Article Text

Abstract
Objective: Treating early active rheumatoid arthritis (RA) with disease modifying antirheumatic drug (DMARD) monotherapy achieves incomplete outcomes and intensive treatment seems preferable. As the relative benefits of combining two DMARDs, one DMARD with glucocorticoids and two DMARDs with glucocorticoids are uncertain we defined them in a factorial trial.
Methods: A 2-year randomised double-blind factorial trial in patients with RA within 2 years of diagnosis treated with methotrexate studied the benefits of added ciclosporin, 9 months intensive prednisolone or both (triple therapy). The primary outcome was the number of patients with new erosions. Secondary outcomes included Larsen’s x-ray scores, disability, quality of life and adverse events.
Findings: 1391 patients were screened and 467 randomised. Over 2 years 132 (28%) changed therapy and 88 (19%) were lost to follow-up. The number of patients with new erosions was reduced by nearly half by adding ciclosporin or prednisolone (p = 0.01 and 0.03); both treatments reduced increases in Larsen’s x-ray scores by over 2 units (p = 0.008 and 0.003). A further reduction in erosive damage was seen with combined use of both treatments. Their effects on erosive damage appeared independent. Triple therapy reduced disability and improved quality of life compared with methotrexate; ciclosporin and prednisolone acted synergistically. More patients withdrew because of adverse events with triple therapy, without an increase in serious adverse effects.
Conclusions: This study confirms the existence of a “window of opportunity” in early RA, when intensive combination therapy produces sustained benefits on damage and disability. Although methotrexate–prednisolone combinations reduce erosive damage, the synergistic effect of two DMARDs is needed to improve quality of life.
Statistics from Altmetric.com
There is intense interest in the optimal management of early rheumatoid arthritis (RA). UK and EULAR guidance1 2 recommends disease modifying anti-rheumatic drugs (DMARDs) should be initiated early with intensive management incorporating escalating doses of DMARDs, glucocorticoids and combination therapy. The rationale includes long-term randomised controlled trials (RCTs) and observational studies that show sequential DMARD monotherapy often results in progressive joint damage and high disability scores.3–7
Intensive therapy in early RA may involve DMARDs or tumour necrosis factor (TNF) inhibitors. Guidance in the UK,8 9 continental Europe10 and internationally11 means TNF inhibitors cannot be used initially. Consequently, intensive early treatment will currently involve conventional DMARDs and glucocorticoids. There is evidence giving two DMARDs or one or more DMARDs with glucocorticoids2 3 12–27 improves outcome. However, the optimal DMARD combination and the value of glucocorticoids are uncertain. TNF inhibitors alone28 or, more especially, in combination with methotrexate26 27 29–32 also improve outcome. The benefits of all combination therapies must be weighed against increased adverse events.33 TNF inhibitors also have specific problems, including high costs and concerns about malignancy.34 Although there is uncertainty about the relative merits of intensive DMARD therapy and early biologics,35 the evidence favours early intensive therapy targeting the window of opportunity in early RA.36–43
We addressed the merits of intensive therapy with conventional drugs in early active RA assessing the relative benefits of two DMARDs, adding prednisolone to one DMARD or using two DMARDs with prednisolone in a factorial-design RCT. Factorial trials usually allow simultaneous evaluation of two interventions in a 2×2 design. Patients are randomly assigned to one of four groups. One group receives neither intervention, a second group receives one intervention, a third group receives the other intervention and the fourth group receives both interventions. Matching placebos maintain blinding. The effects of each intervention can be compared simultaneously and synergistic or negative interactions between interventions evaluated. Such factorial designs have helped optimise combination therapies in cancer and cardiovascular diseases as outlined by McAlister et al.44 In our trial all patients received methotrexate as standard treatment. One additional treatment was “step-down” prednisolone, selected because of its known efficacy and safety in early RA. The other additional treatment was ciclosporin, which was increased incrementally to a pre-defined target dose, was selected because of its combined efficacy with methotrexate45 and ability to reduce erosions.46 The factorial trial lasted 2 years, which is often considered the minimal time to show genuine disease modification.
