Article Text

Abstract
Background Therapeutic approaches to rheumatoid arthritis (RA) have undergone significant changes. The importance of tight control and early treatment, rapidly altered if goals are not achieved, is supported by evidence. However, it is unknown to what extent these insights are accepted by practitioners in clinical practice.
Objective To obtain information about standard follow-up and treatment practices, and rheumatologists' aims in the care of patients with RA.
Methods A survey conducted at the 2008 EULAR Congress.
Results Most specialists, who were mainly from Europe and Latin America, were well-informed about recent concepts: two-thirds specified remission as a major goal. The experts attempted to reach treatment aims within 12–14 weeks, altering treatment otherwise. Disease activity assessment by composite measures is performed by a majority, although one-third preferentially relied upon their judgment.
Conclusion These results suggest the acceptance of ambitious treatment concepts in practice. Although voluntary surveys have limitations, the answers reflect widespread adoption of desirable standards of care.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
During the current decade, rheumatologists have witnessed a series of major developments in the treatment of rheumatoid arthritis (RA), including new treatments1 which allow one to aim for stringent targets, including remission.2 Outcomes assessment has also been advanced and become easy to use in clinical practice,3,–,5 allowing assessment of disease activity, response to treatment and categorisation of disease activity states.
Strategic trials defining the effect of rapid switching of treatment if response is insufficient using regular disease activity assessments6,–,8 have fostered tight control and targeting of low disease activity or remission by respective algorithms.9
Paradigm changes were also seen in the preceding decade, when early diagnosis and early institution of disease-modifying antirheumatic drugs were in focus.10 11 However, the transformation of insights on early arthritis into clinical practice has lagged behind the research progress as seen upon surveying rheumatologists.12
It is currently unknown to what extent the assessment of disease activity is performed in daily practice, since obtaining composite disease activity indices may not be feasible routinely and, therefore, assessments focusing only on patient-reported outcomes may be preferable.13 There is also insufficient information as to whether tight control and rapid switching of treatment have translated into daily practice.
To examine these issues, we performed a survey among doctors caring for patients with RA. The results of this survey are presented in this report.
Methods
Preparation of the survey
A questionnaire for self-completion using a personal computer was designed. The survey involved nine questions dealing with the monitoring of, and treatment aims for, RA in clinical practice. For details please see online supplementary information. The questions and predefined potential answers were compiled by a steering committee comprising 12 rheumatologists and one patient with RA. They were then transformed into a computerised chart. The survey was performed at the Annual European Congress of Rheumatology in Paris, 2008.
All data analyses were performed using SPSS version 15.0 (SPSS, Chicago, Illinois, USA).
Results
Demographics of participants
At the conference, 1044 participants (mostly from Europe and Latin America (~40%), but also other countries, such as 2% from USA) completed the survey; 1001 of whom indicated that they regularly treat patients with RA. For reasons of simplicity, we will focus the analyses primarily on the results obtained from surveying the 870 rheumatologists (including rheumatology trainees) on the items displayed in online supplementary table 1. The professional characteristics are detailed in the supplementary file (mostly they were hospital-based rheumatologists).
