Article Text

Abstract
Background Anti-citrullinated protein antibodies (ACPA) are associated with increased risk for rheumatoid arthritis.
Objective To investigate the effect of the presence and levels of ACPA on arthritis development in patients with arthralgia.
Methods Patients with arthralgia positive for ACPA or IgM rheumatoid factor (IgM-RF) were tested for the shared epitope (SE) and were prospectively followed up for at least 12 months. Absence of clinical arthritis at inclusion and arthritis development during follow-up were independently confirmed by two investigators. Cox regression hazard analyses were used to calculate hazard ratios (HRs) for arthritis development.
Results 147 patients with arthralgia were included (50 ACPA positive, 52 IgM-RF positive and 45 positive for both antibodies). After a median follow-up of 28 months (interquartile range (IQR) 19–39), 29 patients developed arthritis in a median of 4 (IQR 3–6) joints and 26 (90%) of these were ACPA positive. The presence of ACPA (HR = 6.0; 95% confidence interval (95% CI) 1.8 to 19.8; p = 0.004), but not of IgM-RF (HR = 1.4, 95% CI 0.6 to 3.1) nor the SE (HR = 1.5, 95% CI 0.7 to 3.0), was associated with arthritis development. Within the group of ACPA-positive patients, the risk for arthritis was enhanced by the presence of IgM-RF (HR = 3.0; 95% CI 1.4 to 6.9; p = 0.01) and high ACPA levels (HR = 1.7; 95% CI 1.1 to 2.5; p = 0.008), but not the SE (HR = 1.0; 95% CI 0.5 to 2.1; p = 1.0).
Conclusion In patients with arthralgia the presence of ACPA (but not of IgM-RF or SE) predicts arthritis development. The risk in ACPA-positive patients may be further increased by the concomitant presence of IgM-RF or high levels of ACPA.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is an autoimmune disease with frequent occurrence of autoantibodies in the preclinical phase, such as anti-citrullinated protein antibodies (ACPA) and IgM-rheumatoid factor (IgM-RF).1 2 ACPA comprise a group of antibodies that are highly specific for RA: among those described are antibodies against cyclic citrullinated peptide (anti-CCP),3 citrullinated fibrinogen,4 citrullinated a-enolase5 and mutated citrullinated vimentin.6 IgM-RF, an antibody targeting the Fc fragment of IgG is also present in the preclinical phase, but probably at a later stage.2
The occurrence of arthralgia in people with these autoantibodies probably represents a late stage in the preclinical development of (rheumatoid) arthritis, especially if the symptoms are symmetrically located in the small joints, a situation which could be named “inflammatory arthralgia”. Non-specific arthralgia without IgM-RF, on the other hand, is not related to arthritis development.7 In a study of patients with IgM-RF-positive arthralgia, development of RA after 1 year was reported in 17% of the patients.8 Whether the presence of arthralgia increases the risk for RA in ACPA-positive subjects, is likely but not yet known.
The major genetic risk factor for RA is the “shared epitope” (SE) at the HLA-DRB1 locus.9 The SE hypothesis postulates that amino acid sequences bordering the peptide binding groove of the HLA-DRB1 molecule are involved in the pathogenesis of RA—for example, by enabling the presentation of arthritogenic peptides to T cells.9 In support of the latter concept it has been shown that the DRB1*0401 peptide binding groove allows for a high-affinity interaction with citrullinated peptides, resulting in efficient antigen presentation.10 In a study analysing preclinical blood samples of patients with RA, the combination of ACPA and the SE was indeed associated with the greatest risk for RA.11 However, it has also been suggested that the increased risk for RA in SEpositive undifferentiated arthritis is in fact not due to the SE, but to ACPA positivity and levels, suggesting that the SE alleles act as classic immune response genes.12 In a cross-sectional comparison of different stages of arthritis development, we have found evidence that already in the arthralgia stage the effect of the SE on disease risk may be mediated through higher ACPA levels.13
In this study we present data on prospectively monitored arthritis development in ACPA-positive and/or IgM-RF-positive patients with arthralgia at risk for the development of RA, and report the relative contribution of ACPA positivity in relation to ACPA levels and the presence of IgM-RF and the SE.
