Article Text

Abstract
Objective: To investigate the relationship between the magnitude of clinical response in the first 6 months of methotrexate (MTX) therapy and long-term outcome in children with juvenile idiopathic arthritis (JIA).
Methods: The clinical charts of 125 JIA patients who were started with MTX and then followed for at least 5 years were reviewed. Based on the level of American College of Rheumatology (ACR) Pediatric response at 6 months, patients were divided in four mutually exclusive groups: (1) non-responders, (2) responders at 30%, (3) responders at 50%, and (4) responders at 70%. The long-term outcome in each response group was evaluated by calculating the percentage change in active and restricted joint counts from baseline to 1, 2 and 5 years and the frequency of inactive disease at 5 years.
Results: At 6 months, 42 patients were classified as non-responders, 24 as 30% responders, 26 as 50% responders, and 33 as 70% responders. Patients who had achieved a 70% response showed a significantly greater percentage improvement in active joint count between baseline to 5 years compared with non-responders and 30% responders, and a significantly greater percentage improvement in restricted joint count between baseline to 5 years compared with 30% responders. The 70% responders also had a greater frequency of inactive disease at 5 years compared with 30% responders,
Conclusions: Our results show that the achievement of an ACR Pediatric 70 response at 6 months after start of MTX therapy predicts a more favorable long-term outcome of patients with JIA.
Statistics from Altmetric.com
The effectiveness of therapies for juvenile idiopathic arthritis (JIA) is assessed using the American College of Rheumatology (ACR) Pediatric 30 definition of improvement.1 This definition is based on a core set of six outcome measures (physician’s global assessment of the overall disease activity, parent’s global assessment of the child’s well-being, count of joints with active disease, count of joints with restricted motion, functional ability assessment, and an acute phase reactant) and requires, to enable classification of a patient as responder at the end of a trial, an improvement of at least 30% with respect to baseline in at least three of the six core set items, with no more than one of the remaining worsened by more than 30%. The therapeutic response can also be evaluated using more stringent definitions, such as the ACR Pediatric 50 and ACR Pediatric 70, in which patients must improve by at least 50% or 70%, respectively, in individual core set measures to be characterised as improved. The utility of such standardised response criteria is well established for use in clinical trials, where the proportion of patients responding constitutes a measure of efficacy compared to placebo or a standard treatment, such as methotrexate (MTX). This practice has greatly facilitated the evaluation of novel therapies for JIA.2–7
In adult patients with rheumatoid arthritis, it has been argued that an improvement in disease activity measures at a level of 50% or less, such as that captured by the ACR20 or ACR50 definitions,8 9 may not reflect a major clinical response to treatment.10 The course of disease activity in chronic arthritis is often fluctuating and, thus, a partial improvement in the short-term timeframe of a trial may not translate into long-lasting benefit. Furthermore, several reports have documented that measures of inflammatory arthritis, such as those included in the clinical response core sets, may be stable or improved over periods of 5–10 years, while measures of damage, such as radiographic progression or physical function, may progress over the same period.11 In recent years, the availability of more efficacious therapies has increased the expectations of benefit of treatment, which has raised the question as to whether the goal of future clinical trials might be levels of improvement higher than ACR20, or even higher than ACR50, or absolute measures of efficacy, such as Disease Activity Score (DAS)12 or ACR criteria for remission.13 However, the definitions that require lower levels of response (ACR20) may be more discriminative between the placebo and the index drug in clinical trials,14 although a recent meta-analysis of 21 clinical trials conducted in adult patients with rheumatoid arthritis has indicated similar discriminant capacities of ACR20 and ACR50 responses.15 Nevertheless, the optimal threshold level of improvement to be used in clinical trials is still uncertain.9
It has been suggested that important insights into the relative clinical meaning of the different levels of therapeutic response can be obtained by investigating their prognostic value.16 A study in adult patients with rheumatoid arthritis found that a good response to disease-modifying antirheumatic drug treatment during the first year predicted remission during follow-up.17 To explore this issue in childhood chronic arthritis, we investigated the relationship between the level of clinical response to MTX therapy in the first 6 months and the long-term outcome in a group of children with polyarticular JIA.
