Article Text

Abstract
Objectives: Few studies have addressed the natural course of, or prognostic factors for the salivary and lacrimal function in primary Sjögren syndrome (SS). Except for the early stages, glandular function has been seemingly stable, and SS A antigen (SSA) seropositivity and hypocomplementemia may predict a decline in the van Bijsterveld score. The aim of the present study was to assess the natural course of the exocrine function in a larger cohort based on the American–European consensus criteria for SS, and to address possible predictive factors for a declining exocrine function.
Methods: We performed a retrospective cohort study. A total of 141 patients were investigated with the Schirmer I test and unstimulated whole saliva (UWS). Historical data regarding these tests and focus score were collected from the files of 111 patients. Median time from diagnosis to follow-up investigation was 5.0 years.
Results: Median UWS was unchanged during follow-up. Median Schirmer I test improved from 5.0 to 7.0 mm/5 min (p<0.05). Present Schirmer I test was associated with historical high IgG and IgA, positive SSA and SS B antigen (SSB) tests and high focus score, and present UWS with historical low C3/C4. Logistic regression identified high focus scores (odds ratio (OR) = 1.343), and low UWS (OR = 0.692) as factors predicting a 30% or more worsening of the Schirmer I test. High focus scores (OR = 1.488) predicted a 30% or more worsening of the UWS.
Conclusion: We confirmed previous studies showing a stable or slightly improved exocrine function over time. High focus scores and low UWS were identified as independent predictors of a worsened exocrine function.
Statistics from Altmetric.com
Primary Sjögren syndrome (SS) has a prevalence of about 0.6%1 and is thus the most common systemic autoimmune rheumatic disease. The principal manifestations are symptoms of dry eyes and dry mouth, and findings of a reduced lacrimal and salivary function. Few studies have addressed the natural course of, or prognostic factors for the exocrine function and other manifestations in SS.
Four previous studies found a stable lacrimal and salivary gland function2–5 (table 1). A recent study found decreasing stimulated gland specific saliva in early SS.6 Only one previous study looked for possible predictive factors for the exocrine function in SS: In a group of 47 patients followed for 5 years, Theander et al7 found no change in the Schirmer test or unstimulated whole saliva (UWS), but a small worsening of the Van Bijsterveld score. SS A antigen (SSA) positivity and low levels of C3 and C4 predicted further decline in the Van Bijsterveld score. These studies were relatively small. Theander et al were the first to report a predictive value of laboratory tests for exocrine function in primary SS.
The aim of the present study was to assess the natural course of the exocrine function in a larger patient population based on the latest American–European consensus criteria (AECC) for SS,8 and to address possible predictive factors for the exocrine function.
PATIENTS AND METHODS
Patients were recruited from the outpatient registry of the Department of Rheumatology, Haukeland University Hospital, Bergen, Norway. Records of all patients registered with the ICD-10 code for primary Sjögren syndrome (M35.0) from 1 January 1999 to 31 January 2005 were assessed, and those fulfilling the AECC criteria who were less than 75 years of age (n = 169) were invited to participate in the study. Altogether, 141 patients consented to a new clinical and laboratory investigation, which was performed over the period May 2004 to April 2005. These investigations included Schirmer I test as a measurement of the lacrimal function and unstimulated whole saliva (UWS),8 in addition to subjective assessments of dry eyes and dry mouth over the previous week on a 100 mm visual analogue scale (VAS), and standard haematological and immunological tests including antinuclear antibodies (ANA), rheumatoid factor (RF), anti-SSA and anti-SS B antigen (SSB) antibodies, and immunoglobulins. The laboratory tests were performed at the regular hospital laboratory.
Time of diagnosis, biopsy of the minor salivary glands, and previous measures of Schirmer I test, UWS, ANA, SSA, SSB, IgG, IgA, IgM, C3 and C4 were obtained from the medical records. The analytical method used for ANA had changed during the study period. An indirect immunoperoxidase technique had been used formerly, and a titre of ⩾128 was regarded as a positive test. For the newer ELISA test we used a cut-off level of 1.00 for a positive result.9 With very few exceptions these investigations had been performed within 1 year of the time of diagnosis. The study was approved by the Regional Committee for Medical Research Ethics, and all patients provided written informed consent before inclusion.
Variables were frequently not normally distributed and non-parametric statistical methods were used. The median and quartiles were used as estimates of central tendency and dispersion. Differences between groups were assessed by the Mann–Whitney U test, or the Wilcoxon signed rank test for paired variables. Associations between variables were analysed with Spearman correlation, or χ2 for dichotomous variables. In concordance with Theander et al,7 patients were classified according to whether the Schirmer I test or UWS had decreased by 30% or more. Multiple logistic regression was then used to study potential baseline risk factors for a reduced exocrine function. A stepward, forward algorithm was used to select factors for the multivariate models, and the odds ratio (OR) and 95% confidence interval (95% CI) were computed for any significant associations. The statistical analyses were performed using SPSS 13.0 (SPSS Inc., Chicago, Illinois, USA).
