Article Text

Abstract
Anti-endothelial cell antibodies (AECA) are a heterogeneous class of antibodies whose role in the pathogenesis of autoimmune diseases with vascular involvement has been extensively studied. Systemic sclerosis (SSc) is one of the systemic autoimmune diseases in which endothelial dysfunction is well defined and important in the development of the disease. AECA are present in the serum samples of many patients with SSc. Depending on the detection method and on patient selection, 22–86% of patients test positive for AECA. Among the demonstrated clinical associations, lung and peripheral vascular involvement are the most common. In this paper, the methods of detection, various molecular specificities and the possible pathogenic mechanisms of AECA in SSc are reviewed.
Statistics from Altmetric.com
More than three decades ago, anti-endothelial cell antibodies (AECA) were detected for the first time in sera from patients with various rheumatic diseases by an indirect immunofluorescence (IIF) technique using rat livers—by Linquist and Osterland, 19711—or mouse kidneys—by Tan and Pearson, 1972.2 AECA are a heterogeneous group of autoantibodies that specifically recognise endothelial cell proteins and molecules present on the endothelial cell surface, and their presence has been studied since in various diseases with vascular involvement, such as connective tissue diseases (CTDs), vasculitis and atherosclerosis. Their heterogeneity and the multitude of mechanisms by which they might interact with endothelial cells (ECs) offer a rich field for hypotheses to explain disease pathophysiology and clinical variability.
Systemic sclerosis (SSc) is an autoimmune CTD characterised by microvascular injury, cutaneous fibrosis and distinctive visceral changes, mainly affecting the lungs, heart, kidneys and gastrointestinal tract. Although incompletely understood, its pathogenesis associates inflammation with altered T-cell responses, autoantibody production, microvascular and fibroblast dysfunction, resulting in collagen overproduction and fibrosis. Over 90% of patients have antinuclear antibodies, and disease-specific antibodies have been identified, among which are anticentromere antibodies, anti-topoisomerase I antibodies (previously known as anti-Scl-70) and anti-RNA polymerase III antibodies.3
Two disease subsets are currently recognised: limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc).4 5 6
Although the precise mechanism of the vasculopathy in SSc remains largely unknown, there is convincing evidence that endothelial changes are among the earliest pathogenic events.7 Intimal proliferation and inefficient angiogenesis lead to small vessel deformities and obliteration. Patients frequently develop digital ischaemic ulcerations and pulmonary arterial hypertension (PAH) as a result of vascular involvement of the disease. Furthermore, renal failure (also called “scleroderma renal crisis”) is also due to vascular involvement. There is consistent evidence that AECA in scleroderma are associated with these severe forms of vascular involvement.8 9 10 11 12
The numerous studies focusing on the importance of AECA in SSc report largely variable results for AECA prevalence, their target antigens and/or their pathogenic role. This may be caused by the heterogeneity of the disease, but probably more importantly by differences in AECA detection methods. There are interesting data suggesting that AECA might be pathogenic in SSc, yet the precise role of AECA in this disease remains subject to further research. This review presents the various detection methods for AECA, their putative target antigens and the current knowledge of the role of AECA in the pathogenesis of SSc.
AECA detection: methods, substrates and results in SSc
The most frequently used AECA detection methods are immunofluorescence, ELISA and immunoblotting.
The first technique used for AECA detection was IIF, but AECA are at present only infrequently tested by this method.13 However, this technique was recently revitalised by showing good discriminative capacity for SSc lung fibrosis. Wusirika et al found that all healthy controls and patients with SSc without lung fibrosis tested negative, while 42/45 patients with interstitial lung involvement were positive for AECA as tested by IIF on rodent lungs.14
Being more sophisticated and time consuming, immunoblotting techniques are mainly used in studies aiming to identify AECA target antigens.11 Immunoblotting techniques, which use EC lysates, also identify intracellular antigens, which under normal conditions are not accessible by AECA in vivo, unless EC apoptosis has resulted in their exposure.