Treatment aims and strategies
Routine assessments
Individual measures of disease activity and composite indices
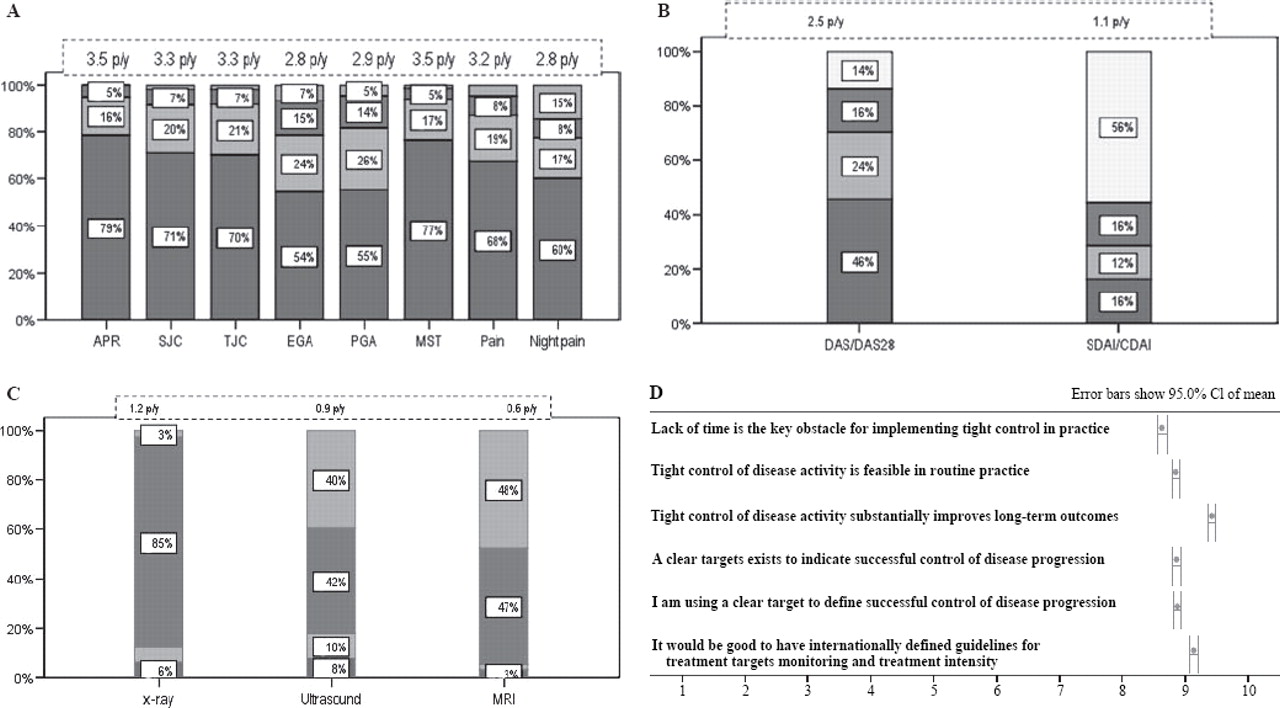
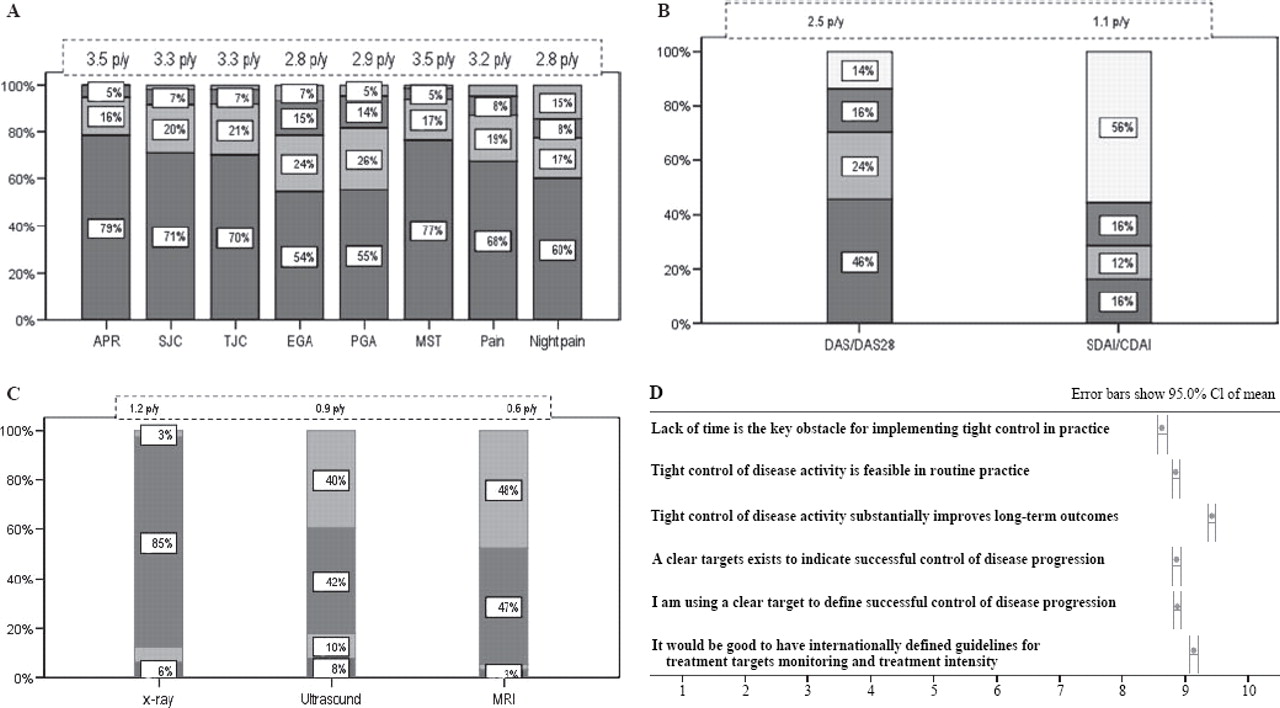
The assessment practice of individual measures of disease activity and the mean frequencies of annual assessments are presented in figure 1A,B.
