Article Text

Abstract
Objective: We undertook an observational study to obtain a complete overview of the long-term effectiveness and safety of etanercept in patients with different juvenile idiopathic arthritis (JIA) subtypes.
Methods: At baseline we collected patient and disease characteristics of all Dutch patients with JIA who started treatment with etanercept. Disease activity was evaluated (at start of the study, after 3 months and then yearly) according to the JIA core set of the American College of Rheumatology paediatric definition for 30, 50 and 70% improvement (ACR Pedi 30, 50 and 70). Use of etanercept and concomitant drugs was monitored. Adverse events were recorded.
Results: We included 146 patients with JIA with a median follow-up of 2.5 years per patient (range 0.3–7.3). JIA subtypes represented: 27% systemic, 8% polyarticular rheumatoid factor positive, 38% polyarticular rheumatoid factor negative, 19% oligoarticular extended, 3% enthesitis-related and 5% psoriatica. Most patients (77%) met the criteria of the ACR Pedi 30 in the first 3 months of treatment. For the majority of patients this improvement was sustained; 53 (36%) of all patients met the remission criteria. No other second-line agents were needed in 43 patients. Although patients with systemic JIA responded initially less to etanercept therapy than patients from other subtypes, those who did respond showed equal effectiveness in the long term. Serious adverse events rate was low (0.029 per patient year).
Conclusions: Etanercept is effective and safe in JIA, even for a large proportion of the patients with systemic JIA. The greatest improvement occurred in the first 3 months of treatment, and was sustained for a long time in most patients (up to 75 months).
Statistics from Altmetric.com
In recent years, tumour necrosis factor (TNF)-α blocking medication has become a treatment option in juvenile idiopathic arthritis (JIA).1 2 Etanercept is currently the most frequently prescribed TNF-α blocking medicine in polyarticular JIA. It binds to TNF-α and TNF-β (lymphotoxin-α), preventing it from interacting with the receptors on the cell surfaces.3 4
Lovell et al first reported on etanercept in 69 patients with JIA in a controlled clinical trial.5 These patients were thereafter followed in an open label extension study, and efficacy and safety of etanercept were shown over a period of 4 years. However, the disease course was not described in detail for all different JIA subtypes.6 7 Several other open label studies produced good initial effectiveness of etanercept; however, they either involved small patient groups or they took no account of the difference in onset subtype.8–12 Horneff et al were the first to describe a registry on etanercept in JIA, including 322 patients; 84% were included in the evaluation of effectiveness, with a maximum follow-up of 4 years.13
To obtain a complete overview of the long-term effectiveness and safety of etanercept in relation to the different onset subtypes, we performed a long-term study in all patients with JIA who started treatment with etanercept in The Netherlands.
PATIENTS AND METHODS
Subjects
In The Netherlands, patients with JIA are eligible for treatment with etanercept if the condition has a polyarticular-course and the response to the maximum or maximum tolerated dose of methotrexate (MTX) proved to be insufficient. When TNF-α blocking medication was included in the Medications Reimbursement System by the Ministry of Health, Welfare and Sport, a central evaluation board was installed to evaluate each patient. All Dutch patients younger than 18 years with JIA of different subtypes, in whom etanercept use was granted by the evaluation board from 1999 until 2006, were included in our register. The database from the central evaluation board, that had to approve etanercept treatment for each individual Dutch patient, was used to insure completeness. The study was financed by the Board of Health Insurances.
Study design
This prospective, ongoing, multi-centre observational study is coordinated by Erasmus MC Sophia Children’s Hospital. The protocol was approved by the Medical Ethical Committee of Erasmus MC, Rotterdam. Written informed consent was obtained, and the study was conducted in accordance with the Declaration of Helsinki.
The following data were collected at baseline: patient and disease characteristics, including gender, age at onset, age at start etanercept, disease duration, JIA subtype, medical history, previous medication, concomitant drugs at start etanercept, starting dose of etanercept and disease activity. Follow-up data (disease activity, observed adverse events, etanercept dose and concomitant drug use) were collected at 3 months (at the same time every patient was re-evaluated by the central evaluation board) and every year thereafter. There were no limitations in the use of concomitant drugs. If etanercept was withdrawn, the reason for withdrawal was reported.
The outcome measures used to assess disease activity consisted of following six response variables of the JIA core set: (1) overall assessment of disease activity by the doctor through the visual analogue scale (VAS) (range 0–100 mm); (2) childhood health assessment questionnaire (CHAQ) (range 0–3) by the patient; (3) overall assessment of well-being by the patient through the VAS (range 0-100 mm); (4) number of active joints (joints with swelling not caused by deformity, or joints with limited motion, and with pain, tenderness, or both); (5) number of joints with limited motion; and (6) a laboratory marker of inflammation, erythrocyte sedimentation rate (ESR).14
Effectiveness analysis
Effectiveness was assessed using the American College of Rheumatology paediatric 30, 50 and 70 criteria (ACR Pedi 30, 50 and 70).14 This definition states that there should be at least 30% improvement (or 50% or 70%, dependent on the score) from baseline in three of any six variables in the JIA core set, with no more than one of the remaining variables worsening by >30%. Patients in whom etanercept was halted within the first 3 months of treatment were marked as initial non-responders. Patients were marked as secondary non-responders if they discontinued etanercept because of a disease flare as judged by the treating doctor.
When patients discontinued etanercept in the event of remission the treatment was considered to be successful. For evaluation purposes we used the criteria by Wallace et al for remission on medication, which had to be met for more than 6 months and are defined as: no active arthritis, no fever, rash, serositis or lymphadenopathy attributable to JIA, no active uveitis, normal ESR and a doctor’s overall assessment of disease activity that indicated no disease activity.15 We defined ESR values under 16 mm/h as normal. We stated that a doctor’s overall assessment score below 20 mm (instead of 0 mm) on the VAS indicated no disease activity.
Safety analysis
All medical important adverse events (AEs) and all serious adverse events (SAEs; defined as events that were life threatening or fatal, or resulted in a disability, handicap, congenital anomaly or birth defect, or required inpatient hospitalisation) were reported by the treating doctors on a continuous base. In addition, the investigators frequently searched for AEs in all patient files to ensure the completeness of data. Flaring of JIA was not recorded as an AE. We calculated the patient year rate of SAEs (for the period that etanercept was used and 30 days after discontinuation) on the base of duration of exposure to etanercept.
Statistical analysis
Baseline characteristics were listed and summarised. Response variables were evaluated according to the ACR Pedi 30, 50 and 70. Missing values (5.1% of the JIA core set response variables) were computed using the aregImpute function by F. Harrell.16 When appropriate the χ2 test and the Mann–Whitney U test were used to compare the responses (using level of significance p<0.05). Adherence to therapy was estimated with Kaplan–Meier plots and differences were defined by the log rank test (significance p<0.05).
Analyses were performed using the SPSS for Windows package, version 14.0.1 (SPSS Inc., Chicago, Illinois, USA), except for imputation of missing values, which was performed with the R package, version 2.4.1 (http://www.r-project.org/).
RESULTS
Patient and disease characteristics
Table 1 shows the patient and disease characteristics and previous JIA therapy of the 146 patients included in the study. All patients were treated in one of the nine centres with experienced paediatric rheumatologists (range 5 to 41 patients per centre). Most patients received etanercept at the usual dose of 0.4 mg/kg twice weekly; in 28 patients etanercept was initiated or changed to a double dose of 0.8 mg/kg once weekly. Median duration of etanercept therapy was 1.7 years (range 0.1 to 6.8 years). Total follow-up time was 436.1 patient years (median of 2.5 years per patient, range 0.3 to 7.3 years). Four patients had a history of uveitis; one of these patients still had an active uveitis at start of etanercept.
Clinical outcomes
Figure 1 shows the flowchart outlining follow-up of all patients. The number of patients who discontinued etanercept for reasons of non-responding, adverse event or complete remission was noted per follow-up period.
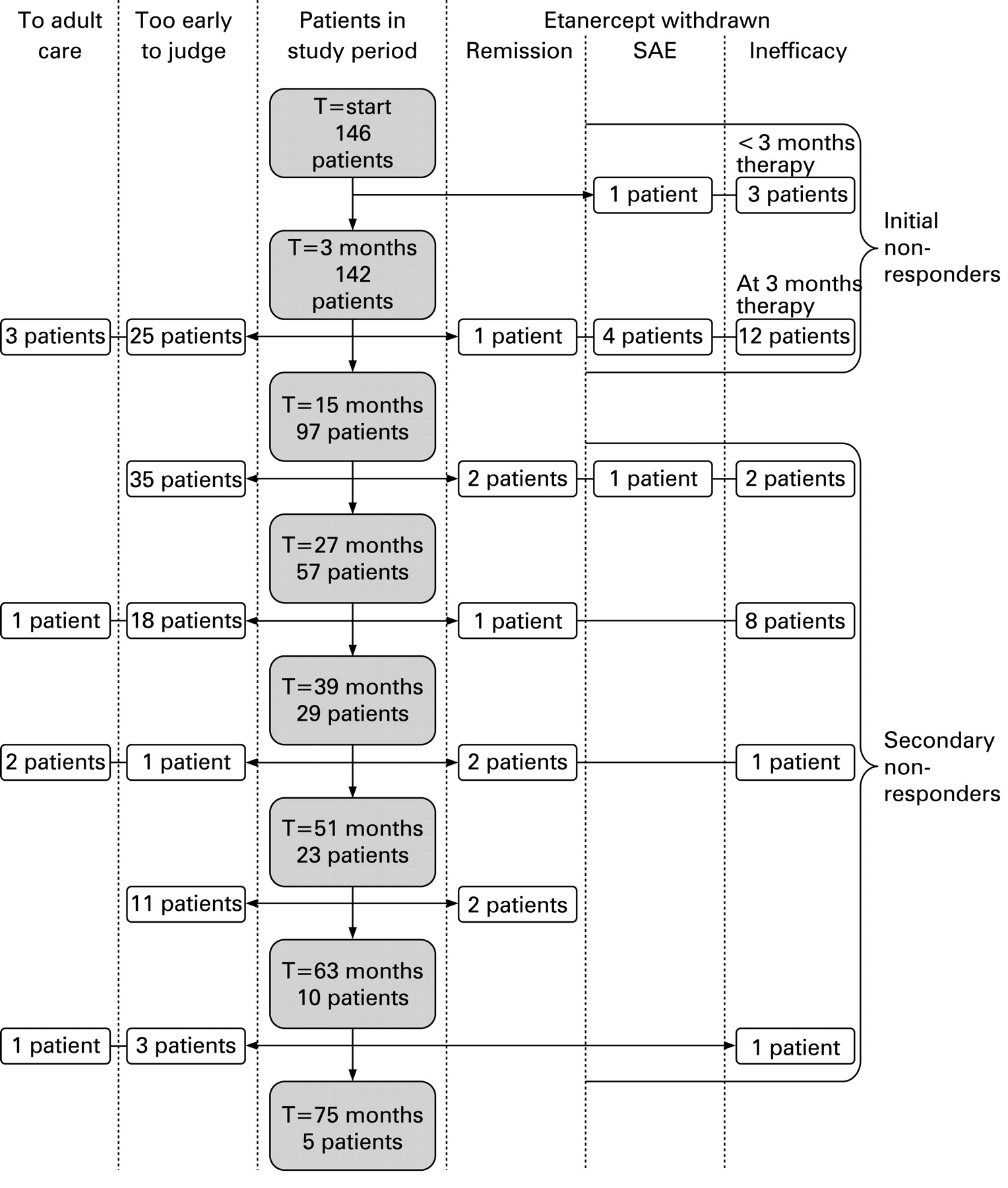
Flowchart of patients in the study using etanercept.
The improvement from baseline and the results of the response variables are shown in table 2. The table contains data from patients who responded to etanercept treatment. Figure 2 shows the number of patients who met the criteria of the ACR Pedi 30, 50 and 70 in relation to the total number of patients according to the intention to treat modus. In general, there was a major improvement for all JIA subtypes in all variables after 3 months of treatment and in the years thereafter. However, the percentage of patients with sustained improvement seems to decline after 27 months. Patients with systemic JIA improved significantly less than other JIA subtypes on the ACR Pedi 30, 50 and 70 scores (p<0.01 for all three scores) in the first 3 months of therapy.

Improvement according to the American College of Rheumatology pediatric (ACR Pedi) score for 30, 50 or 70% improvement in percentage of patients based on the intention to treat modus. The percentage of patients (who could have reached that fixed follow-up moment after start of etanercept treatment) that met the criteria for the ACR Pedi 30, 50 or 70 (all patients, sJIA, non-sJIA) are shown.
During the study period, 53 of all 146 patients met the remission criteria (19 patients had a doctor’s overall assessment score between 0 and 20 mm instead of the strict 0 mm). The percentages of all included patients per subtype, who met those remission criteria were: 38% systemic JIA (sJIA), 32% oligoarticular JIA extended (oJIA ext), 38% polyarticular rheumatoid-factor negative JIA (pJIA RF–), 36% polyarticular rheumatoid-factor positive JIA (pJIA RF+).
Drug withdrawal and survival analysis
Figure 3 shows the Kaplan–Meier analysis of the proportion of patients that continued etanercept on grounds of effectiveness; patients with sJIA are shown separately from other JIA subtypes. This survival analysis indicates that etanercept is more likely to be withdrawn in patients with sJIA on grounds of ineffectiveness than in patients with other JIA subtypes (p<0.001 by log-rank test).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival analysis of etanercept use.
Etanercept therapy was discontinued in 20 initial non-responders and in 13 secondary non-responders (22 sJIA, 1 pJIA RF+, 6 pJIA RF–, 4 oJIA ext). Disease duration at start of etanercept in non-responders compared to responders was neither in total patient group (p = 0.56) nor in the sJIA group (p = 0.38) statistically significantly different. In nine (41%) of the non-responding patients with sJIA flaring of systemic features was observed by the treating doctor after discontinuation of etanercept.
Of the 33 patients who discontinued etanercept, 17 did not switch to another biological. These patients received NSAIDs (88%), MTX (76%), systemic glucocorticoids (65%) and intra-articular glucocorticoids injections (18%) after discontinuation of etanercept. The other 16 patients (14 patients with sJIA and 2 patients with oJIA ext) switched to another biological (6 infliximab, 4 adalimumab and 6 anakinra). Eight did not respond to the other biological either (five infliximab, two adalimumab and one anakinra). One patient started a third biological (anakinra after etanercept and adalimumab), again without improvement.
All patients used at least one concomitant drug at the start of etanercept treatment (table 1). During the first 15 months of etanercept treatment, NSAIDs were discontinued in 37% of all patients who used it at start and glucocorticoids in 67%. Although 22% of all patients using MTX at start discontinued its use during treatment with etanercept, MTX had to be restarted in 8% of those patients. All other DMARDs were discontinued. In total, 43 patients discontinued all other second-line agents besides etanercept.
During the first 15 months therapy 18 patients received one or more intra-articular glucocorticoids injections.
Safety
During 312 patient years of etanercept use, 65 AEs were reported (table 3). The majority of AEs occurred during the first 15 months of treatment (49 during 133 patient years). Additional second-line agents were used by 68% of the patients with non-infectious AEs, 77% of the patients with infectious AEs and 89% of the patients experiencing a SAE. Occurrence of AEs was not statistically significant different (p = 0.25) between the different JIA subtypes.
Serious adverse events (SAEs) occurred in nine patients; the SAE rate was 0.029 per patient year. Etanercept was definitively discontinued in six cases due to SAEs. Three patients continued etanercept despite having a SAE: a patient after colitis caused by Escherichia coli, a patient who experienced convulsions, since a history of epileptic attacks had been reported before the use of etanercept and another patient who developed sarcoidosis. The two patients with an inflammatory bowel disease as well as the two patients with sarcoidosis had no signs of these diseases before the start of etanercept.
None of the patients showed signs of demyelinisation, or malignancies and no new cases of uveitis were reported and none of the patients died on etanercept therapy.
Three patients with systemic JIA who did not respond to etanercept died after multiple immunosuppressive treatments that also failed. One patient who discontinued treatment with etanercept and started treatment with infliximab developed tuberculosis under treatment with infliximab, and died.17 None of the other patients in our study developed tuberculosis. One patient died of a suspected macrophage activation syndrome and another patient died of a suspected sepsis masked by the use of immunosuppressive drugs. All three patients were initial non-responders and had not used etanercept for at least 8 months when they died.
DISCUSSION
This paper presents the results from our prospective open label study in which we consecutively included all patients with JIA in The Netherlands who used etanercept. The data from this Dutch register proved, in a real-life setting with an unselected and complete patient population, the initial but also the sustained effectiveness of etanercept in JIA up to 75 months. This is a promising result considering that the patients in the study had not previously responded to other second-line agents, including the maximum (tolerated) dose of MTX. The greatest improvement took place in the first 3 months. It confirms findings from previous studies, indicating that rapid improvements can be made with etanercept.5 10 13 Further improvements are seen thereafter, although they seem to decline in the long term, but the number of patients are relatively small (table 2 and fig 2). However, considering that some patients had severe disease flaring even though they were previously in remission, we have to conclude that etanercept cannot always completely suppress the activity in all patients with JIA.