Patients and methods
Study population
Between June 2004 and 2007, ACPA-positive and/ or IgM-RF-positive patients with arthralgia were recruited at rheumatology clinics in the Amsterdam area of the Netherlands. After screening and global informed consent by telephone, autoantibodies and SE genotyping were determined at least 1 month after the first positive sample; one or both antibodies had to be above the threshold for test positivity on both occasions to allow for inclusion. At the first study visit, a trained medical doctor (WHB) and a senior rheumatologist (DvS) independently scored for absence of arthritis in 44 joints at physical examination.14 The senior rheumatologist was blinded for the reported joint complaints and the autoantibody status. Disagreement resulted in exclusion from the study. Of 227 patients thus recruited, 80 were excluded by the following criteria: arthritis revealed by chart review (n = 5) or baseline physical examination (n = 31), previous treatment with a disease-modifying antirheumatic drug (n = 2), recent glucocorticoid treatment (<3 months) or present treatment with dexamethasone in a randomised placebo-controlled trial with the goal of preventing arthritis development (see article on page xx;14a n = 42; the patients who received placebo in this trial could be included in this study). Erosions on hand or feet x-ray examination, the final exclusion criterion, were not seen in any patient. In total, 147 ACPApositive and/or IgM-RF-positive patients with arthralgia were included in this study.
Details of joint complaints were recorded at baseline and during yearly follow-up visits. As a subgroup of arthralgia, the presence of symmetric arthralgia in wrists, metacarpophalangeal, proximal interphalangeal and/or metatarsophalangeal joints was defined as inflammatory arthralgia. Extra visits were planned if the patient developed arthritis. At such visits, soft tissue swelling in any of the 44 joints14 was independently confirmed by the same two investigators who performed the inclusion visit, and the Disease Activity Score of 28 joints (DAS28)15 was determined as well as whether the patient fulfilled the American College of Rheumatology (ACR) criteria for RA.16
Laboratory investigations
ACPA and IgM-RF levels were determined batchwise at the end of the study period using the serum samples that were obtained at baseline, by second-generation anti-CCP enzyme-linked immunosorbent assay (ELISA) (Axis Shield, Dundee, UK) and in-house ELISA, respectively. The cut-off level for anti-CCP positivity was set at 5 arbitrary units/ml (AU/ml), according to the manufacturer’s instructions. IgM-RF was calibrated with a national reference serum containing 200 IU/ml17; the cut-off level for IgM-RF positivity was set at 30 IU/ml determined on the basis of receiver operating characteristic curves as described previously.2 C-reactive protein (CRP) levels (normal range ,10 mg/l) were determined using the Roche/Hitachi cobas c systems with a detection range of 0.15–20 mg/l (high sensitive CRP). Samples reaching 20 mg/l were diluted further. The test principle consists of a particle-enhanced immunoturbidimetric assay. Human CRP agglutinates with latex particles coated with monoclonal anti-CRP antibodies.
HLA-DRB1 genotyping was performed by sequenced-based, high-resolution typing (Department of Immunogenetics, Sanquin, Amsterdam). The HLA-DRB1*0101, *0102, *0401, *0404, *0405, *0408, *0410 and *1001 alleles were taken to contain the SE.
Statistical analysis
Categorical variables were analysed by Fisher exact or χ2 test when appropriate. Measures with a Gaussian distribution, expressed as the mean and SD, were analysed by t test. Outcome measurements with a non-Gaussian distribution were expressed as the median and interquartile range (IQR) and were analysed by the Mann–Whitney U test. Cox regression hazard analyses were used to separately investigate the influence of ACPA, IgM-RF, SE presence and autoantibody levels on the development of arthritis. Furthermore, the influence on arthritis development of IgM-RF, SE, and autoantibody levels in the presence of ACPA was also assessed using Cox regression hazard analyses. To quantify the effect of IgM-RF and ACPA levels on arthritis development using Cox regression, positive levels were divided into quartiles and entered as continuous variable (one through four). The associated hazard ratio can be interpreted as mean hazard ratio of the first quartile versus the second, the second versus the third, etc. The analyses were performed using SPSS version 16.0 (Chicago, Illinois, USA).