{kind=link}
Frequency of assessments. Bars represent percentages of rheumatologists who employed or used the respective assessments “at least every 3 months” (red bars), “every 4–6 months” (green bars), less frequently than every 6 months (blue bars; combined results of the three options “every 6–9 months”, “every 1–2 years”, “as mandated by authorities”) and “do not use at all” (grey bars). Average frequencies of respective assessments per year (p/y) are specified above the bars. (A) Proportions of rheumatologists who evaluated, acute phase reactants (APR), swollen joint count (SJC), tender joint count (TJC), evaluator global assessment (EGA), patient global assessment (PGA), morning stiffness (MST), pain and night pain, within the indicated periods. (B) Use of composite indices: percentages of rheumatologists who assessed their patients by composite scores within the indicated period. The average annual frequencies of the Disease Activity Score (DAS) and Simplified Disease Activity Index (SDAI)/Clinical DAI (SDAI/CDAI) assessments are shown above the bars. (C) Proportion of rheumatologists who employed the various imaging modalities within the indicated periods. (D) Results of analyses of numerical rating scales (means ± SD) on the agreement with the statements cited above; the scale ranged from 1= “I strongly disagree” to 10 = “I strongly agree”.
Assessment of physical function and quality of life
A total of 80.2% of respondents said that they used the Health Assessment Questionnaire Disability Index; the greatest proportion of them (29.1%) used it every 3 months (supplementary figure 1) with an estimated number of 1.9 annual assessments. The SF-36 was used by fewer rheumatologists (50.7%) and if so, then less frequently with a mean of 1.1 times a year.
Composite indices
Among the rheumatologists, 45.6% stated that they used the 28 joint count Disease Activity Score (DAS28) at least every 3 months, while only 13.8% did not employ it at all (figure 1B). The Simplified Disease Activity Index (SDAI) or the Clinical Disease Activity Index (CDAI) was used by 16.3% at least every 3 months. Mean annual assessment frequencies were 2.5 for DAS/DAS28 and 1.1 for SDAI/CDAI overall and 2.8±1.3 for DAS/DAS28 and 1.2±1.5 for SDAI/CDAI among score users. Among all respondents, 71 worked in the UK or Germany where the evaluation of the DAS28 is reimbursed; significantly fewer of them did not use composite scores at all (5.6% vs 14.5% in all other countries; p=0.046). Thus, reimbursement appears to increase the proportion of people using composite scores by almost 10%.
Imaging
Radiological follow-up was performed every 1–2 years by 69.5% of the rheumatologists (figure 1C), whereas ultrasound and MRI are not employed in routine practice by the vast majority.
Therapeutic aims and strategies
Participants had to rate their agreement with certain statements on a numerical rating scale from 10 (fully approve) to 1 (fully disapprove).
Major treatment aims
A detailed list of possible answers and respective frequencies of choices made for the question: “What is your major treatment aim for your patients with RA?”, is outlined in table 1 (A) (more than one answer was allowed).
Most rheumatologists (67.9%) defined their major treatment target for patients with RA to be clinical remission measured by a composite index. Also among non-rheumatologists, clinical remission was the number one response (table 1 (A)). Users of composite indices showed a clear trend toward more ambitious treatment goals than non-users.
Of interest, management in hospital practices (academic and non-academic) was very similar to that in office practices (data not shown).
Assessment of treatment response
A total of 59.1% judged the presence of a clinical state as important, while 67.6% used the percentage improvement or absolute improvement of composite scores to evaluate response. Nevertheless, among these latter rheumatologists, 54.3% indicated that they additionally relied on judging clinical state.
