Article Text

Abstract
Objective: To examine the association of radiographic progression and disease activity states in patients with rheumatoid arthritis (RA) treated with methotrexate with or without infliximab.
Methods: Patients (n = 1049) with active RA for 3 years or less and no previous methotrexate treatment were randomly assigned (4 : 5 : 5) to receive methotrexate plus placebo or methotrexate plus infliximab 3 or 6 mg/kg at weeks 0, 2 and 6, and every 8 weeks thereafter to week 46. Disease activity was classified by the simplified disease activity index as remission (⩽3.3), low (>3.3 to ⩽11), moderate (>11 to ⩽26), high (>26). Radiographic progression was measured as a change from baseline to week 54 in total Sharp score.
Results: At weeks 14 and 54, more patients receiving methotrexate plus infliximab than methotrexate plus placebo were in remission (10.7% versus 2.8% week 14; 21.3% versus 12.3% week 54; p<0.001 for both). Methotrexate plus placebo halted radiographic progression only if patients achieved remission within 3 months, whereas methotrexate plus infliximab also halted or minimised progression in patients with low or moderate activity, respectively. Patients with persistently high disease activity levels had much less progression of joint damage if treated with methotrexate plus infliximab versus methotrexate monotherapy. Even with infliximab plus methotrexate there was a direct relationship between disease activity and radiographic changes, although the slope was deflected when compared with methotrexate monotherapy.
Conclusion: With methotrexate, joint damage progresses even at low and moderate disease activity levels, whereas methotrexate plus infliximab inhibits radiographic progression across all disease activity states.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory joint disease involving the production of proinflammatory cytokines, especially tumour necrosis factor (TNF)α. Often, there is rapid development of joint damage characterised by bone erosions and cartilage injury, which frequently leads to significant disability.1 Agents that block TNFα, including infliximab, etanercept and adalimumab, especially in combination with methotrexate, have been shown to reduce joint inflammation significantly, slow radiographic progression of joint damage and improve physical function in clinical studies of both advanced and early RA.2 The Active-Controlled Study of Patients Receiving Infliximab for the Treatment of Rheumatoid Arthritis of Early Onset (ASPIRE) trial3 is the focus of our current retrospective analysis, in which we examined the association of radiographic progression and disease activity, as assessed by composite indices, throughout the course of the study.
Results of a recent strategic trial suggest that intensive management of disease-modifying antirheumatic drug (DMARD) therapy, with the goal of achieving low disease activity (defined as a disease activity score <2.4 and a fall in this score from baseline by >1.2), leads to important clinical and functional benefit associated with a reduction in joint damage when compared with routine care.4 However, despite the achievement of low disease activity in the vast majority of patients, there was still significant radiographic progression observed in many patients.4 In a similar trial with the aim of achieving low disease activity, the use of traditional DMARD was also associated with the progression of joint damage.5 These data indicate that striving for low disease activity with traditional DMARD monotherapy such as methotrexate may not be sufficient to stop the progression of joint destruction. Whereas the extent to which low progression of joint damage affects long-term outcome is not yet fully understood, it has recently been reported that, among patients meeting stringent criteria for clinical remission, those with total Sharp scores greater than 23 have significant irreversible disability on the group level.6
All of these data suggest that the treatment goal of clinical remission, rather than low disease activity, may lead to better functional and radiographic outcomes. In the present study we evaluated the progression of joint damage in the various disease activity categories defined by respective values of composite indices (remission, low, moderate and high) among patients treated with methotrexate monotherapy when compared with methotrexate plus infliximab therapy.
PATIENTS AND METHODS
Patients
Patient eligibility criteria for the ASPIRE trial were reported previously.3 Briefly, patients were at least 18 years of age but not older than 75 years, had persistent synovitis for 3 months or more and 3 years or less, 10 or more swollen joints and 12 or more tender joints; and one or more of the following: positive test for serum rheumatoid factor, radiographic erosions of the hands or feet, or serum C-reactive protein value of at least 2.0 mg/dl.
