Article Text

Abstract
Background: Poor adherence to treatment is difficult to diagnose accurately. Hydroxychloroquine (HCQ) has a long elimination half-life and its concentration in whole blood can be measured easily.
Objective: To evaluate the utility of a very low blood HCQ concentration as a marker of poor compliance in patients with systemic lupus erythematosus (SLE).
Methods: HCQ concentrations were determined on a blinded basis in 203 unselected patients with SLE. At the end of the study, the patients were informed of the results and retrospectively interviewed about their adherence to treatment.
Results: 14 (7%) patients said that they had stopped taking HCQ (n = 8) or had taken it no more than once or twice a week (n = 6). Their mean (SD) HCQ concentration was 26 (46) ng/ml. range (0–129 ng/ml) By contrast, the other patients had a mean HCQ concentration of 1079 ng/ml range (205–2629 ng/ml). The principal barriers to adherence were related to HCQ treatment characteristics. Adherence subsequently improved in 10 of the 12 patients whose blood HCQ concentrations were remeasured.
Conclusions: Very low whole-blood HCQ concentrations are an objective marker of prolonged poor compliance in patients with SLE. Regular drug assays might help doctors in detect non-compliance and serve as a basis for counselling and supporting these patients.
- HCQ, Hydroxychloroquine
- SLE, systemic lupus erythematosus
- SLEDAI, Systemic Lupus Erythematosus Disease Activity Index
Statistics from Altmetric.com
- HCQ, Hydroxychloroquine
- SLE, systemic lupus erythematosus
- SLEDAI, Systemic Lupus Erythematosus Disease Activity Index
Poor adherence to therapeutic regimens is a common and expensive problem in patients with chronic diseases and is difficult to diagnose.1 Rates of non-compliance in patients with systemic lupus erythematosus (SLE) range from 10% to 50%,2–,7 depending on the methods used to evaluate it; methods that are debatable.1 A simple, objective and reliable marker of non-compliance with medications in patients with SLE is needed.
Hydroxychloroquine (HCQ) is widely used in patients with SLE, and HCQ levels in blood can be quantified by high-performance liquid chromatography.8 We found in a recent study that several patients had undetectable blood HCQ concentrations.8 As HCQ has a long terminal elimination half-life, this finding implied that these patients had not taken HCQ for a long time. This result prompted us to evaluate the possibility of very low blood HCQ concentrations as a marker of poor adherence to treatment.
PATIENTS AND METHODS
Patients
This study cohort involved 203 unselected outpatients and inpatients receiving long-term follow-up from June 2000 to November 2004 at the Pitié-Salpêtrière Hospital, Paris, France (143 patients were included in a previous study).8 All patients met the American College of Rheumatology criteria for SLE, were treated with HCQ prescribed at a stable oral dose of 400 or 200 mg/day for at least 6 months, could easily contact their hospital physician if they developed symptoms of flare, had regular follow-up appointments at least every 6 months, were >15 years, not pregnant and had no serious ophthalmic disorders.
Study design
The study design has been described previously.8 All the patients were unaware that HCQ levels could be assessed until they attended our clinic, when they received information about the study, provided informed consent and had a first blood sample taken (day 0). No patient refused to participate in the study. SLE flares, defined by a Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score of >6 , were recorded on day 0 and throughout 6 months of follow-up for patients without flares on day 0, as detailed previously.8
Pharmacokinetic analyses
Blood collected at day 0 was analysed by high-performance liquid chromatography8 once the patient had completed the study.
Assessment and evaluation of non-compliance
Doctors provided their patients with the assay results and then interviewed them non-judgementally, which facilitated an open discussion.1 Patients were classified as non-compliant if they admitted that they had stopped HCQ or taken it only rarely in the weeks before day 0. Non-compliant patients were asked about the reasons for their non-compliance and about their compliance with other treatments for SLE during the same period.
Statistical analysis
Comparisons between non-compliant and other patients used the χ2 test or Fisher’s exact test for categorical variables and the Mann–Whitney U test for data with a non-normal distribution.