The method most widely used method for detection of AECA is ELISA. The most frequently used substrate is cultured human umbilical vein ECs (HUVECs). As the specific vascular lesion in SSc is localised in the microvasculature, more recent studies have used microvascular ECs. The advantage of this substrate has been demonstrated by Renaudineau and coworkers, who compared four EC substrates in a study of AECA in SSc. The prevalence of antibodies reacting with (microvascular) bone marrow endothelial cells was significantly higher than the prevalence of antibodies reacting with HUVECs, a mixed endothelial–epithelial cell line (EA.hy 926) and/or Kaposi sarcoma EC.15 Since antibody populations were not completely overlapping, overall AECA positivity reached 50% of the tested sera, suggesting that antigens that are recognised by AECA in SSc also differ from one patient to another.16
Another important methodological point regarding AECA testing is whether the ECs are fixed or not. During the fixing process, permeabilisation of the substrate EC membranes occurs and intracellular antigens become accessible to autoantibodies which would not interact with ECs in vivo. This problem can be overcome by using unfixed cells.17 18
Recently, Youinou et al13 suggested that different methods (ELISA, FACS and western blotting) should be used together in research, since they are complementary, while for diagnostic purposes a standardised ELISA should be developed in the future.
Standardisation of AECA testing, however, has been difficult for several reasons. First, depending on their macrovascular or microvascular origin, ECs have various patterns of surface antigens. Division of AECA into antibodies against microvascular ECs and antibodies against macrovascular ECs19 has proved to be rational and helpful. Second, ECs derived from different anatomical compartments of liver, kidney or lung tissue express different patterns of surface antigens.20 Third, cultured ECs have a high degree of phenotypic instability. Therefore several attempts have been made to establish stable, permanent cell lines, such as EA.hy 929, resulting from a fusion between HUVECs and the permanent epithelial cell line A 549/821 or EVLC2, a simian virus 40 large T-antigen immortalised HUVEC cell line.22 However, even these cell lines are variable in their expression of membrane antigens. Differences were found between cell lines, as well as within the same line, since cells proved to be unstable even over short time periods.13 23
To avoid these difficulties of substrate heterogeneity, Youinou used expression libraries of cDNA complementary to mRNA extracted from ECs and transfected into prokaryotic or eukaryotic cells.24 Whether these transfected cells will be used for diagnostic purposes remains to be seen.
Prevalence of AECA in SSc, clinical associations and lack of disease specificity
Prevalence of AECA in patients with SSc ranged from 22% to 86% in different studies (table 1). This variability is probably due to differences in patient populations, in detection techniques and substrates and in the chosen cut-off point. High variability in AECA positivity has also been noted in patients with other CTDs.18 For instance, AECA prevalence ranges from 15% to 88% in systemic lupus erythematosus (SLE), from 0% to 87% in rheumatoid arthritis (RA) and from 19% to 81% in Wegener’s granulomatosis (WG).25 AECA were also identified in patiens with diabetes mellitus, pre-eclampsia, multiple sclerosis and even in healthy subjects.26 27 It has been suggested that in SLE, RA and systemic vasculitis, AECA titres correlate with disease activity.28 29 30
Prevalence of anti-endothelial cell antibodies in patients with systemic sclerosis as detected by various methods
To our knowledge there are no studies comparing AECA levels and disease activity of SSc. The presence of AECA, however, apparently correlates with more severe forms of SSc and more extensive organ/system involvement.8 9 10 11 12 Most authors found associations of AECA with digital ulcers and gangrene,8 9 10 with nailfold capillaroscopic changes8 9 and with PAH.9 10 In one study, AECA-positive patients with digital infarcts and PAH had significantly higher AECA levels than AECA-positive patients without these features.10 There are contradictory results concerning AECA association with dcSSc and with heart and interstitial lung involvement, but one should keep in mind that all these studies analyse rather small patient groups and some may also have false-positive results by omitting to adjust for multiple testing.
Target antigen(s)
By blotting EC extracts, antibodies reactive with identifiable electrophoresed antigens can be detected. Several studies claimed to identify disease-specific immunoblot patterns in SLE,28 RA36 and/or WG.37 Also in SSc, several studies claimed to identify specific target antigens, although different antigens are described from one study to another.
In one study, García de la Peña-Lefebvre and colleagues concluded that AECA from patients with diffuse SSc, with or without anti-topoisomerase I (anti-Scl-70) antibodies, bind to EC topoisomerase I.38 The authors performed a systematic analysis of autoantibody repertoires in patients with SSc by using extracts from various cultured cells and from normal human tissues as source of self-antigen, in a quantitative immunoblotting technique. The majority of sera from patients with anti-topoisomerase I (anti-Scl-70) antibodies, as well as some sera from patients with SSc without specific autoantibodies, showed IgG reactivity with a 100 kDa band from lung, kidney and oesophagus tissue. These sera were also positive for IgG, reacting with a 100 kDa band from HUVECs, Hep2 and human microvasculature ECs of lung and dermal origin, while all sera from patients with SSc with anticentromere antibodies did not. The authors concluded that IgG and IgM from patients with limited or diffuse SSc exhibit specific and mutually exclusive reactivity patterns, supporting the concept that the autoantibodies from these patients specifically bind to different target antigens in ECs. Sequencing of the 100 kDa protein band from the HUVEC extract identified DNA topoisomerase I as the target antigen.