Study protocol
The protocol was approved by an institutional review board at each study centre and carried out according to the Helsinki Declaration of 1975, as revised in 1983 and 1989. Patients were randomly assigned to receive one of three treatments in a 4 : 5 : 5 ratio: methotrexate plus placebo, methotrexate plus infliximab 3 mg/kg and methotrexate plus infliximab 6 mg/kg.3 As the two methotrexate plus infliximab groups showed similar radiographic progression of joint damage,3 they were pooled for this analysis. Additional protocol details have been published previously.3 The mean methotrexate doses among all randomly assigned patients at week 54 were 15.1, 15.5, and 14.9 mg/week for the methotrexate plus placebo, methotrexate plus infliximab 3 mg/kg, and methotrexate plus infliximab 6 mg/kg groups, respectively.3
Study evaluations and analyses
For this analysis, disease activity was measured at baseline, week 14 and week 54 using the simplified disease activity index (SDAI)7 and clinical disease activity index (CDAI).7 8 Disease activity was also assessed using the disease activity score, employing the 28-joint count and erythrocyte sedimentation rate (DAS28-ESR).9 The SDAI was calculated as the linear sum of the following outcome variables: tender joint count and swollen joint count based on a 28-joint assessment, patient’s and physician’s global assessments of disease activity (both on a visual analogue scale (VAS) ranging from 0 to 10 cm) and C-reactive protein (mg/dl). The CDAI was calculated as the sum of the tender joint count, swollen joint count (both based on a 28-joint assessment) and the patient’s and physician’s global assessments of disease activity (both on a VAS ranging from 0 to 10 cm). Joint examinations were performed by an independent assessor who had no knowledge of the patient’s treatment assignment. Disease activity was classified as follows based on SDAI scores: remission (⩽3.3), low (>3.3 to ⩽11), moderate (>11 to ⩽26) or high (>26). Remission was also determined using the DAS28-ESR score (<2.6) and CDAI score (⩽2.8). Categorisation of disease activity states was performed by the SDAI and CDAI criteria,10 because the remission criteria have been shown to be more stringent than those by the DAS28-ESR and the modified American College of Rheumatology (ACR) response criteria, because the latter allow for significant residual disease activity.11 12 Consequently, smaller proportions of patients are typically classified as in remission by SDAI and CDAI criteria than by DAS28-ESR and modified ACR criteria.13 14
Radiographs of the hands and feet were taken within 4 weeks of the first dose of study drug and at weeks 30 and 54, or upon premature withdrawal of the patient from the study, as described previously.3 Radiographic progression of joint damage was the change from baseline to week 54 in the van der Heijde modification of the total Sharp score. Two readers scored the radiographs independently without knowledge of treatment assignment, clinical response, or the order of the radiographs. For each set of radiographs, the mean score of the two readers was used for the analyses. The statistical significance of differences between treatment groups was tested using the χ2 test for categorical measures, and using analysis of variance on the van der Waerden scores for radiographic progression. This test converts the ranks to quantiles of the normal distribution, ie, the van der Waerden scores and provides the efficiency of the standard analysis of variance analysis when the normality assumptions are in fact satisfied and also provides the robustness of non-parametric tests when the normality assumptions are not satisfied.
RESULTS
Characteristics of the patients
As previously reported,3 1049 patients were randomly assigned to receive study medication. The baseline characteristics of the study patients with early RA were similar among the three treatment groups, with a mean duration of disease of 0.9 years. The mean DAS28-ESR, CDAI and SDAI scores at baseline indicated that study patients had a high level of disease activity (table 1).
Disease activity
Greater proportions of patients who received methotrexate plus infliximab achieved clinical remission by SDAI at weeks 14 and 54 when compared with the methotrexate plus placebo group (p<0.001; fig 1). The proportions of patients achieving remission using the CDAI were similar and in line with previous observations,13 the proportions reaching remission by DAS28-ESR were higher than by SDAI or CDAI. For example, at week 54, the proportions of patients achieving remission in the methotrexate plus placebo and methotrexate plus infliximab groups were 16.3% and 24.7%, respectively, when assessed by DAS28-ESR, compared with 12.3% and 21.3% (SDAI) and 13.6% and 22.3% (CDAI), respectively.
