Article Text

Abstract
Objective: To investigate differences in clinical signs and symptoms, and in antinuclear antibodies (ANA), between patients with juvenile-onset and adult-onset systemic lupus erythematosus (SLE).
Methods: Clinical and serological data of 56 patients with juvenile-onset SLE were compared with data of 194 patients with adult-onset SLE. ANA were determined by line immunoassay and by indirect immunofluorescence on Crithidia luciliae.
Results: Renal involvement, encephalopathy and haemolytic anaemia were seen, and anti-dsDNA, anti-ribosomal P and antihistone antibodies found, significantly more often in juvenile-onset SLE. Anti-dsDNA antibodies were directly associated, and anti-ribosomal P antibodies inversely associated, with renal involvement in juvenile-onset SLE. In juvenile patients with SLE and anti-dsDNA and without anti-ribosomal P antibodies the odds ratio for glomerulonephritis was 9.00; no patients with anti-ribosomal P but without anti-dsDNA had renal involvement.
Conclusion: Patients with juvenile-onset SLE more often have renal involvement and encephalopathy than patients with adult-onset SLE. Anti-ribosomal P, anti-dsDNA and antihistone antibodies are more often found in patients with juvenile-onset SLE.
Statistics from Altmetric.com
Many studies have been published highlighting the clinical and serological characteristics of systemic lupus erythematosus (SLE) in adults. Autoantibodies, notably antinuclear antibodies (ANA), are important both in the diagnosis and pathophysiology of SLE. Some antibodies are highly specific for SLE and some are associated with clinical symptoms.1 2 The incidence of juvenile SLE is very low (less than 1/100 000), which makes it hard to gather a substantial study group. Several studies have demonstrated that renal disease is more common in children.2–5 In contrast, for other symptoms and autoantibodies few differences have been found and confirmed. One study reported the higher prevalence of anti-ribosomal P antibodies in juvenile-onset SLE compared with adult-onset SLE.6 Other studies found a higher prevalence of anti-dsDNA,5 7 anti-RNP7 and anti-Sm antibodies7 in juvenile-onset SLE.
We report the prevalence of different signs, symptoms and antibodies in juvenile-onset SLE, compared with an adult-onset population. Associations between antibodies and clinical features were assessed.
PATIENTS AND METHODS
Patients
All the patients met four or more of the revised American College of Rheumatology (ACR) classification criteria for SLE.8 9 Juvenile onset was defined as diagnosis at the age of 18 or younger according to the Paediatric Rheumatology International Trials Organization (PRINTO).10 Fifty-six patients with juvenile-onset SLE and 194 patients with adult-onset SLE were studied. Several centres participated: University Hospital Ghent, Belgium; University Hospital Leiden, the Netherlands; Research Institute of Rheumatic Diseases Piestany, Slovakia; University College London, UK; Université Catholique de Louvain, Belgium; and University Hospital Brussels, Belgium. All centres are tertiary referral centres.
Clinical data
A questionnaire covering clinical data was completed by the treating doctor, based on history taking and on the patient’s medical chart (table 1). Symptoms occurring during the entire disease course were considered.
The study was conducted after approval by the local ethics committees. Informed consent was obtained from all patients.
Determination of autoantibodies
Serum samples were analysed by line immunoassay (INNO-LIA ANA update, K1090, Innogenetics, Zwijnaarde, Belgium) as described previously.11 This multiparameter assay contains the following antigens: SmB, SmD, RNP-A, RNP-C, RNP-70k, Ro52, Ro60, La/SSB, Cenp-B, Topo-I, Jo-1, ribosomal P and histones.11
Anti-dsDNA antibodies were detected by indirect immunofluorescence (IIF) on Crithidiae luciliae.
Statistical analysis
Statistical analysis was performed using SPSS, version 15.0.
To determine associations a χ2 test or the Fisher exact test was used. We computed odds ratios (ORs) and their 95% confidence interval (95% CI). No correction for multiple testing was made. For comparing medians, the Mann–Whitney U test was used.
RESULTS
Demography
In the adult group, 23 (11.9%) of the patients were male, versus nine (16.1%) in the juvenile group (NS). Median age at diagnosis was 32 years for adults (range 19–73) and 15 years for juvenile patients (range 9–18). Median age at sampling was 41 years (range 20–77) in adults and 20 years (range 12–49) in juvenile patients. Median symptom duration at sampling was 5 years for adults and 5.5 years for juvenile patients (NS). In the juvenile group 44/55 (80.0%) were Caucasian (data missing for one patient), compared with 161/188 (85.6%) in the adult group (NS) (data missing for six patients).
Distribution of symptoms
The prevalence of symptoms in both groups was calculated (table 1). Among cutaneous symptoms, significant differences were found for generalised erythema, OR = 2.38 (95% CI 1.05 to 5.39), subacute cutaneous lupus, OR = 4.65 (1.20 to 18.02) and chilblains OR = 9.22 (1.73 to 49.00), which were all seen more often in juvenile patients. Fever occurred significantly more often in juvenile SLE, OR = 1.97 (1.05 to 3.70), whereas sicca symptoms and arthralgia were less common. Renal signs occurred markedly more often in juvenile patients (proteinuria: OR = 2.30 (1.23 to 4.28); glomerulonephritis: OR = 2.96 (1.60 to 5.49); urinary cellular casts, OR = 2.83 (1.48 to 5.40)). This was also the case for encephalopathy (OR = 4.55 (1.82 to 11.41)) and haemolytic anaemia (OR = 4.19 (2.07 to 8.48)).
Prevalence of autoantibodies
Table 2 shows the prevalence of autoantibodies. Anti-ribosomal P (p⩽0,01), anti-dsDNA (p⩽0.001) and antihistone antibodies (p⩽0.05) were found significantly more often in the juvenile patients. When we computed the total number of reactivities for each patient we found a higher number of reactivities in the patients with juvenile-onset SLE than in adult-onset SLE (mean 1.9 vs 1.4; p⩽0.05).
Associations of autoantibodies with clinical signs
The most striking findings are the association of anti-dsDNA antibodies with renal signs and the inverse association of anti-ribosomal P with renal signs in juvenile SLE. Anti-dsDNA antibodies were significantly associated with glomerulonephritis, p⩽0.01; OR = 2.41 (1.25 to 4.64) and with urinary cellular casts p⩽0.05; OR = 3.33 (1.01 to 10.97). The association of anti-dsDNA and proteinuria was not significant p = 0.086; OR = 2.67 (0.86 to 8.29). In contrast, anti-ribosomal P antibodies were inversely associated with glomerulonephritis, p⩽0.05; OR = 0.22 (0.06 to 0.80), with urinary cellular casts p⩽0.01; OR = 0.61 (0.04 to 0.70) and with proteinuria, p⩽0.05; OR = 0.20 (0.07 to 0.74).
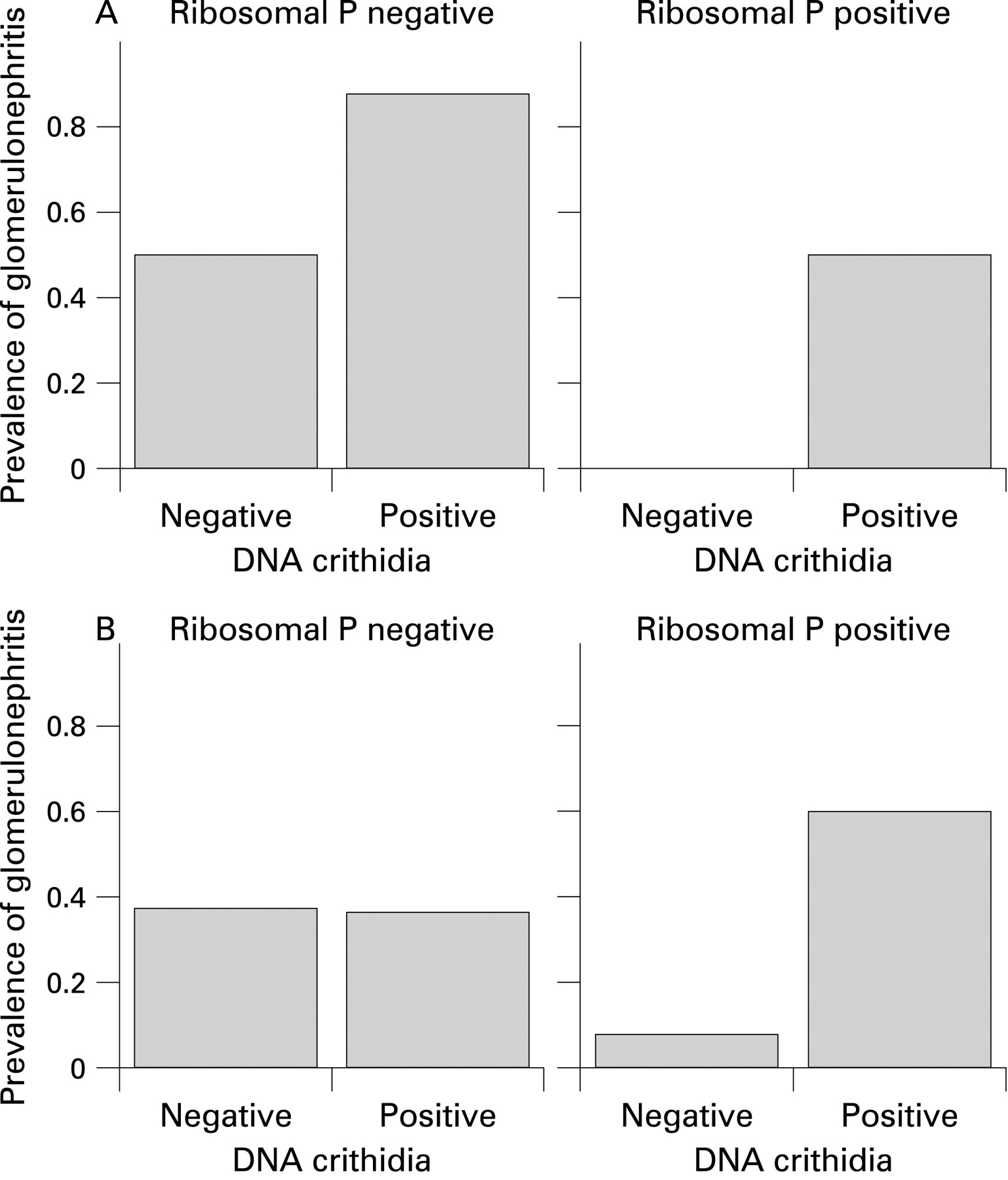
We divided the patients according to their anti-dsDNA and anti-ribosomal P status in order to clarify these results. The presence or absence of both antibodies in the same patient was not associated with renal signs. However, if anti-dsDNA antibodies were present and anti-ribosomal P antibodies were absent (n = 23) a strong association with renal involvement was found: OR for glomerulonephritis = 9.00 (2.23 to 36.33), p⩽0.001; for urinary cellular casts OR = 6.57 (1.74 to 24.77), p⩽0.005; and for proteinuria OR = 4.75 (1.32 to 17.11). In four patients anti-ribosomal P antibodies were present and anti-dsDNA antibodies were absent, none of them had renal involvement (all p<0.05).