The same research group identified the ubiquitous nuclear protein CENP-B as the main target of AECA in patients with lcSSc , by quantitative immunoblotting using extracts from HUVECs and human microvasculature ECs.39 40
These observations are partially in accordance with older studies. Thus, Alderuccio et al41 identified, in SSc sera, antibodies reacting with a doublet of 95 kDa and 100 kDa nuclear proteins from ECs of human and bovine origin, supposed to be a larger form of the Scl-70 autoantigen. In another study Hill and coworkers11 found, in lcSSc sera, AECA with anticentromere activity. However, the functional consequences of AECA showing anti-topoisomerase I or anticentromere reactivity are incompletely understood.
Pathogenic role of AECA in SSc
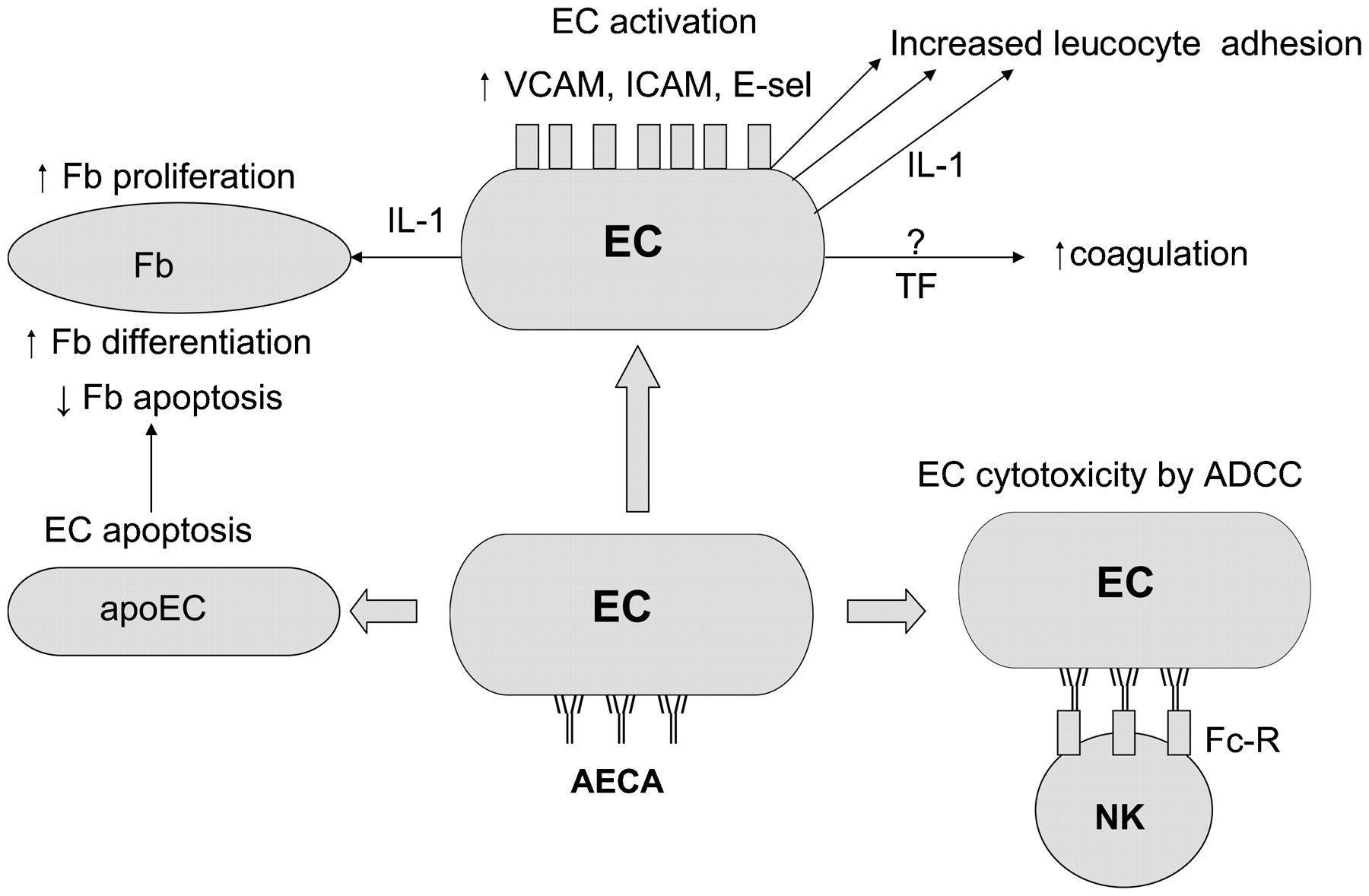
The question of whether AECA are just an epiphenomenon in SSc, or whether they act as an important pathogenic agent in the induction of the endothelial dysfunction and damage seen in SSc, was raised a long time ago. Figure 1 presents a number of mechanisms by which AECA might be involved in the development of SSc.