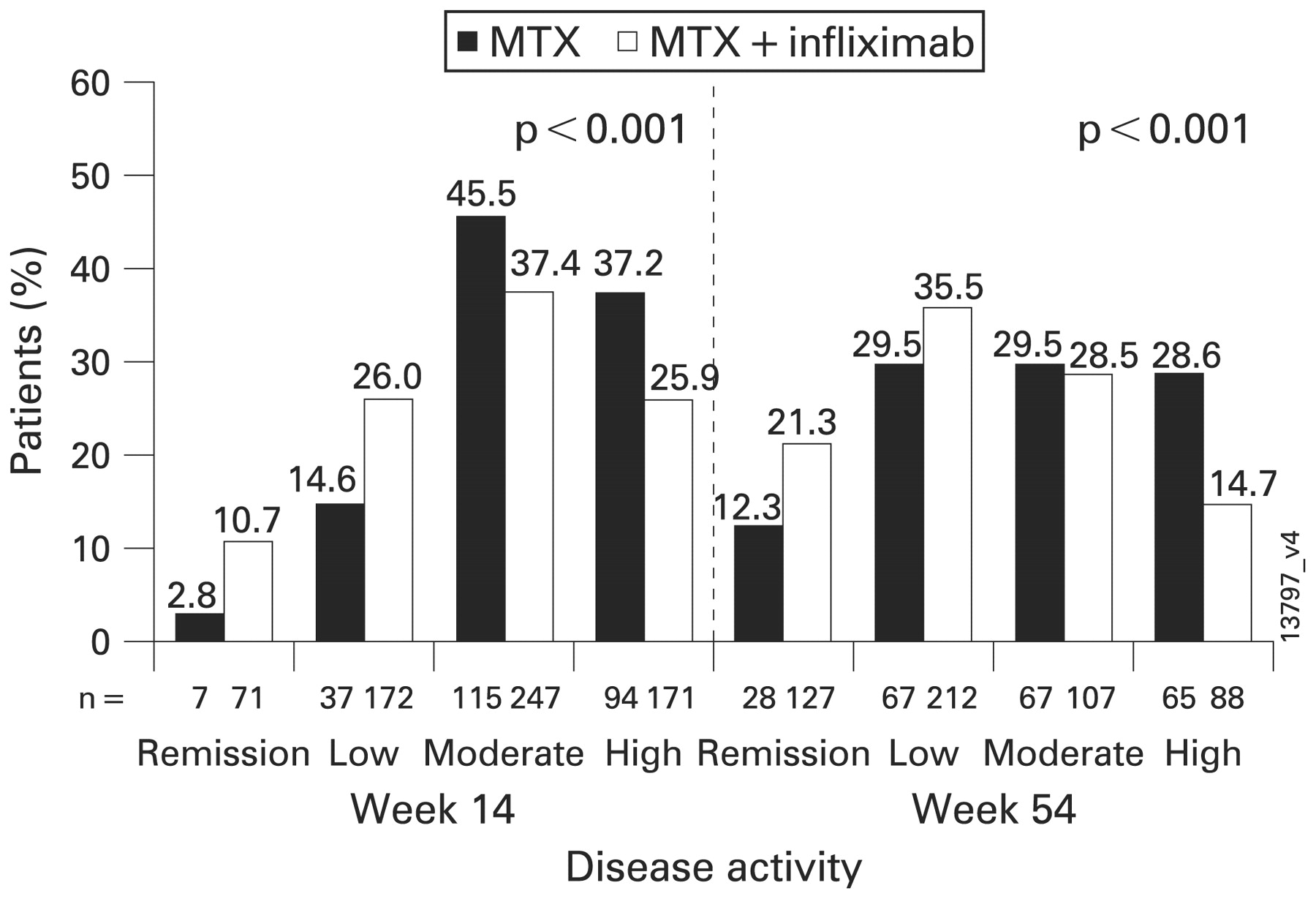
Disease activity categories, as classified by the simplified disease activity index, attained on therapy, at weeks 14 and 54. MTX, methotrexate.
Radiographic evaluation of joint damage
Among patients treated with methotrexate plus placebo, only those who achieved remission, as assessed by the SDAI, by week 14 had minimal progression of radiographic damage at week 54 (fig 2). However, if these patients achieved remission at week 54, they were not protected from at least some radiographic progression (fig 2). Moreover, if patients receiving methotrexate plus placebo achieved only low disease activity at week 14, they exhibited radiographic progression by week 54 (fig 2). Consistent with previous observations,15 joint damage increased with disease activity categories, reflecting increasing disease activity.