In the adult population we could not find any significant associations for patients positive for both antibodies or negative for both antibodies. Moreover, no significant associations were found for the anti-dsDNA positive and anti-ribosomal P negative group (n = 41). Fifteen adult patients had anti-ribosomal P antibodies without anti-dsDNA antibodies, only one of these had proteinuria and glomerulonephritis, none had cellular casts (all p<0.05). Figure 1 shows the occurrence of glomerulonephritis according to antibody status.
{kind=link}
DISCUSSION
We studied the occurrence of signs and symptoms of SLE and ANA in patients with a diagnosis before the age of 18 as compared with patients with adult-onset SLE. We searched for associations between autoantibodies and clinical symptoms in juvenile SLE. It has been suggested that juvenile SLE has a more serious disease course than adult SLE.12 13 A higher occurrence of renal disease, resulting in more renal damage has, notably, been reported.14 We confirm the more frequent occurrence of renal disease in juvenile SLE that has been described previously.2–5 Furthermore, we found a higher frequency of fever, generalised erythema, chilblains, subacute cutaneous lupus, encephalopathy and haemolytic anaemia in juvenile SLE. The higher prevalence of renal, neurological and haematological symptoms points to a more severe disease in juvenile SLE than in adult SLE.
Techniques for detecting ANA have changed markedly over the past 10 years, making it hard to interpret earlier results about the prevalence of antibodies. For detecting antibodies towards Sm, RNP, Ro/SSA, La/SSB, ribosomal P and histones, we used the sensitive and specific line immunoassay technique.11 For detecting anti-dsDNA antibodies we used IIF on Crithidia luciliae, which is very specific for SLE. It was previously reported that anti-ribosomal P6 and anti-dsDNA antibodies5 7 are more common in juvenile SLE. We confirmed this and also found a higher occurrence of antihistone antibodies. Reichlin et al stated that both anti-dsDNA and anti-ribosomal P antibodies were associated with a higher prevalence of renal involvement in juvenile SLE.6 Since these antibodies are more common in juvenile SLE this may explain the higher prevalence of renal disease. However, this was not found in an earlier study focusing on ribosomal P antibodies in juvenile SLE.15 Moreover, our results indicate an inverse association between anti-ribosomal P antibodies and renal disease in juvenile SLE, whereas anti-dsDNA antibodies are associated with a higher occurrence of renal disease. We investigated this in more detail, looking at the different possible combinations of these antibodies. This has not yet been done before. Surprisingly, we found very strong associations between renal involvement and some combinations of antibodies. Patients with anti-dsDNA antibodies who did not have anti-ribosomal P antibodies had a high OR for renal involvement, whereas none of the patients with anti-ribosomal P antibodies without anti-dsDNA antibodies had renal disease. Even though the patient numbers are small, the results are statistically significant and the size of the odds ratio points to their clinical relevance.
To confirm these findings, the associations between these antibody combinations and renal symptoms should be investigated in different cohorts. Ideally, prospective cohort studies should be performed, which would also allow the timing of the appearance of antibodies and of renal disease to be investigated. In addition as our cohort is mainly of Caucasian origin, these results need to be confirmed in patients with different ethnic backgrounds. So far, the emphasis has been put on individual antibodies rather than on combinations of autoantibodies as reported here, which underlines the novelty of our findings. Moreover, the age at onset of SLE seems to have an influence on the occurrence of symptoms and autoantibodies as well as on the associations between antibodies and clinical symptoms.
In conclusion, we confirm that juvenile SLE may have a more severe disease course than adult SLE. We show a higher prevalence of anti-dsDNA, anti-ribosomal P and antihistone antibodies in juvenile SLE. In juvenile SLE we find a differential effect of anti-ribosomal P and anti-dsDNA antibodies on renal involvement.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Approved by the local ethics committees.