Although our study has the longest follow-up period reported in the literature until now, previous studies already reported on this subject. Lovell et al showed sustained benefit of etanercept in JIA in a 4-year open label extension study. However, this study group was relatively small (58 patients) and the patients already proved to be initially responsive to etanercept before entering the extension study.5–7 The German registry on etanercept in JIA by Horneff et al concerned a large study population (322 patients). Of these patients 84% were included in the effectiveness analysis, which may have led to selection bias. They also did not describe the patient and disease characteristics as explicitly as we did.13
In our study we found that early in treatment effectiveness appeared to be depended on the JIA subtype; in the first 3 months of treatment more patients with sJIA were unresponsive or less responsive to etanercept than those with other subtypes. Surprisingly, after 15 months of follow-up patients with sJIA discontinued etanercept treatment about as frequently as patients from other subtypes. The patients with sJIA who responded to etanercept showed the same improvement on the ACR Pedi score after a prolonged time and 38% of all patients with sJIA included even reached remission on medication.
Several other studies have also reported lower rate of responsiveness of patients with sJIA to etanercept. Stated as possible reasons were the severity of disease and other factors such as IL-1 and IL-6 which might play a larger role in patients with sJIA than in other subtypes.18–21 However, in our study a great part of the patients with sJIA was responsive to etanercept. We therefore conclude that it is reasonable to accept etanercept as the first choice in treatment of patients with sJIA as long as no new treatments are available. Anakinra is reported to be effective with different response rates in sJIA.21–23 In our study, five out of seven patients with sJIA unresponsive to etanercept did respond to anakinra. Therefore, at the moment we suggest anakinra to be the next best choice of treatment for those patients with sJIA who do not respond to etanercept, which in most cases can be concluded after 3 months of treatment.
Although etanercept does not induce remission in all patients, it seems to suppress disease activity in patients with refractory JIA. The fact that 41% of the patients with sJIA who discontinued etanercept due to persistent active arthritis developed systemic features suggests that etanercept did have some effect.
Our study shows that doctors generally have the same therapy strategies in patients based on the response. The first strategy is to be cautious when changing treatment in patients who respond well to etanercept. In these patients, doctors often reduce concomitant medication but act with great caution regarding etanercept treatment, leading to continuation for many years for patients in complete remission. Until now, no studies on how or when to stop etanercept in patients with JIA in remission have been published.
The other strategy applies to the patients in whom disease activity fails to decline on etanercept; doctors are likely to treat these patients more aggressive and raise the dose and concomitant medication. If this fails etanercept is stopped and other therapy options are considered. Our results suggest not continuing etanercept for more than 15 months in non-responders, since not much improvement is expected after that.
Some of the patients in this study received etanercept in the double dose of 0.8 mg/kg once weekly. Although there are no reports on controlled clinical trials investigating the double weekly dose in patients with JIA, data from two clinical studies show no differences in effectiveness or safety compared to the usual dose.24 25
In accordance with previous studies on the safety of etanercept our long-term follow-up study reports few AEs and a low SAE-rate.5–10 13 None of the patients developed tuberculosis during etanercept treatment. Additionally, other studies state that the incidence of tuberculosis is lower during etanercept treatment than during infliximab therapy.8 26 However, two patients developed another granulomatous disease: sarcoidosis. To our knowledge, these are the first cases of sarcoidosis during etanercept therapy to be reported. Two patients developed a chronic inflammatory bowel disease (IBD) during etanercept therapy. Although several others cases of new onset IBD during etanercept use were reported anti-TNF-α therapy (mostly infliximab but also etanercept) is described in the literature as IBD treatment.10 13 27–31 This is contradictive and the mechanism behind it is still unknown. More research is required in this field.
It has to be taken into account that this was an observational study; only the clinically relevant AEs were reported by the doctors. This might have led to some underreporting compared to controlled clinical trials.
In conclusion, while this study confirms earlier findings that etanercept is effective and safe in JIA, it also shows that initial effectiveness varies in the subtypes of JIA. Overall, patients with sJIA improve significantly less in the first months of therapy. However, those patients with sJIA who do respond to etanercept therapy show levels of improvement comparable to those of patients with other JIA subtypes. Although some unexpected SAEs occurred, etanercept was safe in JIA.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: The protocol was approved by the Medical Ethical Committee of Erasmus MC, Rotterdam. Written informed consent was obtained, and the study was conducted in accordance with the Declaration of Helsinki.