Treatment modification to reach target
Persistently high disease activity (76.4%), significant radiographic progression (63.8%) and patient-reported difficulties with daily activities (52.0%) were the main reasons for modifying treatment (table 1 (C)). Tight control was most strongly judged to improve long-term outcome (mean 9.5 points on a 10-point scale; figure 1D).
Additional analyses
Additional analyses on respondents who relied upon their own judgment and responses of non-rheumatologists are shown in the online supplementary file.
Discussion
This survey among almost 900 rheumatologists provides insights into the way patients with RA are followed up in routine practice. Importantly, the vast majority of the rheumatologists indicated that they assess core set variables and composite indices routinely in their patients, usually every 3 months.
When asked for their therapeutic aims, two-thirds indicated that remission using a composite index was their major treatment target, followed by patient satisfaction. More than one-third of the rheumatologists relied on their own judgment of clinical response and, not surprisingly, these used composite indices less frequently than the remainder.
Interestingly, the 131 non-rheumatologists answering the survey gave overall similar responses to those of the rheumatologists and only used control examinations less frequently.
The major question that arises from the results of this survey, which to our knowledge is the first large one of its kind, relates to the reliability of the responses: are the answers a true reflection of the participants' practice or are they merely a reflection of their perception of how patients should best be followed up and treated? Indeed, there are some internal consistencies which suggest that the results may reflect practice: users of composite disease activity indices aimed at more ambitious therapeutic goals significantly more often than rheumatologists who did not primarily use composite scores; the mean of 12–14-week lag period for the decision to switch traditional or biological disease-modifying antirheumatic drugs, respectively, is in line with ambitious therapeutic aims; among doctors originating from countries where reimbursement is offered for obtaining composite indices, the proportion of score users was higher than elsewhere. However, even if the data did not reflect true practice but merely perception of best practice, the results of the survey indicate that the paradigm shift has transpired into clinical practice at least by awareness.
There are several limitations to this study. First, this was only a survey and the results might differ from actual practice. However, the data at least represent the views of participants and can serve as a benchmark on how to approach care of patients with RA in clinical practice; the data also suggest that participants may follow this strategy at least in some of their patients. Second, the data reflect the views of the participants in the survey and not necessarily the general view of rheumatologists; rheumatologists who come to conferences may be particularly interested in the newest developments. Third, academic departments may be over-represented in this survey; however, the data at the least speak the language of the respondents who subsequently may also influence other rheumatologists' views. Fourth, as the survey involved participants of the Annual European Congress, it might be seen as not sufficiently reflecting rheumatologists from other regions; however, about 55% of the respondents were from outside Europe, particularly Latin America (though only 2% from the USA) and their responses were similar to those of European survey participants (data not shown). Finally, this questionnaire was designed by expert opinion and has not been validated; however, it was compiled by a committee of 12 rheumatologists and a patient experienced in clinical studies and went through several discussion rounds before finalisation.
The high penetration of the need for tight control examinations using composite indices and remission as therapeutic goal may be surprising but takes account of the many recent publications on the importance of these goals.6 7 9 14 Nevertheless, about one-third of the rheumatologists trusted their own judgment and saw patient satisfaction as the major aim, a less effective approach than score-mediated tight control.6 It would be interesting to see the results of their patient care compared with those of others, but this is not within the realm of such a study. Nevertheless, the overall results of this survey indicate that the time may be near when rheumatologists will compare the results of their own practice with those of others, benchmarking the care of RA (for example using computerised databases such as CARAbase15).
It will be of interest to repeat this survey in the same respondents as well as re-perform it at future EULAR congresses. Also, similar surveys might be valuable nationally to learn about the penetration of current paradigms and potential differences in care for RA among different countries or healthcare systems.
In conclusion, the data obtained in this survey suggest that most rheumatologists are aware of the need to follow-up patients tightly using composite scores and to aim for remission as a therapeutic goal, and they adopt this practice. This is a reassuring result and it is to be hoped that the survey responses are truly adhered to in the care of all patients with RA around the world.
References
Supplementary materials
Web Only Data ard.2009.108472
Files in this Data Supplement:
Footnotes
-
Funding The study was supported by an unrestricted grant from Abbott.
-
Competing interest Representatives of the company attended the initial meeting, but had no active participation or influence on the decision-making regarding the questions. In addition, none of the questions related to the use of particular treatments. The analyses were performed at the Medical University of Vienna. The handling editor was D T Boumpas.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous