected only at the scheduled follow up visits, and therefore underestimation can be expected. Swedish patients received the more conservative strategy, based on slow and extensive treatment with low to moderately effective DMARDs.
For all cohorts the inclusion and exclusion criteria were similar and RA diagnosis was based on the ARA (1987) criteria. However, despite this, the disease-specific characteristics (core set variables) showed large differences in baseline values of morning stiffness, joint counts, and pain. This may be due to a variety of circumstances, such as different genetic, cultural or ethnic features, different referral policies or measurement differences (as variables for disease activity are not internationally calibrated). In the analysis, specific procedures had to be chosen (curvatures) because absolute values could not be directly compared.
Early treatment with moderately to highly effective DMARDs produced a rapid and sharp reduction of disease activity in the first year of the disease. Thereafter, the level of disease activity remained rather constant. Radiographic damage (Larsen) at baseline was least in the Finnish cohort. This difference was further maintained if only the patients (F, S, and UK) under the age of 65 were included in the analysis. Owing to the difference in baseline radiographic damage, progression was evaluated by linear regression. Radiographic progression (irrespective of baseline values) was highest for the Swedish cohort, intermediate for the British cohort, and lowest for the Finnish cohort. In the Dutch cohort radiographic progression slowed down. These results show clearly that early and continuous treatment with effective DMARDs results in a more rapid reduction of the disease activity, and even in less radiographic damage after five years, than delayed treatment. This is in concordance with short term randomised clinical studies4 ,17 ,19 ,26 ,27 showing that early and continuous treatment results in a better outcome.
Despite these beneficial effects of aggressive treatment, one should be cautious as to whether such a strategy does not result in increased morbidity and/or mortality. In this study, no figures on morbidity are available, but over the first five years, the number of deaths was similar for the four cohorts. Recently, mortality figures from both the Swedish and Dutch inception cohorts were published,28 ,29showing that in the first 10 years the mortality rate of the RA cohort was not different from that of the general population. Fortunately, it can be concluded that aggressive treatment does not seem to increase the mortality rate. However, aggressive treatment needs preferably to be reserved for patients with aggressive disease. Therefore, treatment goals need to be defined individually and DMARD treatment tailored accordingly. To achieve this, further research should focus on stratifying patients by genotype and other prognostic markers.30-36 It can be foreseen that such research, again, requires a collective effort as large international datasets are needed to establish (clusters of) prognostic factors that are sufficiently accurate in the clinical setting.
Conclusion
This observational study of cohorts of patients with early RA from four different European countries confirms that early treatment reduces disease activity more rapidly. In those cohorts in which patients were treated more aggressively, more suppression of disease activity was achieved than in the more conservatively treated cohorts. Last but not least, radiographic progression, irrespective of baseline damage, was less in those cohorts in which patients were treated more aggressively.
Acknowledgments
We are grateful to all the patients who willingly gave of their time to complete the various assessments.
References
Footnotes
This study was supported by a grant from Novartis AG.