RESULTS
Demographics
Altogether 141 patients were included. Median age was 57 (49.5–65.0) years, 134 (95%) were women, and 134 (95%) were of Norwegian ethnic (Caucasian) origin. The median time since diagnosis of SS was 5.0 (3.0–9.0) years. A biopsy of the minor salivary glands had been performed in 121 patients, 103 of these (85.1%) were positive (focus score ⩾1). The most frequent other conditions (present or formerly) were diseases related to the thyroid gland (32%). A total of 25 patients (17.7%) used antimalarials, 5 (3.5%) other disease-modifying antirheumatic drugs, 50 (35.5%) non-steroidal anti-inflammatory drugs (daily or intercurrently), and 11 (7.8%) oral steroids. Concerning xerogenic medications, none were taking anticholinergic drugs on a regular basis. In all, 17 patients (12.1%) were rheumatoid factor positive, 107 (75.9%) ANA positive, 86 (61.0%) had anti-SSA antibodies, and 55 (39.0%) anti-SSB antibodies. During follow-up, 33 (23.4%) patients seroconverted to a positive ANA, 5 (3.5%) to a positive RF, and 15 (10.6%) to a positive SSA and/or SSB.
Cross-sectional associations at follow-up
Several of the SS disease measures correlated well with each other in cross-sectional analyses at follow-up, notably Schirmer I test with UWS, ANA and IgG, and UWS with age, dry mouth in last week (VAS) and IgG (table 2). The Schirmer I test was lower in patients with a positive anti-SSA (median 8.50 for SSA negative vs 6.75 for SSA positive, p = 0.03) and anti-SSB (median 8.75 for SSB negative vs 4.50 for SSB positive, p<0.01). Although a similar trend was noted for UWS (median 1.60 vs 1.50 for SSA positive and 1.60 vs 1.40 for SSB positive), these results were not significant.
Exocrine function over time
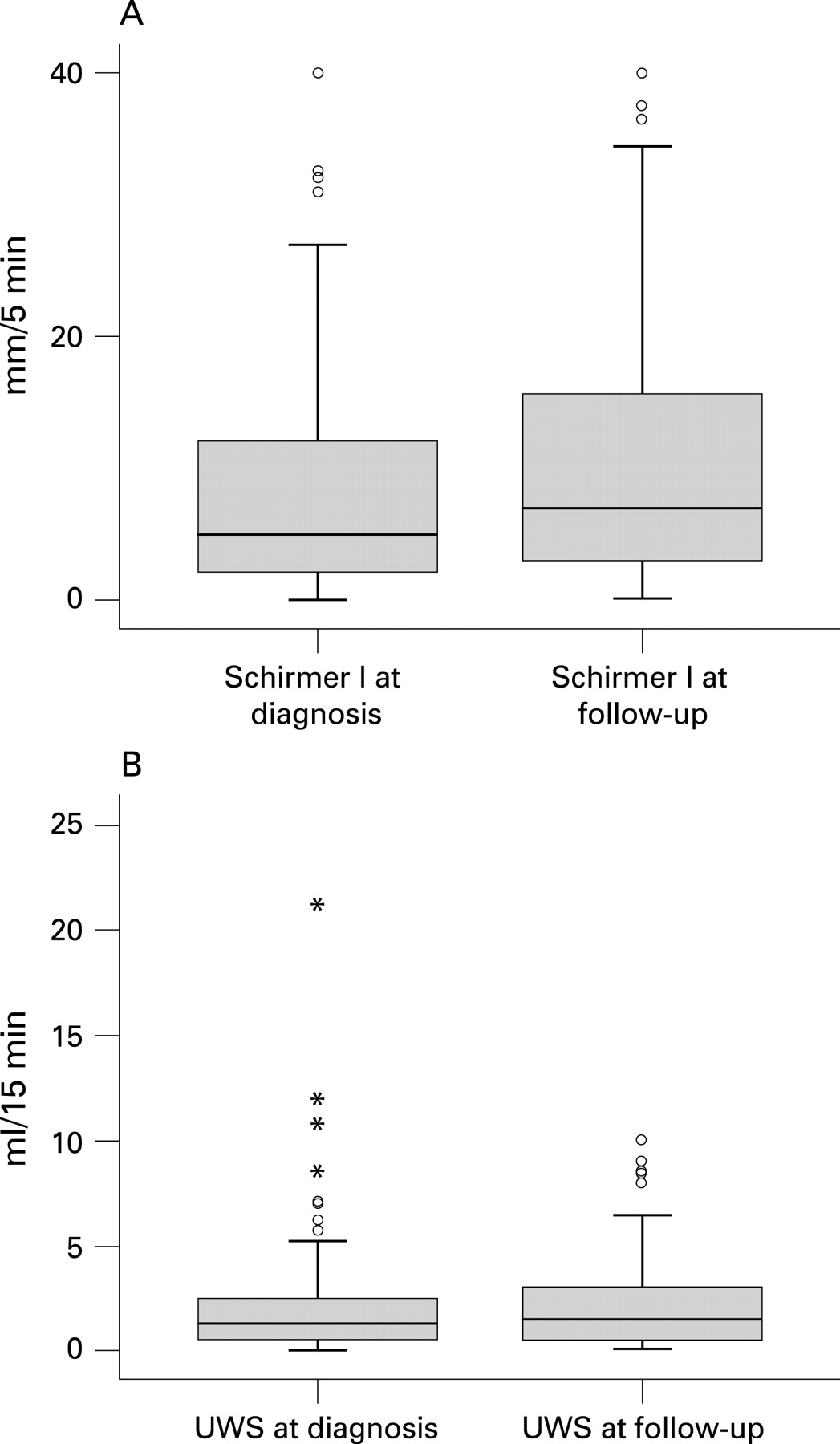
During the observation period there was an increase of the median Schirmer I test from 5.0 to 7.0 mm/5 min (p<0.05, n = 111, fig 1A). A total of 52 (36.9%) patients had an increase of 30% or more of the Schirmer I test, while 34 (24.1%) patients had a decrease of 30% or more. The median UWS was not significantly changed during the observation period (1.30 and 1.50 ml/15 min, p = 0.26, n = 114, fig 1B). A total of 45 (31.9%) patients had an increase of 30% or more of the UWS, while 42 (29.8%) patients had a decrease of 30% or more. Whether or not patients took antimalarials, methotrexate or oral steroids did not give significant differences with respect to a 30% increase or decrease in Schirmer I test or UWS. The Schirmer I test and UWS correlated well with corresponding historical measurements (table 2). On both visits, nine patients had zero UWS, and three patients had zero Schirmer I test, these were included in the 30% decrease groups. There were no longitudinal data on subjective sicca measures.

{kind=link}
Factors associated with a worsened exocrine function