Results
Arthritis development
Table 1 shows the baseline characteristics of the patients. The majority of patients had symmetric distribution of tender joints, morning stiffness was present infrequently. The followup was a median of 28 months (interquartile range (IQR) 19– 39). Twenty-nine patients (20%) developed arthritis after a median of 11 (IQR 5–17) months in a median of 4 (IQR 3–6) joints. Their mean DAS28 at the first visit with arthritis was 4.4 (SD 1.2), and 10/29 patients fulfilled the ACR criteria for RA.
Baseline characteristics of 147 patients*
Inflammatory arthralgia with morning stiffness was uncommon (n = 10; six ACPA positive), but six (five ACPA positive) of these patients developed arthritis during follow-up (versus 23/ 137 in the group without these characteristics, p = 0.004). The other baseline clinical characteristics, as well as CRP levels (3.0 (IQR 1.1–4.7) and 2.3 (IQR 0.9–5.0); p = 0.81), were similar in the groups of patients with and without arthritis during followup. Only 17/147 patients had CRP levels above the normal range (.10 mg/l), and this was also not associated with arthritis development (p = 0.74).
Arthritis development is associated with ACPA status and levels
The percentage of patients positive for ACPA was higher in the group of patients with arthritis than in the group without arthritis (26/29 (90%) vs 69/118 (58%); p = 0.002). The median ACPA levels were higher the group of ACPA-positive patients with arthralgia who had developed arthritis than in the group who had not developed arthritis (141 (IQR 21–304) AU/ml vs 31 (IQR 11–100) AU/ml, respectively; p = 0.005).
SE carriage (45% vs 35%, p = 0.33), IgM-RF positivity (21/29 (72%) vs 76/118 (64%), p = 0.42) and median levels of IgM-RF (72 (IQR 39–119) vs 56 (IQR 39–117); p = 0.36) were similar in the groups of patients with and without arthritis during followup. To correct for the follow-up duration of each patient, Cox regression hazard analysis was performed. These analyses also revealed ACPA status and levels as predictors for arthritis development (table 2).The hazard ratio for ACPA-positive patients was 6.0 (p = 0.004).
Arthritis development is associated with ACPA status and levels: univariate analyses
These data show a significant relationship between ACPA status and levels and arthritis development. In contrast, no significant association was observed between arthritis development and the presence of SE, IgM-RF status or IgM-RF levels.
Arthritis development is associated with IgM-RF in the presence of ACPA
Next, the contribution of IgM-RF, the SE and autoantibody levels in the presence of ACPA was determined, again using Cox regression analyses (table 3).
Arthritis development is associated with IgM-RF in the presence of ACPA
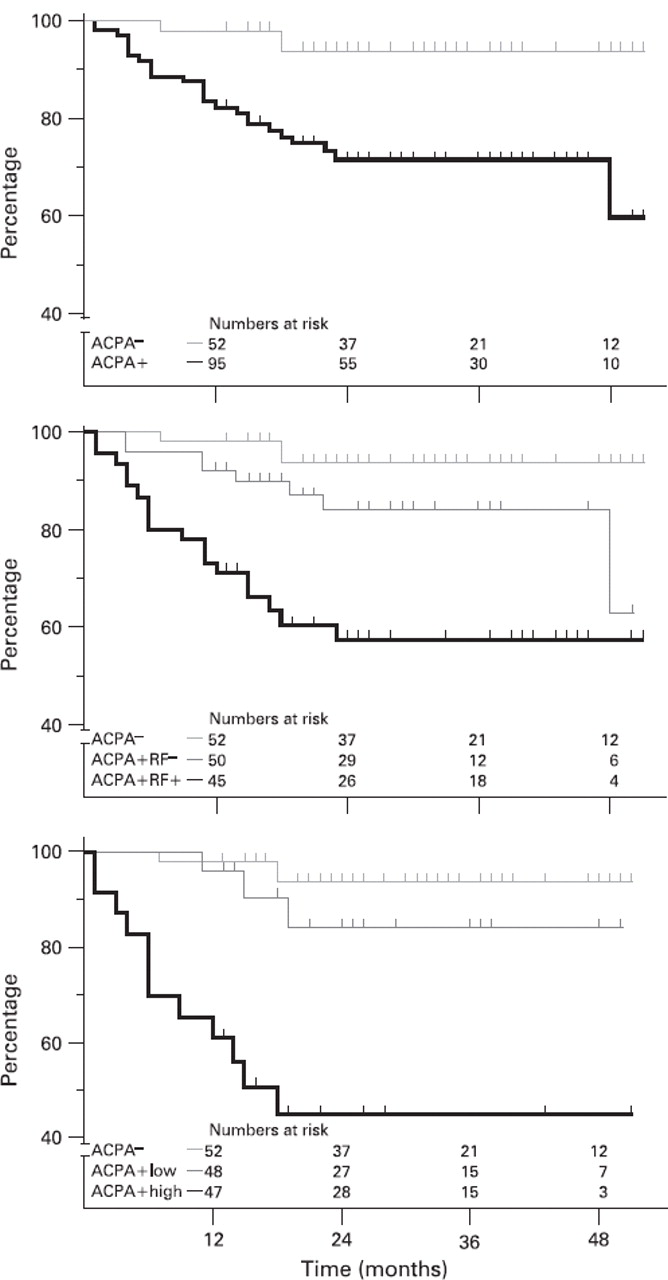
The hazard ratios were calculated with the hazard for ACPAnegative patients as reference. The hazard ratio of ACPA positivity significantly increased with the concomitant presence of IgM-RF (table 3, model 1).To quantify this effect, we compared the risk of arthritis development in ACPA-positive, IgM-RF-positive patients with the risk of arthritis development in ACPA-positive but IgM-RF-negative patients, resulting in a hazard ratio of 3.0 (p = 0.01). IgM-RF levels do not contribute to the risk for arthritis development in the presence of both ACPA and IgM-RF (HR = 1.0; 95% CI 0.6 to 1.4, p = 0.8). Furthermore, when the SE instead of IgM-RF was added to the model, the hazard ratio did not change (table 3, model 2). Gender and age had no influence on the hazard ratios. Figure 1 shows the percentage of patients developing arthritis in the three autoantibody groups (ACPA negative, ACPA positive, ACPA and IgM-RF positive). Figure 2 depicts the corresponding Kaplan–Meier survival curves. These results show that ACPA determines arthritis development in patients with arthralgia and that IgM-RF or high ACPA levels increase this risk. Arthralgia duration before inclusion was not associated with arthritis development, nor did it influence any of the results from the univariate and multivariate analyses.

Arthritis development in patients with arthralgia. Percentage of IgM rheumatoid factor (IgM-RF)-positive, anti-citrullinated protein antibodies (ACPA) negative (left bar); ACPA positive, IgM-RF negative (middle bar) and ACPA and IgM-RF positive (right bar) patients with arthralgia who developed arthritis after a median follow-up of 28 (IQR 19–39) months.

{kind=link}
{kind=link}
The role of anti-citrullinated protein antibodies (ACPA) and IgM rheumatoid factor (IgM-RF) in arthritis-free survival of patients with arthralgia, as plotted by Kaplan–Meier curves. (Upper graph) ACPAnegative, IgM-RF-positive patients (light grey line) are compared with ACPA-positive patients (black line). (Middle graph) ACPA-negative, IgMRF-positive patients (light grey line) are compared ACPA positive, IgMRF-negative patients (dark grey line) and ACPA and IgM-RF-positive patients (black line). (Lower graph) ACPA-negative, IgM-RF-positive patients (light grey line) are compared with ACPA low (below 25% centile (12 AU/ml)) patients (dark grey line) and ACPA high (above 75% centile (156 AU/ml)) patients (black line). The corresponding Cox regression hazard ratios are reported in tables 2 and 3.