{kind=link}
{kind=link}
Changes in total Sharp score from baseline to week 54 by disease activity, as classified by the simplified disease activity index, at weeks 14 and 54. MTX, methotrexate; TSS, total Sharp score.
In contrast to methotrexate monotherapy, patients treated with methotrexate plus infliximab who reached remission or a low level of disease activity by week 14 or week 54 had no further radiographic progression by one year, whereas patients who had high disease activity at weeks 14 or 54 experienced some progression of radiographic changes (fig 2). However, when compared with patients who received methotrexate plus placebo, those treated with methotrexate plus infliximab who still had high levels of disease activity exhibited significantly less progression of joint damage (fig 2). Nevertheless, even in the infliximab plus methotrexate arm, progression of joint damage was related to disease activity, although the slope of progression was deflected when compared with methotrexate monotherapy. The differences in radiographic progression between the methotrexate plus placebo and methotrexate plus infliximab arms were not caused by differences in disease activity within each of the respective disease activity categories. For example, at week 14, patients in the low disease activity category receiving methotrexate plus placebo had a mean (SD) SDAI of 7.7 (2.6), whereas patients receiving methotrexate plus infliximab with low disease activity exhibited a mean SDAI of 7.4 (SD 2.2, p = NS). Within the remission, moderate disease activity and high disease activity categories, the respective SDAI values were 2.1 (SD 0.6) and 1.9 (SD 0.9), 18.1 (SD 4.4) and 17.9 (SD 4.1) and 39.3 (SD 8.6) and 39.9 (SD 10.8), respectively.
DISCUSSION
Utilising data from the ASPIRE trial,3 we explored the association between radiographic progression and disease activity, as assessed by composite indices rather than individual predictors, following treatment with methotrexate plus placebo or methotrexate plus infliximab in RA patients. The results of these analyses demonstrated that among the patients receiving methotrexate monotherapy, the level of disease activity during treatment was highly associated with joint damage at week 54. Patients who were in remission in terms of disease activity at an early time point, ie, at week 14, demonstrated virtually no progression of joint damage, whereas joint damage was observed across all other levels of active disease (low, moderate and high) at weeks 14 or 54, as well as in patients achieving remission at a later stage of treatment (week 54). Therefore, achieving remission rapidly on traditional DMARD such as methotrexate may completely protect patients from progression of joint damage. However, even if only a low level of disease activity is achieved and not remission, joint damage ensues, consistent with observations on the strong correlation of time-averaged disease activity and joint damage.8 16 17
The addition of a TNF inhibitor such as infliximab to traditional DMARD therapy with methotrexate, in line with previous experience,3 18 19 was superior to treatment with methotrexate alone, not only in controlling disease activity as assessed by the achievement of remission or low disease activity, but also in preventing joint damage. These results were observed across all levels of disease activity, even in patients who maintained a high level of disease activity throughout the study, and are in line with previous findings on the dissociation of the direct and strong relationship between active inflammation and joint damage.20 21 Nevertheless, even though the degree of radiographic progression was dramatically reduced by treatment with methotrexate plus infliximab, patients with a high level of disease activity did have a residual amount of progression when compared with patients having low or moderate levels of disease activity. This finding provides evidence that the correlation between disease activity and joint damage is not totally disconnected by TNF inhibition, but in relation to the degree of disease activity, only dissociated or deflected from the more natural course. The slope of progression is thus considerably shifted and smaller compared with methotrexate monotherapy, and radiographic damage is virtually halted in disease activity states, especially low disease activity, in which methotrexate monotherapy cannot prevent the accumulation of joint destruction.
Importantly, however, whereas with regard to DMARD monotherapy the observations herein are consistent with previous studies on the natural history of RA and the results of clinical trials correlating disease activity with radiographic progression of joint damage,20–23 achieving remission with methotrexate early is associated with an arrest or at least profound reduction of joint damage progression. Therefore, the current study introduces the aspect of time into our assessments of response to therapy. With methotrexate monotherapy, on the group level, progression of joint damage was only completely halted between baseline and week 54 if patients achieved remission within the short term, ie, week 14.