PATIENTS AND METHODS
Participants
Consecutive patients with early RA who were seen in routine rheumatology outpatient clinics at 42 centres in England and Wales were enrolled into the trial.
Inclusion criteria
This was determined as active RA by American College of Rheumatology (ACR) criteria of less than 24 months with three of the following: ⩾3 swollen joints, ⩾6 tender joints, ⩾45 min morning stiffness, erythrocyte sedimentation rate (ESR) ⩾28 mm/h. Other inclusion criteria were that patients needed to give informed consent and were aged ⩾18 years.
Exclusion criteria
These were other inflammatory arthropathies (eg, psoriatic arthritis), current oral glucocorticoids, serious medical disorders (eg, hepatic or cardiac failure), women of child-bearing potential without adequate contraceptive protection, and contraindications for trial drugs. We recorded details of non-recruited patients in line with CONCORD recommendations.
Interventions
Study drugs
These were: (a) open-label methotrexate (starting 7.5 mg weekly, increasing incrementally to target dose of 15 mg/week); (b) “step-down” prednisolone started with methotrexate (60 mg/day initially, reduced to 7.5 mg at 6 weeks, 7.5 mg daily from 6 to 28 weeks, stopped by 34 weeks); and (c) ciclosporin started 3 months after methotrexate (initial dose 100 mg/day, increased gradually to target dose of 3 mg/kg daily). Prednisolone and ciclosporin were given as active tablets or matching placebos.
Study drugs were varied by supervising rheumatologists for: (a) adverse effects; (b) uncontrolled disease activity; (c) intercurrent illnesses/surgery. Central advice (EHSC) recommended changes in ciclosporin dose for renal function and blood pressure.
Concomitant therapy
Analgesics (paracetamol or co-proxamol) and/or non-steroidal anti-inflammatory drugs were used at standard dosages. Other drugs (eg, hypertensives) were continued as needed. To limit toxicity patients received folate supplements (5 mg/week) and bone protection (calcium and vitamin D supplements and optional bisphosphonates). Intra-articular glucocorticoids (40 mg methylprednisolone with lignocaine) were given (⩽6 occasions) as required. Intramuscular glucocorticoids were allowed but only three doses of 120 mg of depot methylprednisolone could be given in a year. All intra-particular and intramuscular steroid treatments will be recorded.
Safety monitoring
National guidelines were followed (monthly blood counts, liver and renal function tests, urinalysis, blood pressure). Patients were asked about adverse events. DEXA scans (spine, hip) were undertaken at 0 and 2 years.
Objective
Testing the hypothesis combining methotrexate with glucocorticoids and/or ciclosporin in early RA reduced the proportion of patients developing new erosions within 2 years. A clinically relevant reduction was 40% fewer patients developing new erosions.
Primary outcome
The primary outcome was the development of new erosions in x-rays of hands and feet.
Secondary outcomes
These comprised changes in total Larsen score for x-ray damage, function, quality of life, disease activity and adverse events. Patients were screened for eligibility then assessed at entry and every 6 months.
x-Rays of hands and feet
These were read chronologically and independently by two observers (DLS, LC) after preliminary studies had ensured comparable scoring of new erosions and modified Larsen scores.47 These methods were chosen to replicate the methods in the ARC trial of glucocorticoids in early RA.2
Function
The Health Assessment Questionnaire (HAQ) was used to determine function.
Quality of life
SF-36 (summary physical and mental component scores) and EuroQol were used to determine quality of life.
Disease activity
Clinical core data (28 swollen and tender joint counts, visual analogue scores for pain, assessors’ global and patients’ global assessment, ESR) used to calculate disease activity score (DAS28) for 28 joints and ACR-20, 50 and 70 responder rates. Disease remission is defined as DAS28 <2.6.48
Adverse events
All events were recorded whether or not they were considered treatment-related.