{kind=link}
Mechanisms by which anti-endothelial cell antibodies (AECA) might be involved in the development of systemic sclerosis (SSc). ADCC, antibody-dependent cell cytotoxicity; apoEC, apoptotic endothelial cell; E-sel, E-selectin; ICAM, intercellular adhesion molecule; IL, interleukin; TF, tissue factor; VCAM, vascular cell adhesion molecule.
EC activation and induction of coagulation
Injury and/or activation of ECs in SSc has been demonstrated in a large number of studies showing increased levels of various endothelial markers such as von Willebrand factor, endothelin-1 (ET-1), thrombomodulin and vascular adhesion molecules.42 43 44 45 There is strong evidence that adhesion molecules are upregulated on ECs in SSc, both within lesions and at clinically uninvolved sites.46 47 This is thought to be one of the earliest pathogenic events in SSc, since it has been shown that the expression of adhesion molecules is already increased in the affected skin of patients with recent-onset SSc.48
High levels of soluble adhesion molecules are found in patients with dcSSc, but not in those with lcSSc where levels are similar to those from patients with primary Raynaud’s disease.49 Carvalho and colleagues showed that pretreatment of human ECs with SSc AECA-positive sera or IgG led to significant increased adhesion of monocytic U937 cells, in a dose-dependent manner, accompanied by increased expression of E-selectin, intercellular adhesion molecule-1, and vascular cell adhesion molecule-1.33
A large number of mediators are overproduced by ECs of patients with SSc, including growth factors and cytokines; among these, ET-1 has been receiving most attention.50 ET-1 activates the surface expression of intercellular adhesion molecule-1 on fibroblasts, and collagen production by both dermal and pulmonary fibroblasts. It can also stimulate fibroblasts to exhibit potent procontractile properties and promote the formation of highly contractive myofibroblasts.51 52 Treatment with ET-1 receptor blockers has been found effective in PAH and digital ulcer prevention in SSc.53 Interestingly, in in vitro studies incubation of HUVECs with AECA-positive sera from patients with SLE and pre-eclampsia resulted in enhanced release of ET-1.54 55 Whether this is also true for sera from AECA-positive patients with SSc, however, needs to be demonstrated.
Coagulation has been shown to be significantly activated in patients with SSc, while fibrinolysis is impaired.56 These alterations have been considered to be consequences of endothelial injury and are supposed to contribute to chronic peripheral ischaemia.57 In vitro IgG from AECA-positive SLE sera induced the expression of tissue factor on HUVECs that were incubated with low doses of tumour necrosis factor α.58 This effect, however, has not yet been demonstrated for sera from AECA-positive patients with SSc.
Cytotoxicity and AECA-induced EC apoptosis
Endothelial injury has long been recognised as one of the main pathological features in SSc, having an early onset in the course of the disease. This led to the hypothesis that a serum factor might induce vascular damage. Studies in the 1980s focused on various effects of SSc sera on cell cultures,59 60 61 62 63 64 65 and the observed prevalence of SSc sera cytotoxicity ranged from 19% to 75%. Some of these studies61 62 64 demonstrated antibody-dependent cell cytotoxicity mediated by SSc sera on various EC substrates, a mechanism also described in SLE66 and in WG.67 The effector cells involved in this cytotoxicity possess Fc receptors and the responsible serum factor(s) is present in IgG-containing fractions. Control studies, using sera from normal controls and from patients with either diabetes or extensive atherosclerotic vascular disease, failed to show cytotoxicity.64 66
Some authors assumed the cytotoxic factor in SSc serum to be a protease.59 68 This hypothesis remains interesting because further research69 demonstrated the presence of a 60 kDa granzyme in SSc sera, inducing profound EC growth inhibition while having a mitogenic effect on fibroblasts. The identification of this granzyme in SSc suggests an important role for cytotoxic T cells and/or NK cells in endothelial injury.