RESULTS
Blood HCQ levels and compliance
The study included 203 patients. Table 1⇓ reports their demographic and clinical characteristics and laboratory findings. Mean (SD) blood HCQ concentration on day 0 was 1007 (529) ng/ml. We found large interindividual variations for all patients and for comparisons limited to patients taking either 200 or 400 mg daily (fig 1⇓, table 1⇓).
Baseline demographic and clinical characteristics and laboratory measurements of the 203 patients with systemic lupus erythematosus (SLE), according to compliance status
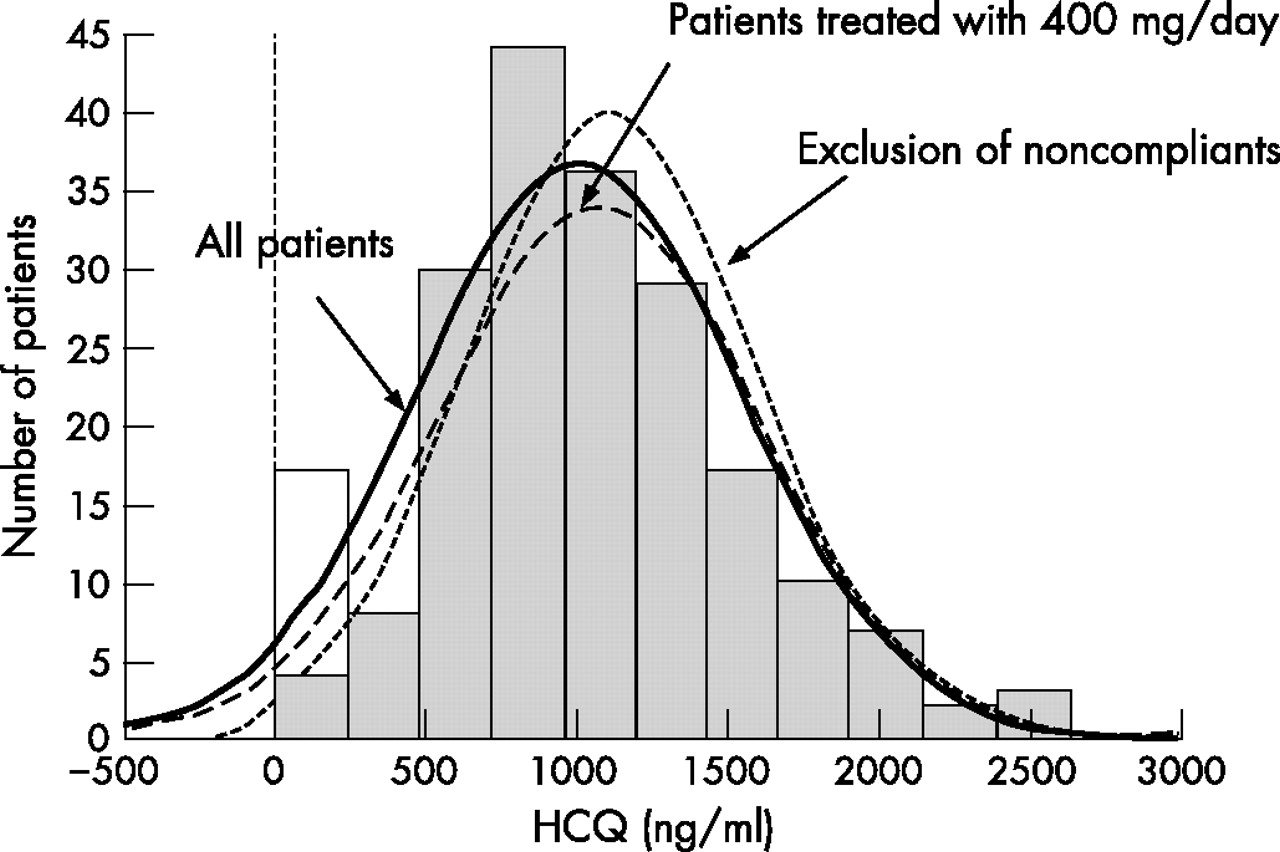
Distribution of whole-blood hydroxychloroquine (HCQ) concentrations. This figure demonstrates the clear Gaussian distribution of the blood HCQ concentrations in 203 unselected patients with systemic lupus erythematosus (SLE). Values of all patients (solid line), of patients treated with 400 mg/day HCQ (dashed line) and of the “other patients” (dotted line) have a Gaussian distribution. The variations in the right of the curve are considered to be the result of pharmacokinetic–pharmacodynamic factors (patients are usually not suspected to spontaneously increase their HCQ intake). Similarly, these factors probably explain the variations in the left of the curve. Non-compliant patients are represented in white histogram. HCQ concentrations ranged from 0 to 2629 ng/ml.