Sample size
Previous data from Kirwan2 indicated 46% of patients receiving one DMARD develop new erosions after 2 years. Sample size calculations were based on a logistic regression model for dual therapy taking a 40% reduction in cases developing new erosions as clinically relevant. In a 2×2 factorial design with equal group sizes a sample size of 438 is required to achieve 90% power, conservatively assuming triple therapy leads to a 56% reduction. This corresponded to 110 in each group; allowance for 5% of patients who may withdraw consent gave a planned recruitment number of 464.
Randomisation
The study involved four geographical regions (London, West Midlands, North East and South West). Patients were randomly allocated to one of the four groups stratified by region.
Sequence generation, allocation concealment and implementation
The allocation sequence was generated by VF (statistician). Randomisation, stratified by region, used random treatment assignment in balanced blocks of 16. Metrologists performed the screening visit and faxed anonymised data to the trial centre. CMS (co-ordinator) assigned consecutive patient numbers (within strata) to patients in chronological order when they passed the screening assessment. The metrologists and co-ordinator were unaware of the allocation sequence. Treatment assignments were in a locked cabinet in the co-ordinating centre pharmacy for emergency access.
Blinding
The study was fully blinded with matching placebos for oral glucocorticoids and ciclosporin. x-Rays were read independently by DLS and LC without knowledge of the treatments. HAQ, SF-36 and EuroQol were completed by patients and scored independently of supervising clinicians. Disease activity was assessed by the visiting metrologist without knowledge of treatments.
Statistical methods
Data were analysed on an intention to treat basis at the end of the trial. The primary outcome was evaluated by logistic regression analysis, stratified by region. Odds ratios (ORs) and confidence intervals (CIs) were calculated for the main effects of prednisolone and ciclosporin. Information on interaction effects was examined, although the study was not powered for this analysis. Secondary outcomes were analysed in a comparable fashion using a general linear model and analysis of variance. These analyses were also used to calculate number needed to treat (NNT) and number needed to harm (NNH). Missing data were imputed through last observations carried forward (LOCF). Pre-planned subgroup analysis examined the effects of age, sex, region, rheumatoid factor and disease activity using logistic and linear regression.
Ethics review
The trial was approved by the South East Multicentre Research Ethics Committee and local research ethics committees at each centre.
Trial registration
The trial was registered by the sponsor (Medical Research Council) at http://www.controlled-trials.com as ISRCTN no.32484878 (accessed 28 December 2006).
RESULTS
Participants and recruitment
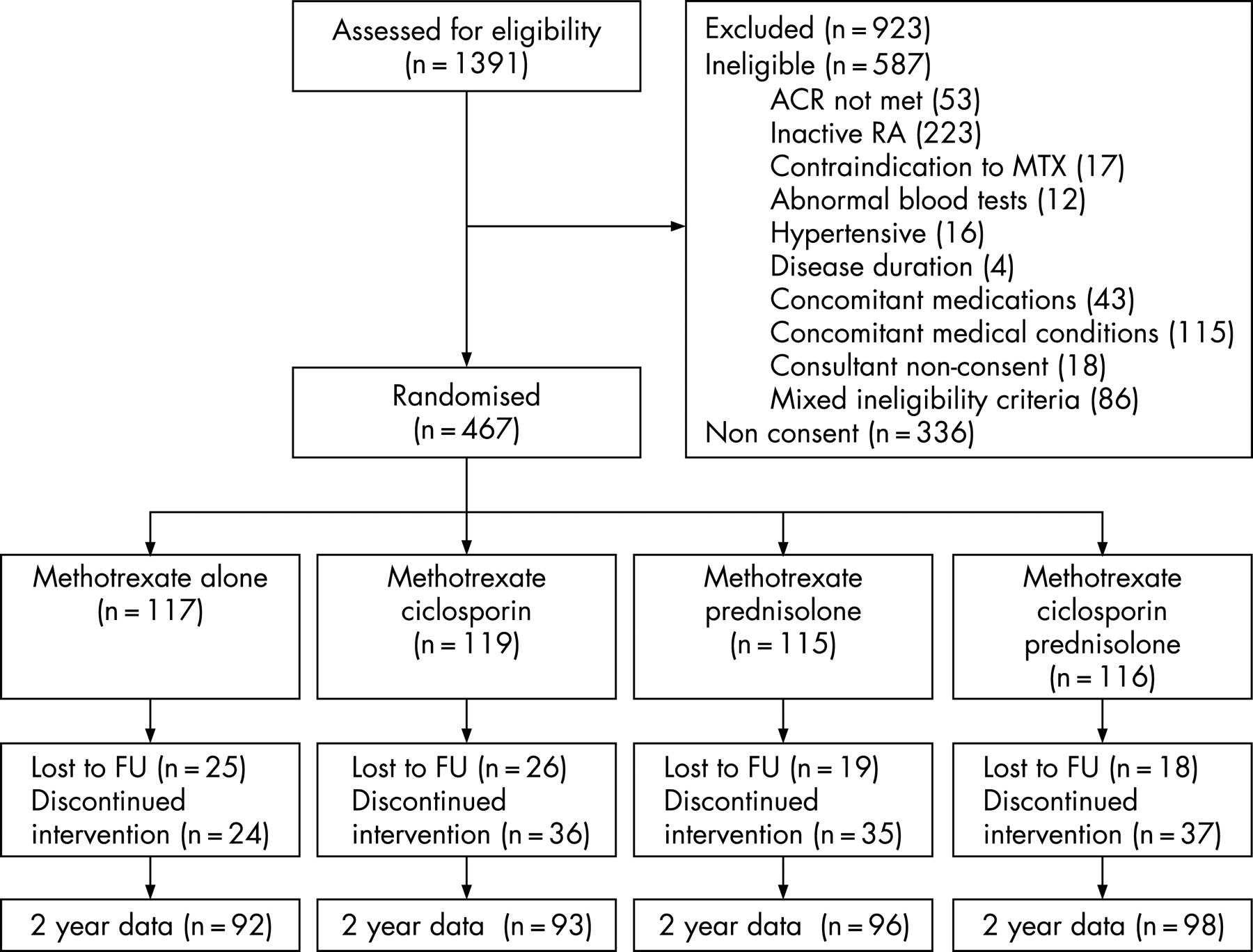
A total of 1391 patients were screened at 42 rheumatology units: 587 patients were ineligible and 804 patients were eligible; 337 of these 804 eligible patients declined to participate and 467 were randomised (fig 1). Patients were recruited from 2000 to 2002, follow-up was completed in 2004 and data validated in 2005.
Baseline data
A total of 312 (67%) patients were rheumatoid factor positive, 103 (22%) had rheumatoid nodules and 154 (33%) erosive damage. Sixty-five (14%) had previously received DMARDs. Mean (95% CI) clinical assessments comprised 11.8 (11.1, 12.5) tender joints, 9.9 (9.3, 10.4) swollen joints, ESR (mm/h) 41 (38, 44), assessor global (VAS mm) 48 (46, 50), patient global (VAS mm) 55 (53, 57) and pain (VAS mm) 48 (45, 50). The groups were well matched (table 1).
Cases analysed
A total of 247 (53%) patients continued allocated treatment for 2 years, 88 (19%) were lost to follow-up and 132 (28%) changed treatment. At 24 months, results were available in 379 (81%); data from the remaining 88 (19%) were imputed using LOCF. Observed case analysis was also carried out to check the impact of the LOCF assumption.
Primary outcome
With methotrexate monotherapy, 34 (29%) patients developed new erosions (table 2). Logistic regression analysis showed reductions with prednisolone (OR 0.59 (95% CI 0.36, 0.96), p = 0.03) and ciclosporin (OR 0.54 (95% CI 0.33, 0.88), p = 0.01). Least new erosions were seen with triple therapy (15 of 116, 13%), regression analysis showed no multiplicative effects (p = 0.32), although sample size of the study was not powered to detect interaction. Analyses omitting patients with missing data at 2 years gave estimated ORs of 0.55 (p = 0.02) and 0.56 (p = 0.02) for ciclosporin and prednisolone.
Based on the estimated ORs from the stratified factorial analysis, and an assumed baseline rate of new erosions of 29% (from the methotrexate arm), the number needed to treat (NNT) to stop erosive progression was 11 (95% CI 6, 120) with added prednisolone and 10 (95% CI 6, 39) with added ciclosporin. The estimated NNT for triple therapy was 6 (95% CI 4, 14).
Secondary outcomes
Larsen scores
These increased most with methotrexate monotherapy, though the rate of increase declined with time (fig 2). Ciclosporin reduced progression throughout the 2-year period. Prednisolone showed a rapid initial effect without a “rebound” increase after stopping steroid therapy. At 24 months the mean increase in Larsen score was 7.41 (95% CI 5.47, 9.33) with methotrexate monotherapy. Stratified factorial analysis estimated reductions of 2.33 and 2.11 with ciclosporin and prednisolone respectively (p = 0.003 and 0.008) with no significant interaction (p = 0.45) between prednisolone and ciclosporin (table 2). Observed case data at 24 months gave estimated reductions of 2.39 for ciclosporin and prednisolone (both p = 0.004).

Disability
HAQ scores decreased with all treatments by 6 months (fig 2): with methotrexate monotherapy and added ciclosporin mean HAQ scores fell by 0.21 and 0.23; with added prednisolone and triple therapy they fell by 0.53 and 0.63. At 24 months HAQ scores showed a mean fall of 0.29 with methotrexate monotherapy. Stratified factorial analysis showed a significant synergistic interaction between therapies (p = 0.01); estimated mean changes in HAQ were −0.20, −0.28 and −0.50 with additional ciclosporin, additional prednisolone, and triple therapy compared with methotrexate alone (table 2). An observed case analysis gave similar results.
Quality of life
SF-36 PCS showed similar changes to HAQ (table 2). Mean increases at 24 months were 5.8 with methotrexate; adding ciclosporin or prednisolone alone gave no benefits but with triple therapy the mean increase was 8.0. Stratified factorial analysis showed no significant reductions in SD-36 PCS at 24 months with ciclosporin or prednisolone, but a significant interaction with triple therapy (p<0.01). There were no differences in SF-36 Mental Component scores or with EuroQol. Observed case analyses gave comparable results.
Disease activity
Disease activity fell in all groups by 6 months: with methotrexate monotherapy and added ciclosporin mean falls in DAS28 were 1.14 and 1.49 and 9% and 14% were in DAS28 remission; with added prednisolone and triple therapy mean falls were 1.81 and 1.84 with 36% and 31% in DAS28 remission. At 24 months mean falls in DAS28 were 1.42 with methotrexate monotherapy (table 2) and with triple therapy mean DAS28 scores fell by 1.67; stratified factorial analysis showed no significant differences between treatment arms. DAS28 remission at 24 months occurred in 21 of 117 (18%) patients receiving methotrexate, 27 of 119 (10%) and 23 of 115 (20%) receiving added ciclosporin and added prednisolone and 32 of 116 (28%) on triple therapy. Detailed changes in disease activity (ACR responders and mean DAS28 scores) over time are shown for methotrexate monotherapy and triple therapy in fig 3. Triple therapy reduced all assessments of disease activity by 6 months compared with methotrexate monotherapy but thereafter the number of responders in the patients initially randomised to receive methotrexate increased and by 24 months the groups were similar.

{kind=link}
{kind=link}
{kind=link}
Adverse events and withdrawals
Adverse events
A total 81 (17%) patients had serious adverse events (table 3), including five deaths (one ovarian cancer, one cerebrovascular accident, three sudden/unexpected). Three patients had strokes, three angina, three myocardial infarctions and 16 infections (two tuberculosis and three pneumonias). These serious adverse events were unrelated to treatment group.
Prednisolone resulted in hypertension (OR 2.16; 95% CI 1.07, 4.36) and larger falls in hip DEXA scores (p = 0.03). Ciclosporin also resulted in hypertension (3.35; 1.57, 7.12), mouth ulcers and headaches were commoner, and many patients had transient creatinine elevations (OR 9.13; 95% CI 4.32, 19.30) that did not persist beyond 2 years.
Withdrawals
Seventy-one (15%) patients withdrew for toxicity and the same number for inefficacy. Toxicity was implicated in more withdrawals, prednisolone, ciclosporin and triple therapy. Based on a factorial analysis, which showed no evidence of an interaction (p = 0.95), and an assumed baseline rate of withdrawals due to toxicity of 9% (from the methotrexate arm), the NNH for any adverse event leading to withdrawal was 20 (95% CI 8, 1280) with added ciclosporin and 14 (95% CI 6, 65) with added prednisolone. The estimated NNH for triple therapy, based only on data from patients receiving this therapy was 6 (95% CI 3, 23).
DISCUSSION
Our results show combining “step-down” prednisolone or ciclosporin with methotrexate reduces erosive damage in active early RA. Prednisolone and ciclosporin have independent, additive effects on erosive damage. Prednisolone exerts its effects on erosive damage early. Ciclosporin has less prominent early effects on erosive damage; its benefits extended over 2 years. Triple therapy shows synergistic long-term effects on disability and health status. With both prednisolone and ciclosporin the NNT for stopping erosive progression (8) is substantially less than the NNH for an adverse effect resulting in withdrawal (12 and 14 respectively). With triple therapy the NNT and NNH are both 6, but this more intensive treatment has additional sustained benefits on disability and quality of life.
Our results confirm previous RCTs showing glucocorticoids given either with2 3 12 13 15 22–24 26 27 or without49 50 DMARDs reduce progressive erosive damage in early RA, which has also been confirmed in a systematic review.51 Theoretically DMARD co-prescribing could mask this benefit of glucocorticoids.52 Our results confirm previous RCTs showing adding ciclosporin to methotrexate without glucocorticoids reduces erosive damage;18 19 21 though other DMARD combinations may not reduce erosive damage.16 20 25–27 Overall RCTs of intensive therapy suggest two DMARDs and glucocorticoids is the optimal conventional treatment for early RA. Most trials use the COBRA12 regimen of high dose/rapidly tailing glucocorticoids rather than low-dose glucocorticoids.2 Such “step down” prednisolone gives lower overall cumulative 2-year doses (3740 mg vs 5475 mg with 7.5 mg daily) without the resumption in erosive damage after stopping glucocorticoids seen with low-dose glucocorticoids.53 Nevertheless the optimal steroid regimen in early RA remains undecided. An additional issue is the optimal dose of methotrexate; although we used up to 25 mg per week, which is widely recommended,1 there is evidence more intensive treatment regimens may give better results.54
RCTs have compared TNF inhibitors plus methotrexate against DMARD monotherapy alone29–32 and also against both intensive DMARD/steroid combinations and DMARD monotherapy.26 27 Overall, TNF inhibitors with methotrexate show comparable improvements in disease activity and disability to intensive DMARD/steroid combinations in a head-to-head RCT26 27 and a comparative meta-analysis.55 However, TNF inhibitors with methotrexate may give greater reductions in radiological progression.
RCTs in early RA use varying x-ray assessments. We used Larsen scores, which were used in RCTs by Kirwan3 and other investigators15 19 21 24 and comparable observational studies.6 56 Other RCTs use Sharp scores;3 12 13 16–18 23 25–27 one used both Rattingen (Larsen variant) and Sharp scores.22 The relative utility of different x-ray scores is contentious.57–59 RCTs vary in recording patients considered for entry; we recorded details of non-recruited patients following CONCORD recommendations; 42% of patients screened were ineligible and 24% declined. The number of patients with mild RA reflected the numbers of patients in the Norfolk Arthritis Register who did not need DMARDs.55 Other early RA RCTs do not reported this screening information.
Though evidence favours intensive treatment in early RA, it is rarely used in routine care60 61 often because of concerns about glucocorticoids, which persists despite reassurance.62 63 An associated issue is the increased toxicity of intensive treatment regimens.33 Although the benefits of intensive treatment outweigh its risks, and combinations such as the COBRA regimen seem less toxic,12 patients continue to have greater concerns about adverse events than about treatment benefits;64 consequently, many patients may prefer a conservative approach. Such concerns may be partially allayed by choosing combinations with less long-term toxicity than ciclosporin. In addition there are important roles for patient education in implementing intensive treatments such as step-down in routine clinical practice, and the optimal ways to enhance such education merits further investigation. Intensive treatment is not yet ideal. Over 30% of our patients receiving triple therapy had active DAS28 ⩾5.1 after 12 months; RCTs of other intensive treatment give comparable results. The ultimate goal is identify ways of increasing the efficacy of intensive initial treatment without enhancing its toxicity.
Acknowledgments
Trial Steering Committee: Professor Roger Sturrock (Chair); Professor Vern Farewell (Statistician); Dr David Walker, Dr Andrew Hassell, Dr Adam Young and Professor David Blake (Regional Collaborators); Professor Paul Bacon and Professor David Isenberg (Independent members); Neil Betteridge (Patients’ Advocate); Professor Ian Harvey (Advisor on Clinical Trials); Dr Alison Carr (Advisor on Health Status); Dr Luke Archard (Advisor on Health Economics). Data Monitoring and Ethics Committee: Professor DGI Scott (Chair), Professor Bryan Williams, Dr Alex MacGregor, and Janice Mooney; Rheumatologists: London region: Dr O Duke and Dr SR Patel (St Helier); Dr TR Price, Dr AL Dolan and Dr G Coakley (Queen Elizabeth, Woolwich); Professor K Chakravarty (Harold Wood); Dr D MacFarlane and Dr Warr (Pembury); Dr A Hammond (Maidstone); Dr N Gendi (Basildon); Dr MS Irani (Ashford); Dr B Dasgupta and Dr Wong (Southend); Dr N Cheung (Queen Mary’s, Sidcup); Dr J Wojtuleskwi (Eastbourne); Dr PL Williams (Medway); Dr C Erhardt (Bromley); Dr AB Bhanji (Homerton); Professor C Pitzalis and Dr T Garood (King’s College); Dr GH Kingsley and Dr V Hajela (Lewisham); Dr P Pitt (Orpington); Dr D Doyle (Whipps Cross); Dr C Kelsey (Oldchurch); Dr M Lloyd (Frimley Park); Professor G Panayi (Guy’s); Dr SM Griffiths (East Surrey); Dr J Griffin and Dr D Fishman (Chase Farm); Dr A Jawad (Royal London); and Dr R Sturge and Dr C Smith (Barnet).
West Midlands region: Dr P Dawes, Dr MF Shadforth and Dr EM Hay (Haywood); Dr D Mulherin and Dr T Price (Cannock Chase); Professor D Symmons and Dr SM Knight (Macclesfield); Dr R Butler (Oswestry); Dr AJ Farrell (Leighton); Dr M Allen (Walsgrave); Dr I Pande (Nottingham); and Dr G Kitas (Dudley). North East region: Dr LJ Kay, Dr I Griffiths, Dr P Platt and Dr ML Grove (Freeman/North Tyneside); Dr M Plant and Dr J Fordham (James Cook University Hospital); Dr AJ Chuck (Dryburn); Dr C Kelly (Queen Elizabeth, Gateshead); and Dr P Crook (Ashington). South West region: Dr NL Cox (Royal Hampshire County Hospital and the Royal National Hospital for Rheumatic Diseases); Dr SM Jones (University Hospital of Wales); Dr P Creamer and Dr Hollingworth (Southmead); Dr M Davis, Professor A Woolf and Dr D Hutchinson (Royal Cornwall); and Dr S Richards and Professor PW Thompson (Poole).
REFERENCES
Footnotes
Funding: This trial was funded by the Medical Research Council, UK.
Competing interests: None.