Article Text

Abstract
Background COBRA (for ‘COmbinatie therapie Bij Rheumatoide Artritis’) combination therapy is effective for the treatment of rheumatoid arthritis (RA), but long-term safety is unknown. This study evaluates survival, comorbidities and joint damage in the original COBRA trial cohort.
Methods In the COBRA trial, 155 patients with early RA were treated with sulfasalazine (SSZ) monotherapy (SSZ group) or a combination of step-down prednisolone, methotrexate (MTX) and SSZ (COBRA group). The current 11-year follow-up study of the COBRA trial invited all original patients and performed protocollised scrutiny of clinical records, questionnaires, physical examination, laboratory and imaging tests.
Results In all, 152 out of 155 patients yielded at least partial data. After a mean of 11 years follow-up, 18 (12%) patients had died, 6 COBRA patients and 12 SSZ patients, HR 0.57 (95% CI 0.21 to 1.52). Treatment for hypertension was significantly more prevalent in the COBRA group (p=0.02) with similar trends for diabetes and cataract. Conversely, hypercholesterolaemia, cancer and infection showed a trend in favour of COBRA. Other comorbidities such as cardiovascular disease and fractures appeared in similar frequency. Radiographic findings suggest as a minimum sustained benefit for COBRA therapy, that is, difference in joint damage but similar subsequent progression rates after 5 years. Imputation to compensate for selective dropout suggests increasing benefit for COBRA, that is, difference in yearly progression rates similar to that seen in the first 5 years of follow-up.
Conclusions After 11 years, initial COBRA combination therapy resulted in numerically lower mortality and similar prevalence of comorbidity compared with initial SSZ monotherapy. In addition, lower progression of joint damage suggests long-term disease modification.
Statistics from Altmetric.com
Introduction
The COBRA (for ‘COmbinatie therapie Bij Rheumatoide Artritis’) study was a double blind randomised controlled trial in patients with early rheumatoid arthritis (RA) that compared the combination of three traditional disease-modifying antirheumatic drugs (DMARDs) (sulfasalazine (SSZ), methotrexate (MTX) and prednisolone) with monotherapy (SSZ). It proved COBRA therapy to be a rapidly effective treatment of RA,1 including a sustained decrease of radiological progression after a mean of 4.5 years follow-up.2 A subsequent trial showed COBRA therapy to be as effective as initial combination therapy of high-dose MTX with infliximab.3 4 Despite this, we showed that Dutch rheumatologists are reluctant to use COBRA in their clinical practice,5 mainly due to practical and emotional constraints as well as concerns over long-term safety of high dose prednisolone.6 Worldwide, the use of prednisolone in RA is still a topic for debate.7
In the context of an effort to improve uptake of COBRA in general rheumatology practice, we conducted a study on the long-term safety of this regimen by studying survival and comorbidity in the original COBRA trial cohort. In addition we studied whether the benefit on radiographic progression present at 5 years was sustained over a longer period.
Methods
The COBRA cohort
From 1993 to 1995, 155 patients with early RA entered a randomised, double blind trial comparing COBRA combination therapy to SSZ monotherapy. Details of the initial trial and of the 5-year follow-up have been reported previously; key demographics are summarised in table 1.1 2 In summary, inclusion criteria were a diagnosis of RA (American College of Rheumatology (ACR) criteria) with a duration of 2 years or less; ≥6 swollen joints and presence of at least 2 of the following: ≥9 tender joints; morning stiffness ≥45 min; erythrocyte sedimentation rate (ESR) ≥28 mm/h. Patients previously or currently treated with any DMARD except antimalarials were excluded.
Baseline patient characteristics at 0 and 11 years after the COBRA trial
COBRA step-down combination therapy comprises SSZ (2 g/day), MTX (7.5 mg/week) and an oral pulse of prednisolone, starting with 60 mg in the first week and tapered to 7.5 mg in the seventh week. At 28 weeks, prednisolone is tapered and withdrawn and after 40 weeks, MTX is withdrawn. Patients in the SSZ group received SSZ (2 g/day) and placebo MTX and prednisolone. All patients received folic acid (1 mg/day), calcium (500 mg/day) and if needed 25-hydroxyvitamin D (400 IU/day). Patients experiencing a disease flare during or after tapering of a drug restarted treatment with the drug that was most recently withdrawn. After the protocol period of 56 weeks, treatment decisions were made at the discretion of the treating rheumatologists.
All patients were invited for follow-up by their current rheumatologist. The general practitioner was asked to invite patients without a rheumatologist to participate at the nearest hospital. Assessments and data collection were blind to the original treatment allocation. All participating patients gave their written informed consent; this study was approved by the medical ethical committee of the VU University Medical Center.
Outcome measurements
Disease activity and patient reported health outcomes
Trained research nurses performed the joint counts to calculate the 28-joint Disease Activity Score (DAS28), with remission at DAS28<2.6.8 Visual analogue scales measured pain and fatigue, and the Health Assessment Questionnaire (HAQ),9 36-item Short Form questionnaire (SF-36)10 and EuroQol11 measured functional ability and health status, respectively.
Laboratory measurements
These included ESR, C reactive protein (CRP) and cholesterol (total, low-density lipoprotein (LDL) and high-density lipoprotein (HDL)).
Survival and comorbidities
Clinical records (and the general practitioner where necessary) were queried for survival, including information on date and underlining cause of death. A protocollised scrutiny identified major comorbidities. For a list, see supplementary appendix 1. Dual-energy x-ray absorptiometry (DEXA) measured changes in bone mineral density (BMD) in the anteroposterior lumbar spine at L2–L4 and the femoral neck. Two readers (WL, BD) unaware of the trial allocation graded radiographs of the thoracic and lumbar spine for vertebral deformities (Th4–L5, Genant criteria).12
Radiographs
As follow-up of radiographs of hand and feet was complete for up to 5 years, the current study collected all available subsequent radiographs, including one made for this study. Two independent assessors scored digitally converted images of 2, 5, 8 and 11 years of follow-up according to the Sharp/van der Heijde method.13 14 Assessors were blinded for group allocation but aware of time sequence; improved scoring was allowed. Their agreement on the change between 5 and 11 years (intraclass correlation coefficient) was 0.82. Missing data were linearly interpolated between available assessments. Results are reported as the mean of the two observers' scores. To compensate for differential dropout, an extra dataset was made that replaced missing values up to 11 years by values imputed from individual progression rates of patients between 0 and 5 years follow-up.
Drug use
Drug treatment was documented from 56 weeks (end of trial), facilitated by the presence of earlier follow-up data. The use of DMARDs and biologicals was registered as yes/no; use of oral prednisolone was calculated as mean and cumulative dose following a protocol (see supplementary appendix 2). Patients completed a questionnaire on lifestyle, comorbidities and drug use, with special focus on prednisolone and biologicals.
Statistical analysis
Student t tests and continuity-corrected Pearson χ2 tests analysed differences between treatment groups where appropriate, without correction for multiple tests. Cox regression analysed survival; data were censored 1 April 2006. Survival was also compared to a reference sample of the general population of The Netherlands, matched for age and sex.15 Generalised estimating equations (GEE) analysis with an exchangeable correlation structure was applied to analyse progression of joint damage on radiographs in years 5, 8 and 11. Significance was reached at p<0.05. All statistical analyses were conducted using SPSS for Windows, V.15.0 (SPSS, Chicago, Illinois, USA). Patients who died during the follow-up period contributed data up to the moment of death.
Results
The original COBRA trial included 155 patients; 76 received COBRA therapy and 79 SSZ only.
For survival, follow-up is almost complete with only 3 of 155 patients completely untraceable. The reasons for 20 patients to refrain from full participation comprised: health problems (n=3), not seeing a rheumatologist anymore and unwilling to participate (n=5), a centre not participating (n=5) and unspecified (n=7). In some of these 20 patients data could still be gathered from available material. Radiographs at 11 years were available for 112 patients and 2 or more radiographs were available for 146 patients. Follow-up of comorbidities and drug use in clinical records is complete for 146 out of 155 patients, with 2 patients missing in the COBRA group and 7 in the SSZ group. Vertebral fractures could be studied for 50 COBRA patients and 43 SSZ patients and DEXA was measured in 47 patients in both treatment groups.
Apart from the three untraceable patients, we were unable to follow-up on any outcome other than death of a further six patients (three COBRA, three SSZ). Of nine patients, only comorbidities were documented, but no new data could be gathered (two COBRA, seven SSZ).
General health characteristics
The mean age of patients at follow-up was 60 years, with more women in the COBRA group (68% vs SSZ 52%; table 1). Functional capacity and disease activity between the groups was similar: mean (SD) HAQ score 1.02 (0.69) vs 0.91 (0.65), DAS28 3.05 (1.2) vs 3.07 (1.3) with 39% of patients in remission in both groups. The patients lost to follow-up at 11 years (25 SSZ patients and 16 COBRA patients) had a significantly higher HAQ at 5 years follow-up. Utility scores (EQ-5D) were similar: 0.72 (0.2) vs 0.74 (0.2). Scores on the SF-36 were also similar, and all subdomains except mental health were well below population norms in the two groups (data not shown).
Survival
After a mean of 11 years follow-up, only 6 patients had died in the COBRA group compared to 12 in the SSZ group. Adjusted for age, the hazard ratio for COBRA compared to SSZ was 0.57 (95% CI 0.21 to 1.52, p=0.26). Additional adjustment for sex yielded similar results (figure 1).

The 11-year survival after the COBRA (for ‘COmbinatie therapie Bij Rheumatoide Artritis’) trial. Sulfasalazine (SSZ) (lower line) in dark grey, healthy Dutch control population (middle line) in light grey, COBRA (upper line) in black.
Causes of death in the COBRA group were as follows: two from cancer (adenocarcinoma, lung), one mesenteric thrombosis, one pulmonary fibrosis and two from unknown causes. Causes of death in the SSZ group were as follows: six from cancer (lung, colon, pancreas, acute myeloid leukaemia, ovary, adenocarcinoma), two from cardiovascular disease (myocardial infarction, circulatory failure after hip surgery), one from obstructive pulmonary disease and three from unknown causes.
Comorbidity
Major comorbidity was similar in both groups. Specifically, cardiovascular events did not occur more commonly in the COBRA group (table 2). However, hypertension was significantly more prevalent in the COBRA group, and there were similar trends for diabetes and cataracts. In contrast, hypercholesterolaemia, cancer and infection showed a trend in favour of COBRA.
Comorbidities in 11 years of follow-up
Prevalence of osteoporosis was also similar in both groups: clinical fractures, radiographic vertebral fractures and bone loss were all similar. Prevalent vertebral deformities (mostly thoracic) were found in 11 of 50 (22%) patients in the COBRA group versus 9 of 43 patients (21%) in the SSZ group. Mean bone loss at the spine and femoral neck since inclusion was −5.2 (14.3) and −11.1% (13.9) in the COBRA group and −4.1 (12.0) and −11.8% (12.4) in the SSZ group. Osteoporosis based on the DEXA measurement at 11 years (T score <−2.5 in spine or hip) was seen in five COBRA patients and nine SSZ patients.
Drug treatment
After the trial period COBRA patients tended to be on prednisolone more frequently and use it for longer periods which resulted in a somewhat higher mean cumulative dose (see supplementary appendix 2); none of these differences were significant. Likewise, the proportion of patients treated with MTX or biologicals was slightly (but not significantly) higher in the COBRA group.
Radiography
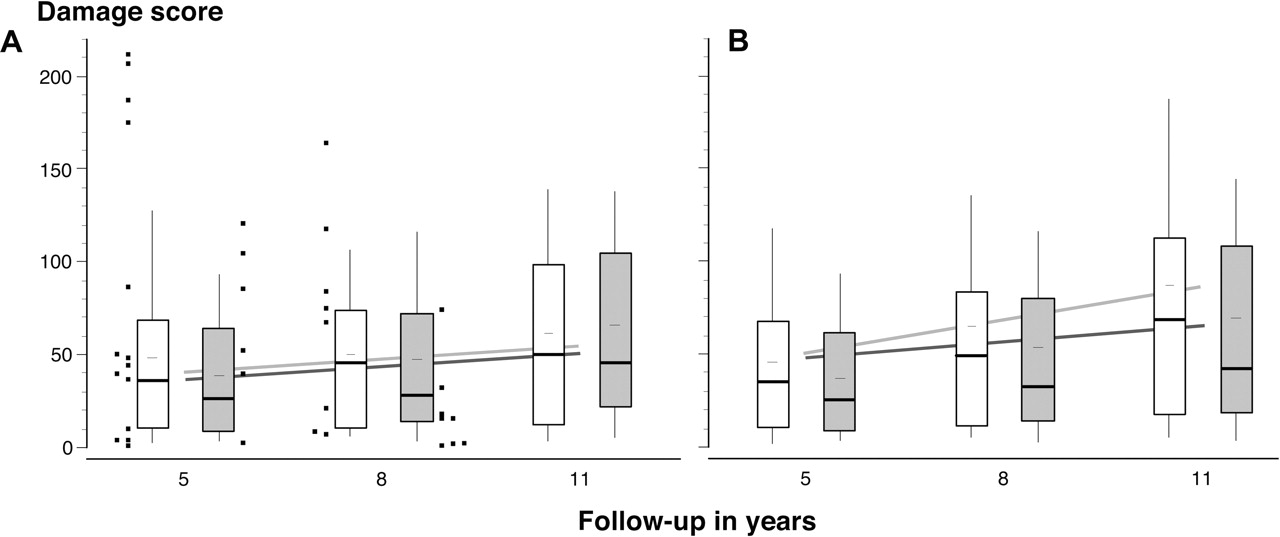
In the patients available for study, on initial examination damage progression appears similar, with median damage in the COBRA group even slightly higher than the SSZ group at 11 years (figure 2A). GEE analysis suggests scores in both groups increase by 2.4 points per year with the COBRA group 4.2 points lower than the SSZ group at every time point. However, the interpretation of the results is hampered by differential dropout: more patients in the SSZ group dropped out (12 died, 15 lost to follow-up) and these patients had more damage at their last available measurement (51, median 25) than the COBRA patients that dropped out (6 died, 11 lost to follow-up; score mean 23, median 8). This is seen by the distribution of the last available scores in figure 2B. When data of the patients that were lost to follow-up are imputed up to 11 years according to their individual progression rate in the first follow-up period (1–5 years2), the GEE model shows a significant difference between the treatment groups of 3.1 points per year in favour of the COBRA group, consistent with the results in the first 5 years (p=0.03).
{kind=link}
{kind=link}
A. Total Sharp–van der Heijde radiographic damage scores after the COBRA (for ‘COmbinatie therapie Bij Rheumatoide Artritis’) trial. Boxes show inner quartiles, medians as thick bars, means as thin bars and 10% to 90% percentiles as whiskers; sulfasalazine (SSZ) in white, COBRA in grey. Last available score of patients lost to follow-up (dots) show patients dropping out of the SSZ group have higher damage scores before dropping out. The lines represent the generalised estimating equations (GEE) model that most closely matches the available data (SSZ light, COBRA dark grey). B. Total damage scores (box plots) with imputation of missing data at 8 and 11 years based on individual progression rates recorded between 0 and 5 years (SSZ in white, COBRA in grey). The lines represent the GEE model that best matches this data (COBRA in dark grey, SSZ in light grey).
Discussion
This 11-year follow-up study strongly suggests that brief and intensive combination therapy that includes an oral pulse of glucocorticoids has a risk profile similar to that of other antirheumatic strategies. Especially glucocorticoids administered in this fashion do not appear to carry an unacceptable risk of long-term consequences. In fact, in the COBRA group actual mortality was lower, and cardiovascular and other major comorbidities similar to that in the SSZ group. Increases in the prevalence of hypertension and diabetes were offset by a decrease in hypercholesterolaemia. Prevalence of osteoporosis was also highly comparable. Many commonly reported side effects of prednisolone16 were not seen at all in our study. Moreover, after 10 years of therapy at the discretion of the treating doctor, benefits on the disease itself, as previously demonstrated in damage progression after 5 years2 appeared to be maintained and perhaps even continued to increase after COBRA therapy, depending on how one deals with the selective drop-out cases. Recently Verschueren and colleagues demonstrated the feasibility of COBRA therapy in daily practice.17 Given these and former published data,1 2 5 18,–,20 we feel COBRA therapy is effective, cost effective, feasible and safe to use as treatment in early RA.
A strength of this study is the high percentage of patients with at least partial follow-up. In particular the survival analysis, with only three patients declared missing, was very complete, giving a reliable result of mortality in our cohort. The 40% to 50% reduction in mortality risk of COBRA is remarkable, especially considering the relatively low overall mortality in our study. Although our sample size was too small to exclude a chance finding, the converse (an increased mortality due to COBRA) has become exceedingly unlikely. Kroot et al studied mortality in an inception cohort of patients with recently diagnosed RA followed-up for 10 years. They found a mortality of 16% in their inception cohort, compared to 11% in our cohort of trial patients; as our patients had active disease, we would expect them to have an increased mortality risk.21 Like us, Kroot et al found no increased mortality in patients with RA compared to the general Dutch population, in contradiction to most studies indicating an increased mortality risk.22,–,24
For comorbidity, the only significant difference between the two treatment groups was the increased prevalence of treated hypertension in the COBRA group. The prevalence of hypertension and other comorbidities was identified by chart review and use of medication during the follow-up period. Clearly, this method has its limitations, such as underreporting or selective over-reporting in patients treated with the COBRA regimen (expectation bias). For instance COBRA patients could have been more frequently checked for hypertension because they received a high dose of prednisolone in the past, as compared to the SSZ patients.
Another potential point of concern is the bone density data. Bone scanning apparatus may have changed over the years, affecting reliability of the change scores. However, this should not bias the comparisons between groups, as this would be a centre effect and patients were stratified for centre on randomisation.
The findings on cardiovascular morbidity are highly interesting. The lower mortality and similar rates of cardiovascular disease, despite some indication of increased hypertension and diabetes mellitus in the COBRA group, suggests that this COBRA regimen including an oral pulse of prednisolone has no additional long-term side effects in the setting of chronic antirheumatic therapy that includes low-dose glucocorticoid therapy in patients with more severe forms of RA.
Confounding by indication is a well known problem in observational studies that have found increased cardiovascular risk in patients with RA treated with glucocorticoids. In these studies, glucocorticoid use is often a marker for severe disease with its concurrent comorbidity.25 In our study, glucocorticoid use in the follow-up period tended to be higher in the COBRA group (52%), although the SSZ group also received prednisolone during follow-up (37%). Of note, these percentages are still lower than the 66% ‘ever users’ reported by Caplan et al in the US.7 The use of prednisolone during follow-up in both treatment groups makes it impossible to judge which side effects are glucocorticoid induced and which are not. Obviously a larger sample size and a longer follow-up period would make these conclusions more robust. However, for side effects and comorbidity that occur frequently the numerical survival benefit combined with the lack of further important differences in comorbidity between the groups is highly reassuring.
The main objective of this study was safety, given the persistent concern in the rheumatology community over the long-term safety of the COBRA regimen. However, we could not resist the temptation to also look at the radiographs and found the proper analysis of such data to be complex.
The analysis of radiographic progression has limitations inherent in a long-term follow-up study. Patients with the poorest prognosis (and highest progression rates) preferentially dropped out of the SSZ group, artificially improving the prognosis of the patients remaining available for follow-up. Nevertheless, the model most closely describing the available data still shows a stable difference between the treatment groups of 4.2 Sharp–van der Heijde points every year. If we impute the progression of the patients that were lost to follow-up with the best estimation of their real progression rate, there is a sustained and significant difference between the groups in yearly progression rate of 3.1 points per years in favour of COBRA.
Note that this benefit cannot be solely ascribed to the trial treatment. Importantly, treatment strategy after the 1-year trial was uncontrolled, in contrast to more recent trials. As noted, patients in the COBRA group received somewhat more glucocorticoids and biologicals in the follow-up period. The rheumatologists treated the patients to achieve a disease activity level that matched treatment options and expectations at that time. In our view, this mostly explains the numerical differences in treatment intensity and similar levels of disease activity and HAQ (a measure strongly affected by disease activity until late in the disease). In our current understanding, ‘tight control’ over (low) disease activity should be maintained over many years before benefits in disease progression can manifest themselves in improved patient outcome, as expressed by permanent disability, joint replacements, etc.
Not many trials complete such a long and complete follow-up of their patients. The BeSt group recently confirmed in abstract that the benefits of COBRA (or a combination of high dose MTX plus infliximab) on radiographic progression persist up to 5 years.26 The FINRACo trial, comparing a combination treatment of SSZ, MTX, hydroxychloroquine and prednisolone with SSZ alone (with or without prednisolone)27 achieved a similar 11-year follow-up. Although their follow-up was less complete than ours, they did not encounter problems of differential dropout and showed that combination treatment during the first 2 years of disease results in less radiological progression after 11-year follow-up compared to monotherapy.28
This study was part of a project to increase uptake of COBRA therapy in rheumatological practice in The Netherlands. We have detected several barriers to implementation on the part of the rheumatologist, including the workload, fear of prednisolone and the anticipated negative reaction of the patient.19 We addressed these by developing information material for patients and disseminating scientific evidence that contradicts the doctor's beliefs. The current study serves to take away lingering concerns over long-term safety of this strategy, and documents that initial COBRA therapy is as safe as other antirheumatic treatment modalities in the short and long term, under appropriate rheumatology care.
Acknowledgments
We would like to thank Maal van Everdingen and Arco Verhoeven for scoring the radiographs, and Jos Twisk and Piet Kostense for their statistical advice. Furthermore, we want to thank all patients, arthritis nurses and rheumatologists in the different centres that made it possible for us to gather these data.
References
Supplementary materials
Web Only Data ard.2009.108027
Files in this Data Supplement:
Footnotes
-
Funding This study was partly financed by the Dutch Arthritis Association.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the VU University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.