A total of 14 (7%) patients with SLE said that they had stopped taking HCQ (n = 8) or they took it no more than once or twice a week (n = 6). Mean duration of non-compliance was 17 months (range 1–56 months). Their mean (SD) HCQ concentration was 26 (46) ng/ml. Blood HCQ concentrations were undetectable in eight patients and ranged from 10 to 129 ng/ml in the other six patients.
All other patients reported either good adherence or only few omissions. Their mean (SD) HCQ concentration was 1079 ng/ml (range 205–2629 ng/ml).
Characteristics and indicators of non-compliance
Regarding demographic, clinical and laboratory variables, the only indicator of non-compliance was the SLEDAI score, which was higher on day 0, given the higher risk of ongoing SLE flare in non-adherent patients.
During the year before day 0, 12 of the 14 non-compliant patients had come regularly to their routine appointments, without missing any. None reported difficulties with adherence to treatment. All had regularly undergone their routine yearly electroretinogram from onset of HCQ treatment. Before the HCQ results were available, doctors suspected non-compliance in only 5 (36%) of these 14, owing to psychological or psychiatric troubles (n = 4) or absence of Cushing’s syndrome (n = 1). However, these five patients had always denied poor adherence.
Of these 14 patients, 10 also took corticosteroids, associated with immunosuppressive agents in 4. Four of them admitted poor compliance with these treatments.
Barriers to adherence
Patients attributed non-compliance to HCQ characteristics in 9 (64%) cases: four reported concern about potential side effects, three perceived HCQ to be ineffective compared with other treatments and two had experienced adverse side effects (vomiting and dizziness). Patient characteristics accounted for the remaining five cases of non-adherence: three admitted that they did not accept their disease and thought that they did not need treatment, one was “bored” with taking treatment, and another reported “forgetting” very frequently.
Course of non-compliance over time
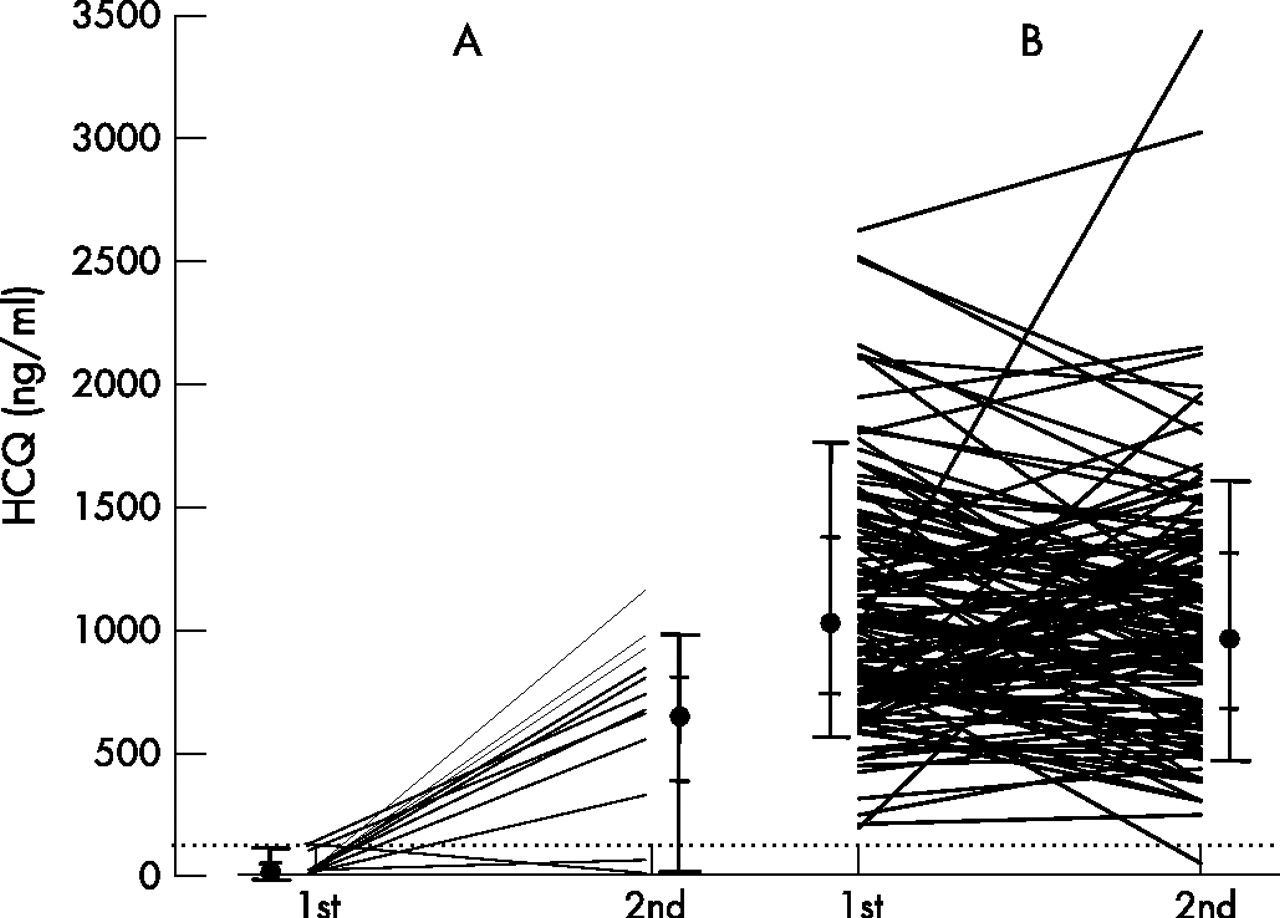
During the discussion with non-compliant patients, doctors again informed them about the benefit/risk ratio for HCQ treatment in SLE. In the months that followed, two patients decided to be treated in another hospital. The remaining 12 underwent a second unscheduled blood sample and HCQ assay, 13 (7) months later (fig 2⇓). Mean (SD) blood HCQ increased significantly, from 30 (49) ng/ml to 636 (354) ng/ml (range 0–1157 ng/ml; p = 0.001), but remained significantly lower that the mean blood HCQ concentration of the entire cohort (p = 0.01).

{kind=link}
{kind=link}
Whole-blood hydroxychloroquine (HCQ) concentrations over time according to compliance status. Blood HCQ concentrations were determined twice in some patients: first at day 0 and then after the completion of the study. (A) Includes the 12 patients non-compliant at day 0 who had two blood assays. Mean blood HCQ concentration increased between both samples. The mean interval between the blood samples was 13 (7) months. (B) Includes the 130 patients with blood HCQ concentration above our cut-off of non-compliance at day 0 who had 2 blood assays. The mean (SD) interval between the blood samples was 17 (13) months. The mean concentration did not differ significantly from that on day 0 (1043 (507) vs 1087 (490) ng/ml; p = 0.48). In this group, most patients remained in the same range of concentrations, but some considerably changed. Pharmacokinetic modifications may explain part of these variations: for example, the patient whose HCQ concentration increased from 1018 to 3438 ng/ml was treated with azathioprine when the first assay was performed and did not receive this treatment anymore when the second was done. A similar interaction has been found between azathioprine and warfarin.9 With regard to the patient whose HCQ concentration decreased from 830 to 47 ng/ml, she became non-compliant. Results are shown as individual data and as plots. For plots, the circles indicate the median, the small bars indicate the 25th (lower) and 75th (upper) centiles, and the long bars indicate the 10th (lower) and 90th (upper) centiles. The dashed line represents the cut-off for non-compliance.
Two patients reported continued non-compliance, one (HCQ concentration 0 ng/ml) because of persistent side effects and the other (56 ng/ml) because of persistent concern about ophthalmological risks.
For comparison, we subsequently assayed HCQ concentration in 130 of the other 189 patients: their mean concentration did not differ significantly from that on day 0 (fig 2⇑).
Non-compliance with HCQ treatment is strongly associated with SLE flares
At day 0, 7 of the 14 (50%) non-compliant patients had SLE flares, compared with 28 of the other 189 (15%) patients (p = 0.004).
During the 6-month follow-up period, 3 of the 7 (43%) non-compliant patients with inactive SLE at day 0 developed flares, a significantly higher flare rate compared with other patients with inactive SLE at day 0 (13/161; 8%; p = 0.02). Overall, 10 of the 14 (71%) non-compliant patients had active SLE (SLEDAI ⩾6) on either day 0 or during the 6 months afterwards.
DISCUSSION
Non-compliance with treatment is a major problem in the management of chronic diseases, but there is no satisfactory method of measuring compliance with medication.1,10,11 Patient self-reports, clinician’s assessments or suspicions, keeping appointments, pill count, the refilling approach and electronic monitoring devices that record the opening of the pill container are either disputable or not routinely applicable.1,11–,13 Objective methods, such as unscheduled blood or urine samples, are often limited by the unavailability or cost of sensitive assays, the frequent need for repeated sampling (due to the short half-life) and their inability to identify poor long-term compliance in patients whose compliance improves shortly before the doctors’ appointment (“white-coat compliance”).1,14 Because of its long terminal elimination half-life (>40 days), these limitations do not apply to blood HCQ assays.
Poor adherence was confirmed by 14 (7%) patients in the interviews, during which they were confronted with their blood HCQ levels. Their HCQ concentrations were <130 ng/ml, whereas all other patients had levels >205 ng/ml. This percentage is consistent with the 5–10% of patients who completely stopped or frequently interrupted tablet ingestion in studies using electronic monitoring.11,12
We were unable to identify any risk factors for, or indicators of, non-adherence except for ongoing SLE flares. Even if this may be attributable to the small number of patients, these results are consistent with previous studies that report conflicting results about these risk factors.1–6,15 As some have emphasised, “adherence is so difficult to diagnose because it is a task-specific behavior rather than a personality trait”.13
The doctors treating 9 (64%) of these 14 patients did not suspect non-compliance. This is not surprising as clinical judgment has been found wanting in almost every study in which it has been examined.1 The remaining five patients denied non-compliance until faced with the blood test result. This finding suggests that interviews without blood HCQ results are likely to be insufficient for diagnosing non-compliance.
The main barriers to patient compliance were due to HCQ treatment characteristics. After provision of new explanations, HCQ concentrations rose significantly in most patients, confirming that doctors’ awareness of non-compliance is an essential prerequisite for improving adherence.
The clinical consequences of non-compliance were substantial: very low blood HCQ concentrations at baseline were strongly associated with ongoing disease activity and, in patients with inactive SLE at day 0, with the risk of further SLE flares during the following 6 months. Even after exclusion of these 14 non-compliant patients, low blood HCQ concentrations remained significantly associated with SLE flares (data not shown), confirming our previous results.8
Two specific limitations of our study should be pointed out. First, two separate independent patterns of non-adherence have been described11—(a) relatively infrequently missed medication, and (b) complete stopping or frequently interrupted and erratic tablet intake—and low HCQ concentrations can identify only the latter. Patients who missed some medication had blood HCQ concentrations >205 ng/ml and were thus indistinguishable from those who reported good adherence. Another limitation of our study was the lack of objective assessment of non-compliance with other treatments.
In conclusion, these findings strongly suggest that unscheduled, regular assays of HCQ levels in whole blood are a reliable, simple and objective method for identifying non-adherent patients with SLE: undetectable or unexpectedly low HCQ concentrations should prompt a non-judgemental discussion with the patient. Determination of blood HCQ concentration, available within few days in our centre, may be helpful for doctors confronted with a flare as it may prevent incorrect interpretation of poor compliance as a lack of response, and lead to unnecessary or even dangerous regimen escalation. HCQ assays may also help to prevent SLE flares by detecting non-compliant patients with currently inactive SLE who are at high risk of further flares and by making it possible to conduct specific interventions to improve their compliance.
REFERENCES
Footnotes
Published Online First 23 February 2007
Competing interests: None.