Discussion
This study shows that the risk for arthritis development in ACPA-positive and/or IgM-RF-positive patients with arthralgia is strongly associated with ACPA status. The presence of IgMRF, and high levels of ACPA further increase the risk for arthritis development. These data prospectively confirm and extend observations in patients with asymptomatic preclinical RA or early arthritis,11 18 as well as in rodents19 20 on the presumed pathophysiological role of ACPA in RA. Since the presence of ACPA or IgM-RF seems an evidence-based first step in the detection of those patients with arthralgia at risk for the development of arthritis, an ACPAand IgM-RF-negative reference group was not included in this study.
The frequency of the SE was higher in those developing arthritis (45% vs 35%), although this did not reach statistical significance. The presence of the SE was not associated with arthritis development when ACPA was present. The latter is in line with previous observations in undifferentiated arthritis, suggesting that the contribution of the shared epitope to RA development is mediated via the presence and perhaps levels of ACPA.12
IgM-RF only enhanced the risk for arthritis development in the presence of ACPA, which is compatible with a role of IgMRF as marker of inflammation, secondary to the rheumatoid inflammatory process that may be induced or enhanced by ACPA.21 This is underlined by the fact that ACPA antibodies precede IgM-RF in the preclinical phase.2
The 6% rate of IgM-RF-positive, ACPA-negative patients with arthralgia who developed arthritis in 2 years is still considerable compared with the calculated 5-year risk of 1.5% which our group has found in IgM-RF-positive healthy blood donors.2 Incidentally, it should be noted that these figures were obtained with a higher cut-off value (30 IU/ml) of the IgM-RF assay than is usually applied, especially in many primary care laboratories. Although the study groups cannot be formally compared, it seems that the presence of arthralgia enhances arthritis risk in IgM-RF-positive subjects. A similar observation was made for ACPA-positive subjects: 27% of patients with arthralgia developed arthritis in 2 years, this is clearly higher than the 5-year risk of 5% in healthy blood donors.2
A small number of patients (10, of whom six were ACPA positive) were characterised by morning stiffness and “inflammatory type arthralgia”—that is, the presence of symmetric arthralgia in hand and/or foot joints. Six of these patients (five ACPA positive) developed arthritis suggesting that this type of arthralgia is associated with arthritis development, but obviously a larger number of patients is needed to confirm such an association.
Forty per cent of ACPA-positive and IgM-RF-positive patients with arthralgia have developed arthritis after a median follow-up of slightly over 2 years. This high frequency suggests that the arthralgia of autoantibody-positive subjects is often caused by the rheumatoid inflammatory process that has not yet reached sufficient intensity to be detectable clinically or by means of CRP, since CRP levels were in the normal range for most patients and were not associated with arthritis development. It is conceivable that sensitive imaging techniques such as ultrasound, magnetic resonance imaging or even positron emission tomography may be able to detect subclinical synovitis in these patients. A further study of preclinical RA will allow better assessment of the risk of arthritis development in various subgroups. Interventions can then be directed to the subgroups with the highest risk. The therapeutic possibilities in this stage of the disease have only just begun to be explored.14a
In summary, the presence of ACPA, but not of IgM-RF or SE, predicts arthritis development in patients with arthralgia. This risk may be further increased with the concomitant presence of IgM-RF or high levels of ACPA and provides further evidence for the pathophysiological role ACPA plays in RA.
Acknowledgments
We thank Margret de Koning and Roel Heijmans for their technical assistance and Mike Peters for critically reading the manuscript. Funding This study is financially supported by the Netherlands Organisation for Health Research and Development (ZonMw), grant number 6100.0010.
References
Footnotes
-
Competing interests None.
-
Ethics approval Approval from the ethics committee, Jan van Breemen Instituut/ Slotervaart Hospital, Amsterdam, The Netherlands.
The funding source did not have any involvement in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
-
Provenance and peer review Not commissioned; externally peer reviewed.