The present Schirmer I test was associated with a range of variables from the time of diagnosis. Significant correlations were found between Schirmer I test and focus score, IgG and IgA (table 2). Schirmer I test was lower among patients with SSA or SSB antibodies, with a median of 7.50 (4.0–21.5) mm/5 min for SSA negative vs 7.0 (2.0–13.4) for SSA positive, p = 0.04), and 8.5 (3.5–20.5) for SSB negative vs 6.0 (1.5–10.5) for SSB positive, p = 0.01. Corresponding results regarding present UWS also showed lower values among patients positive for SSA or SSB antibodies, but these results were not significant. Whether ANA was positive or negative at diagnosis did not significantly affect the UWS or Schirmer I test at follow-up.
In univariate analyses, a 30% or more worsening of the Schirmer I test or UWS was associated with focus score, but not the other variables from the time of diagnosis (table 3). However, when dichotomising the C3 and C4 (low C3/C4 or not) a significant association was found with UWS (table 3). A multivariate logistic regression with 30% worsening or more of the Schirmer I test as dependent variable was performed. Age, gender, time since diagnosis and the variables from time of diagnosis that had significant associations with the present Schirmer I test or a worsened Schirmer I test were the independent variables. In this model, focus score and previous UWS were identified as independent predictive factors for a worsened lacrimal function. In a corresponding logistic regression analysis with worsening of the UWS by 30% or more as the dependent variable, only focus score was identified as an independent predictive factor for a worsened salivary function (table 4).
DISCUSSION
The course of primary Sjögren syndrome typically reflects the consequences of reduced lacrimal and salivary flow. Few patients in our study used disease-modifying antirheumatic drugs (DMARDs). In addition, DMARDs have not been shown to influence on the exocrine function in SS.17 Thus, the observed exocrine function over time may be seen as the natural course in our patients. Saliva performs an important role in maintaining and protecting oral health, eg, growth factors and soft-tissue repair, buffer activity, re-mineralisation, immunity and defence eg, against Candida (chronic erythaematous infection in 70–75%).18 Measures of decayed, missing and filled teeth are increased in SS.19 20 In one study, loss of teeth in SS due to caries preceded the first mouth dryness symptoms by on average 9 years.20 Dryness also leads to problems with speech and swallowing. Concerning measures of salivary excretion, unstimulated whole saliva is mostly used, some studies use gland-specific sialometry instead. UWS is more readily measured in a clinical setting, though stimulated whole (or gland-specific) saliva may be a more sensitive measure when gland function is low. The ocular problems are eg, foreign-body sensation and irritation, and complications like corneal ulceration and scarring, in some patients possibly causing visual impairment, with considerable functional disability.21
Mostly cross-sectional and only a few longitudinal studies on the long-term clinical course of SS have been performed. Apart from exocrine function, there are longitudinal data on lymphoproliferative disease, lung disease and quality of life measures in SS. The findings in these studies, including any identified predictive factors, are summarised in table 1.