PATIENTS AND METHODS
Patient selection
The clinical charts of all consecutive patients who had JIA by the International League of Associations for Rheumatology (ILAR) revised criteria,18 were started with MTX at the study units between November 1986 and September 2000, and had a follow-up of at least 5 years after the beginning of MTX therapy (baseline), were reviewed. All patients seen before the publication of ILAR criteria for JIA were re-classified using such criteria.
Baseline clinical and radiographic assessment
Patient information recorded at baseline included: onset age, sex, ILAR category, disease duration, and MTX dosage. The following baseline clinical and radiographic assessments were also recorded: physician’s global assessment of the overall disease activity (physician global assessment) measured on a 10-cm visual analogue scale (VAS; 0 = no activity, 10 = maximum activity); parent’s global assessment of the child’s overall well-being on a 10-cm VAS (0 = very good, 10 = very poor); count of joints with active disease (ie, joints with swelling or, if no swelling was present or detectable, with restricted motion and either pain upon movement or tenderness) and count of joints with restricted motion;19 functional ability assessment through the Italian version of the Childhood Health Assessment Questionnaire (C-HAQ)20 (0 = best, 3 = worst) or, in the years earlier than 1994 (when the C-HAQ was published), through the Modified Lee Index21 or the Juvenile Arthritis Functional Assessment Report (JAFAR)22 (we previously found a high correlation between these three questionnaires when administered to the same patient on the same day);19 erythrocyte sedimentation rate (ESR; Westergren method); and Poznanski score of radiographic damage.23 24 Briefly, the Poznanski score is based on the measurement of the radiometacarpal length (RM) and of the length of the second metacarpal bone (M2). For each wrist, the number of standard deviations between the expected and the observed RM for the measured M2 is calculated. The Poznanski score reflects the amount of radiographic damage in the wrist. The more negative the Poznanski score is (that is, the shorter the RM is relative to the length of M2), the more severe the radiographic damage.
Assessment of therapeutic response at 6 months
The clinical response at 6 months after the beginning of MTX therapy was assessed by means of the ACR Pediatric definition of improvement,1 as above. Based on the level of response, patients were divided in four groups: (1) non-responders, (2) responders at 30%, (3) responders at 50%, and (4) responders at 70%. The three responder groups were mutually exclusive, that is: patients who achieved a 30% improvement, but did not reach the 50% threshold were placed in the 30% responder group; patients who achieved a 50% improvement, but did not reach the 70% threshold were placed in the 50% responder group; patients who achieved a 70% improvement were placed in the 70% responder group.
Assessment of long-term disease outcome
In each 6-month response group, long-term disease outcome was evaluated by calculating the percentage change in the count of active and restricted joints from baseline to 1 year, from baseline to 2 years, and from baseline to 5 years. Furthermore, the achievement of a state of inactive disease at 5 years after treatment start was assessed using the preliminary definition of clinical remission for JIA.25 At the same timepoint, the presence of the following single inactive disease parameters was assessed: physician global assessment = 0, active joint count = 0, restricted joint count = 0, C-HAQ = 0, and ESR<20 mm/h.
The following therapeutic interventions (if any) made in each patient by the attending physician between month 6 of MTX therapy and the 5-year assessment were recorded: ⩾50% increase in MTX dosage, start or dose increase of prednisone, introduction of a further second-line drug (combination therapy), introduction of a biologic agent, and intraarticular corticosteroid therapy.
Statistics
Descriptive statistics were reported in terms of medians and ranges for continuous variables and in terms of absolute frequencies and percentages for categorical variables. The percentage change in the active and restricted joint counts in the 0–1 year, 0–2 years, and 0–5 years intervals was computed by substracting the value of each joint count at 1, 2 and 5 years from the baseline value and by calculating the percentage of the change with respect to the baseline value. A negative change reflects improvement, whereas a positive change reflects worsening. Comparisons of quantitative variables among ACR Pediatric response groups were made by means of the non-parametric analysis of variance (Kruskal–Wallis test); the Dunn test was chosen as a posteriori test to assess the statistical significance of differences between pairs of patient groups. Comparison of qualitative data was performed by means of the χ2 test, or the Fisher exact test in case of expected frequencies less than 5. Bonferroni adjustment was applied as a correction for multiple comparisons to explore post-hoc differences between pairs of patients groups. All statistical tests were two sided; a p value of less than 0.05 was considered as statistically significant. The statistical package used was Statistica (StatSoft Corp., Tulsa, Oklahoma, USA).
RESULTS
Of the 185 JIA patients who were started with MTX in the study period, 139 had a follow-up of at least 5 years and were thus eligible for the study. Fourteen of these patients were excluded because they had insufficient clinical data available. The baseline clinical features of these patients were comparable to those of the 125 patients included in the study (data not shown).
Assessment of therapeutic response at 6 months
As it was our policy in the study period, all patients had the MTX dosage unchanged in the first 6 months of therapy. At 6 months after the beginning of MTX treatment, 42 patients (33.6%) were classified as non-responders, 24 patients (19.2%) were classified as 30% responders, 26 patients (20.8%) were classified as 50% responders, and 33 patients (26.4%) were classified as 70% responders. The baseline clinical features of the study patients divided by the ACR Pediatric response category at 6 months are shown in table 1. The four subgroups were comparable for all parameters, except for a tendency towards a greater representation of patients with systemic arthritis among non-responders and for a lower C-HAQ score among 30% responders.
Therapeutic interventions between 6 months and 5 years
Table 2 summarises the frequency of the therapeutic interventions made by the attending physicians between month 6 of MTX therapy and the 5-year visit in the four response groups. As expected, patients who were non-responders at 6 months received additional therapeutic interventions more frequently in the subsequent time period than did patients in the three responder groups, although the frequency of MTX dose increase was similar in non-responders and 30% responders. Among the three groups who had achieved an ACR Pediatric response at 6 months, the 30% responders had the MTX dosage increased more frequently than the 50% and 70% responders, whereas the two latter groups received more frequently intraarticular corticosteroid therapy. The mean duration of MTX therapy in non-responders, 30% responders, 50% responders and 70% responders was 4.3, 4.4, 4.3 and 4.1 years, respectively. At 5 years, 87 patients (69.6%) were still receiving MTX, whereas 38 patients (30.4%) had discontinued the drug (19 for disease remission, 8 for inefficacy, and 11 for side effects).
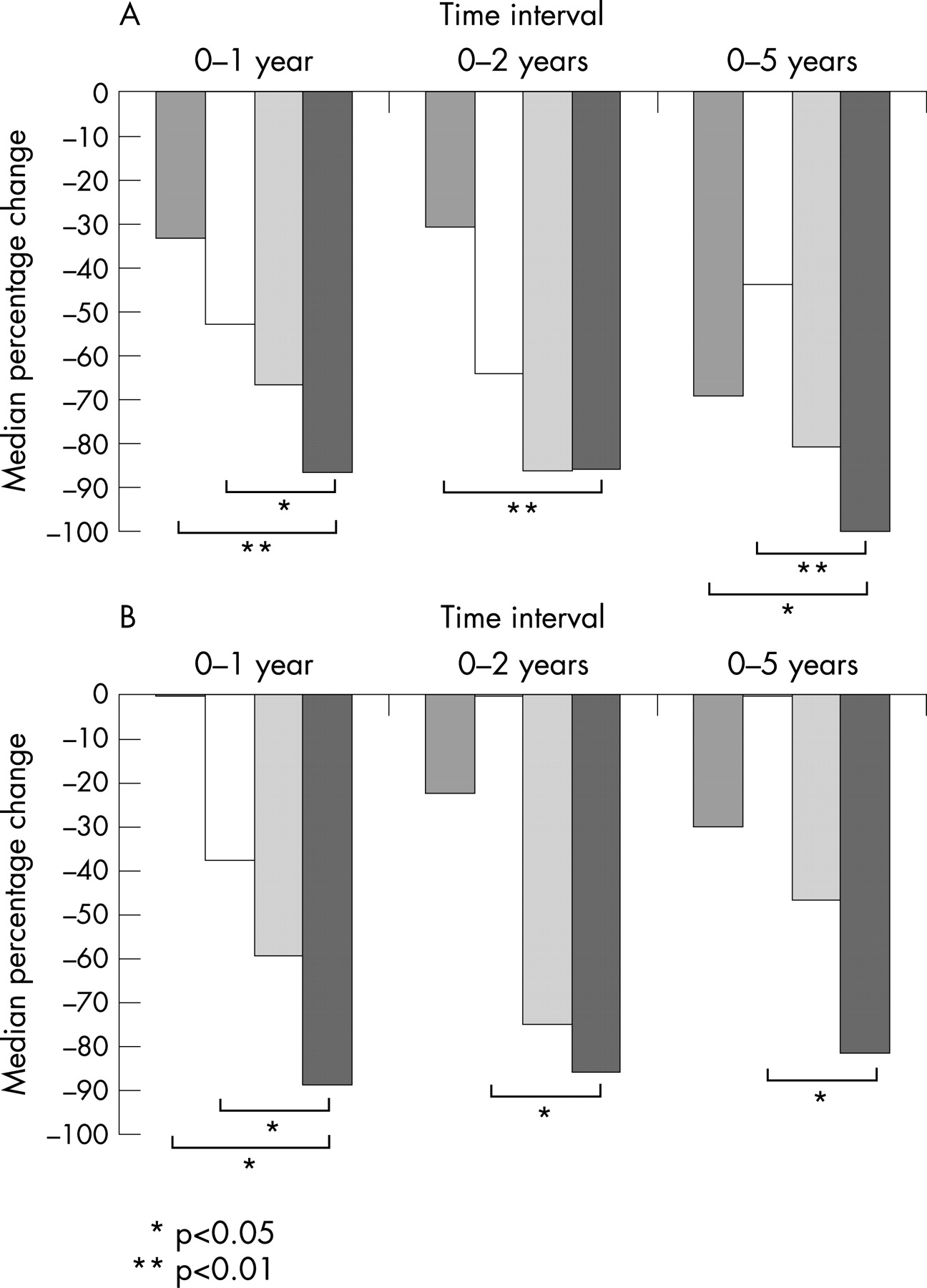
Long-term change in joint counts
The median percentage change in the active and restricted joint counts between baseline to 1 year, 2 years and 5 years in patients grouped according to the magnitude of ACR Pediatric response at 6 months is depicted in figs 1A and B, respectively. Patients who had achieved a 70% 6-month response showed a significantly greater and sustained change (improvement) in the number of active joints between baseline to 5 years compared with the non-responders and 30% responders. The 70% responders also showed a significantly greater and sustained improvement in the number of restricted joints between baseline to 5 years compared with the 30% responders.

{kind=link}
Frequency of inactive disease at 5 years
Table 3 shows the frequency of inactive disease parameters at 5 years after MTX start in the four response groups. Patients who had achieved a 70% response at 6 months had a greater frequency of all remission parameters at 5 years as compared with non-responders and 30% and 50% responders. Statistically significant comparisons included a greater frequency of an active joint count = 0, a normal ESR, and an inactive disease state23 in 70% responders than in 30% responders. There were no differences in the frequency of inactive disease parameters at 5 years between non-responders patients who had received (n = 10) or not received (n = 32) therapy with biologic agents (data not shown).
DISCUSSION
We investigated the relationship between the magnitude of the ACR Pediatric response in the first 6 months of MTX therapy and the 5-year disease outcome in 125 patients with JIA. Because in the study period it was our policy to start MTX in all JIA patients with polyarthritis who failed to respond to a course of non-steroidal anti-inflammatory medications, the study population is representative of the most severe cases of JIA who are candidates to receive a second-line drug therapy in a tertiary care pediatric rheumatology centre.
The ACR pediatric 30 response rate at 6 months after the beginning of MTX therapy was 66%, which is in the range of that reported in two controlled clinical trials of MTX in JIA (63% and 72%).2 3 Based on the magnitude of clinical improvement at 6 months, the 83 responders were placed in three mutually exclusive groups: 24 (19.2%) achieved a 30% response, 26 (20.8%) achieved a 50% response, and 33 (26.4%) achieved a 70% response; 42 (33.6%) patients were responders. Although we cannot exclude that the patients who experienced the greater levels of clinical improvement had a more benign disease, the clinical indicators of JIA severity at baseline were comparable across the four response groups. In the first 6 months of treatment, all patients were given MTX as monotherapy and had the dosage unchanged; the initial MTX dosage was comparable across the four response groups.
We found that patients who had achieved an ACR Pediatric 70 response at 6 months after MTX start experienced a significantly greater and sustained improvement from baseline to 5 years in the count of joints with active disease and restricted motion compared with those who were non-responders or had reached only the 30% response. The 70% responders also had a significantly greater frequency of indicators of inactive disease at 5 years compared with 30% responders. No differences in long-term outcomes were seen between 50% responders and non-responders or 30% responders. The analysis of the therapeutic interventions made by the attending physicians between month 6 of MTX therapy and the 5-year assessment revealed that the ACR Pediatric 70 responders were not given increased doses of MTX or other therapeutic interventions more frequently than the other response groups. By contrast (and as expected), therapeutic changes were more common in the non-responder group and in the group who had only a 30% response. These findings suggest that in our patient population only a 70% improvement in the core set measures after the first 6 months of MTX therapy made a real difference in terms of long-term disease outcome.
In recent years, the expectation of benefit of treatment of chronic arthritis, of either childhood or adult onset, has evolved. With the shift towards early aggressive therapy and the advent of the novel potent biologic medications, the lowest levels of therapeutic response (eg, the ACR Pediatric 30), are no longer considered sufficient; 50% responses are considered acceptable, but improvement of 70% or greater is now a goal for many clinicians.10 26 27 The US Food and Drug Administration (FDA) requires maintaining an ACR70 response for at least 6 months to consider an adult patient with rheumatoid arthritis to have achieved a major clinical response.28 Studies in adult patients with rheumatoid arthritis have shown that minimising disease activity over time reduces radiographic progression and improves long-term functional outcome.29 30 Our observation that the achievement of an ACR Pediatric 70 response after 6 months of MTX therapy was associated with a more favorable long-term disease outcome suggests that a 70% improvement should be set as the most meaningful target threshold in future clinical trials in JIA.
A number of potential limitations to the study must be acknowledged, the chief of which is its retrospective and non-controlled nature. A retrospective study is subject to missing and possibly erroneous data. Furthermore, the 14-year timeframe of our study (1986–2000) reflects for a large part a past era in the treatment of JIA, when low-dose MTX was the only available second-line medication whose efficacy had been formally demonstrated in a controlled trial2 and there was reluctance to increase MTX above the standard dose of 10 mg/m2/week owing to the concerns regarding its long-term toxicity.31 In recent years, there has been a major shift in the therapeutic approach of JIA. The traditional pyramid has been replaced with early aggressive intervention, and if major improvement does not occur within 3 months or so, the treatment is replaced or combined with other aggressive therapies, including higher doses of parenteral MTX and biologic agents, either alone or in combination with MTX.32 Nevertheless, our study is the first to investigate the relationship between early therapeutic response and long-term outcome in JIA and provides important clinical information that is useful to assess and interpret the effectiveness of the next generation of drugs proposed for use in children with JIA.
An important issue that arises from our analysis is that the potential for progression or therapeutic response that the disease displays in its early stages may be more important in predicting long-term outcome than the clinical characteristics at onset. We previously found that the early change in Poznanski score of radiographic damage was more powerful than baseline features in predicting long-term radiographic progression and physical disability in children with polyarticular JIA.22 These findings indicate that future investigations of long-term outcome in JIA should incorporate the early change in outcome measures and the degree of short-term therapeutic response in the list of potential predictors.
In conclusion, our results show that the achievement of an ACR Pediatric 70 response at 6 months after start of MTX therapy predicts a more favorable long-term disease outcome in patients with JIA. This finding suggests that the threshold level of meaningful clinical improvement in future clinical trials in JIA should be set at 70%, particularly when the efficacy of the novel (and costly) biologic medications is under evaluation.
REFERENCES
Footnotes
Competing interests: None declared.