Excessive apoptosis as a key phenomenon in the pathogenesis of several CTDs has been the subject of intense study and debate throughout the past decade. The hypothesis that AECA are involved in the pathogenesis of SSc by inducing EC apoptosis has been tested both in vitro and in vivo.
Incubation of ECs with AECA isolated from patients with SSc resulted in the expression of phosphatidylserine on the surface of the cells, an early characteristic of cells undergoing apoptosis.70 This was not the case with AECA-negative SSc sera, nor with sera positive for antiphospholipid, anti-dsDNA, anti-ribonucleoprotein and/or rheumatoid factor antibodies. Interestingly, apoptosis-inducing AECA did not recognise the Fas receptor, suggesting that the observed effect of AECA was not Fas-mediated.
Another study demonstrated that AECA-induced EC apoptosis in SSc is triggered by an antibody-dependent cell cytotoxicity mechanism. By incubating cultured human dermal microvascular ECs with AECA-positive sera from patients with SSc, EC apoptosis was found in the presence of activated NK cells and could be inhibited by pretreatment with anti-Fas ligand antibodies.71 The same experiments carried out with macrovascular ECs (HUVECs) instead of human dermal microvascular ECs, or with AECA-negative SSc serum samples, were negative.
Furthermore, the induction of endothelial apoptosis by AECA has been demonstrated in vivo using the chicken model of systemic sclerosis UCD-200. Direct transfer of AECA-positive UCD-200 serum into normal chicken embryos led to binding of AECA to the microvascular ECs in the chorioallantoic membrane, as detected by immunofluorescence, and subsequently, to EC apoptosis as detected by the TUNEL technique. The same tests, performed with AECA-negative serum from other chicken lines (UCD058, NWL and OS), led to negative results.72 In the avian models of SSc UCD-200 and UCD-206, EC apoptosis was found to be an early event in the pathogenesis of scleroderma: all UCD-200/206 combined biopsy samples, even in a very early stage of the disease, showed apoptotic cells in the deeper dermis, further identified as ECs.73 Since combined biopsies from 39/45 UCD-200/206 chicken were positive for AECA in IIF, and all sera from these animals were also AECA positive, AECA have been supposed to induce EC apoptosis. EC apoptosis has also been found in skin biopsy samples from patients with SSc with early disease, but in not in those with late disease.73
Interaction of EC with fibroblasts
Uncovering the link between microvascular injury and fibrosis in the pathogenesis of SSc is one of the most ambitious goals. It has been hypothesised that some AECA may also ligate to fibroblasts in vivo, triggering fibroblast activation and thus directly connecting AECA with fibrosis.11
Denton et al elegantly demonstrated that soluble factors released by ECs modulate fibroblast properties. When fibroblasts were co-cultured with ECs, fibroblast proliferation was observed, showing evidence for a link between endothelial activation and fibroblast dysfunction in scleroderma.74 The same researchers showed that EC-derived interleukin 1 and basic fibroblast growth factor are important factors that modulate fibroblasts and that lesional scleroderma fibroblasts are more responsive than control fibroblasts to EC-induced modulation.75
A C-terminal fragment of the domain V of perlecan was recently identified as one of the fibrogenic mediators present in the medium conditioned by apoptotic ECs.76 This peptide activates the PI3K pathway and induces myofibroblast differentiation with expression of α-smooth muscle actin, formation of stress fibres and production of collagen I. This suggests that a chronic increase in endothelial apoptosis and/or increased sensitivity of fibroblasts to mediators produced by apoptotic ECs could form the basis of a fibrotic response.
Conclusions
AECA, although not specific to SSc, remain a very interesting topic of research. Their importance in disease pathogenesis is sustained by some of their demonstrated roles: EC activation, antibody-dependent cell-mediated cytotoxicity and endothelial apoptosis, the last of these possibly triggering the fibrosing process that defines SSc. A further argument for a pathogenic role is the clinical association of AECA in patients with SSc with PAH and severe peripheral vascular involvement. On the other hand, AECA in SSc seem to be directed to topoisomerase I and CENP-B, and the functional consequence of this binding is completely unclear. In addition, the presence of AECA in a large variety of diseases and in healthy subjects, their great heterogeneity and the small number of studies on their functional abilities do not let us firmly rule out the possibility that AECA are just an epiphenomenon in SSc. AECA testing in patients with SSc is at present not indicated in clinical practice. Further research on this topic, including longitudinal studies in patients with SSc, is mandatory for a better understanding of the clinical value and the pathophysiological role of AECA in SSc.
REFERENCES
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.