Although primary Sjögren syndrome earlier has been described as a chronic progressive disease, most works mentioned here indicate instead a stable and rather mild course of glandular and extraglandular manifestations, with the exception of an increased risk of malignant lymphoma.1 Four previous studies found a stable lacrimal and salivary function.2–5 According to Kruize et al, the ocular component showed a steady state over 10 to 12 years.3 4 The oral component showed relative stability over a minimum of 5 years in a study with 49 patients.5 A recent study found declining stimulated gland specific saliva over time but more stable unstimulated quantities in early SS.6 Only one of these investigations looked for possible predictive factors for the exocrine function in SS: in a group of 47 patients followed for 5 years, Theander et al7 found no significant change in the Schirmer I test or unstimulated whole saliva, but a small worsening of the Van Bijsterveld score. SSA positivity and low levels of C3 and C4 predicted further decline in the Van Bijsterveld score. This was the first report of a laboratory test predicting changes in exocrine function in primary Sjögren syndrome.
Previous studies were relatively small, differences between study populations are striking, and estimates from these small sample sizes may not reflect the actual situation in an SS population. Another methodological problem may be limitations in classification. Different criteria were used earlier,22 and the present AECC may also entail some data variation in studies. Subjects without autoimmune disease may be included in SS studies because up to 15% of normal controls may show a focus score ⩾1.23 24 Modern ELISA-based methods for anti-SSA and SSB antibodies are very sensitive but not equally specific, and antibodies can sometimes be found in normal subjects.25
Additionally, the stable course observed in most of these studies may be influenced by floor–ceiling effects, falsely giving the impression of a stable disease course, as Theander et al7 emphasise. In our study, we did not experience high risk of floor–ceiling effects, with only nine patients with zero UWS on both visits, and three patients scoring zero on the Schirmer I test twice. The reason for this difference to the work by Theander et al7 may be the lower median age of 57 years of our patients, in contrast to 64 years in the study by Theander et al, with exocrine function naturally declining in the general population.
The diagnostic delay in SS is typically 5 to 10 years, and most of the exocrine function loss may develop prior to diagnosis, possibly also extraglandular manifestations. Pijpe et al6 tried to avoid this bias by defining disease duration as time since the first dryness symptoms, and not time since diagnosis. Though they had a small study population, their results indicate that most changes in exocrine function take place very early in the disease course. Early diagnosis therefore seems important with respect to any treatment to halt the decline in glandular function.
Concerning prognostic factors for decreased exocrine function, former studies have not found any correlation with focus score. The present study has the hitherto largest sample size, and is based on the latest classification criteria and standardised examination procedures. It is the first showing high focus scores, and also low UWS, as independent predictors of a worsened exocrine function. At the same time, the data show great variation: At least a 30% increase or decrease in Schirmer I test was experienced by 37% and 24% of 111 patients, respectively, although the data altogether showed a significant increase in tear flow (fig 1A). At least a 30% increase or decrease in UWS was found in 32% and 30% of 114 patients, respectively (fig 1B).
CONCLUSIONS
In primary Sjögren syndrome, results to date indicate that except in early disease stages, salivary and lacrimal function remains relatively stable over time, and that SSA seropositivity and low complement levels may predict a decline in exocrine function. In 141 subjects with SS, we confirmed previous studies showing a rather stable or slightly improved exocrine function over time. High focus scores and low UWS were identified as independent predictors of a worsened exocrine function. There was a significant increase in the Schirmer I test, though the data show great variation in individual development. We have carried out a longitudinal study with a retrospective cohort design, the ideal design would be a prospective study. The natural course of, or prognostic factors for the exocrine function in SS is not sufficiently explored. Future works should aim at longitudinal studies earlier in the disease course, and there is also a need to examine more thoroughly the predictive factors concerning glandular and extraglandular features of SS.
Acknowledgments
We thank the Department of Otolaryngology/Head and Neck Surgery and the Department of Oral Pathology, Haukeland University Hospital, for obtaining and assessing routine minor salivary gland biopsies. We thank the Department of Microbiology and Immunology and Laboratory of Clinical Biochemistry, Haukeland University Hospital, for routine laboratory testing.
REFERENCES
Footnotes
Competing interests: None declared.
Funding: This project was supported by a grant from the Reidun Aasgård Foundation, Helse Vest, the Strategic Research Program at Helse Bergen, and a grant from University of Bergen regarding rheumatology research.
Ethics approval: The study was approved by the Regional Committee for Medical Research Ethics, and all patients provided written informed consent before inclusion.