Clinical analyses recently suggested that disease activity at 3 months after the start of therapy was highly predictive of disease activity at one year.24 The present data pertaining to joint destruction, in conjunction with the aforementioned clinical data, indicate that for patients receiving methotrexate (and probably other traditional DMARD) the achievement of, at the very least, low disease activity and, ideally, remission within a few months of starting treatment should be a major therapeutic goal. If this aim is not attained within a short time frame, treatment would need to be modified to prevent the progression of joint damage and, consequently, the accrual of irreversible disability.6 This stands in stark contrast to the arrest or minimisation of radiographic progression observed at low and even moderate levels of disease activity, both early and late in the treatment of RA patients, with infliximab in combination with methotrexate. This result was obtained despite the similar SDAI values observed in the respective disease activity categories in both treatment groups, further supporting the concept of a dissociation, or at least a reduction of the association, between disease activity and joint damage by TNF inhibitor plus methotrexate therapy.20
The major limitation of our study is the nature of the post-hoc analysis. Therefore, our findings primarily serve as hypothesis generating and confirmation of the results will be required from prospective trials. Moreover, the trial was not designed to assess whether therapy could be reduced or even halted once remission is achieved. Although a trial investigating such options would be desirable, it should be borne in mind that stopping therapy in patients, even in those with prolonged remission, has been shown to result in increases in disease flares and difficulties in regaining a state of remission.25 26
In summary, combination therapy with methotrexate plus infliximab inhibits radiographic progression across all disease activity states, with no or only minimal progression even with low and moderate levels of disease activity. In contrast, therapy with traditional DMARD such as methotrexate can lead to the progression of joint damage, even at low and moderate disease activity levels; however, when remission is achieved early in the course of DMARD therapy, progression can be halted.
Acknowledgments
The authors wish to thank Michelle Perate and Mary Whitman (Centocor, Inc) for writing support.
REFERENCES
Footnotes
Competing interests: EWSC received grant support from Amgen. He is a consultant for Genentech, Bristol-Meyers Squibb, Novartis, Synovex, Biogen Idec and Medimmune. CH owns Johnson & Johnson stocks. JMB has research contracts with Amgen, Bristol Myers Squibb and IDEC-Biogen. PE has provided expert advice and undertaken clinical trials for Centocor/Schering-Plough, Amgen, Abbott and UCB. EK was funded by Abbott Laboratories, Amgen Inc, AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb Company, Centocor, Inc, F Hoffmann-LaRoche Inc, Novartis Pharmaceuticals Corp, Schering-Plough Corporation, UCB and Wyeth Pharmaceuticals and is a consultant for Abbott Laboratories, Amgen Inc, Bristol-Myers Squibb Company, Centocor, Inc, Chelsea Therapeutics, Inc, CombinatoRx Inc, F Hoffmann-La Roche Inc, Genentech, Inc, GlaxoSmithKline, Medarex, Inc, Schering-Plough Corporation, UCB and Wyeth Pharmaceuticals. DMFMH has received consultancy fees and/or research grants from Abbott, Amgen, BMS, Centocor, Chugai, Roche, Schering Plough and UCB. RNM has had consultancies/advisory boards with Abbott Laboratories, Arana (formerly Peptech), AstraZeneca, Boehringer Ingelheim Ltd, Centocor Inc, Domantis, Evotec, F-star, GlaxoSmithKline, Nicholas Piramal India Ltd, Roche, Schering-Plough and UCB/Celltech in the past 5 years. The inventor’s shares of royalties are received by Kennedy Institute of Rheumatology Trust from Centocor and Abbott. JRK has served on advisory boards of Abbott, Wyeth, Centocor, Pfizer and Merck. JSS received grant support from Abbott, Roche, UCB, Schering-Plough, Wyeth and honoraria from Abbott, Amgen, Astra-Zeneca, BMS, Centocor, Novartis, Roche, Schering-Plough, UCB, Wyeth.
Funding: This research was supported by Centocor, Inc, Malvern, PA, a subsidiary of Johnson & Johnson.
Ethics approval: The protocol was approved by an institutional review board at each study centre and carried out according to the Helsinki Declaration of 1975, as revised in 1983 and 1989.
Patient consent: Obtained.
Linked Articles
- Miscellaneous