Article Text

Abstract
Objective: To estimate the disease activity score (DAS)28-C-reactive protein (CRP) threshold values that correspond to DAS28-erythrocyte sedimentation rate (ESR) values for remission, low disease activity and high disease activity in patients with rheumatoid arthritis.
Methods: DAS28 data were analysed using a large observational study (Institute of Rheumatology Rheumatoid Arthritis) database of 6729 patients with rheumatoid arthritis. Firstly, the relationship between the DAS28-ESR and the DAS28-CRP values was analysed. Secondly, the best DAS28-CRP trade-off values for each threshold were calculated using receiver operating characteristic (ROC) curves.
Results: The correlation coefficient of ESR versus CRP was 0.686, whereas that of DAS28-ESR versus DAS28-CRP was 0.946, showing the strong linear relationship between DAS28-ESR and DAS28-CRP values. DAS28-CRP threshold values corresponding to remission, low disease activity and high disease activity were 2.3, 2.7 and 4.1, respectively. The sensitivity and specificity from the ROC curves were gradually reduced as DAS28 values became lower.
Conclusions: This study showed that DAS28-CRP and DAS28-ESR were well correlated, but the threshold values should be reconsidered. As the results were derived from only Japanese patients, it is essential to compare DAS28-CRP threshold values in people of other ethnic groups.
- CRP, C-reactive protein
- DAS, Disease Activity Score
- ESR, erythrocyte sedimentation rate
- ROC, receiver operating characteristic
- VAS, visual analogue scale
Statistics from Altmetric.com
- CRP, C-reactive protein
- DAS, Disease Activity Score
- ESR, erythrocyte sedimentation rate
- ROC, receiver operating characteristic
- VAS, visual analogue scale
Although the development of new classes of therapeutic agents for the treatment of rheumatoid arthritis has provided a subset of patients with relief from pain and disability in recent years, doctors still require a reliable evaluation system for patients that allows the effects of these agents to be accurately assessed. The Disease Activity Score1 uses 28 joint counts (DAS28)2 and has been widely used in clinical trials and for the assessment of patients in the clinic to monitor disease activity of patients with rheumatoid arthritis.3–6
The DAS28 is calculated from four components: tender joint count, swollen joint count (both performed by the treating doctor), visual analogue scale (VAS) score of the patient’s global health and the laboratory parameter erythrocyte sedimentation rate (ESR). The DAS28 is widely used, and cut-off points of 2.6, 3.2 and 5.1 have been proposed to be indicative of remission, low disease activity and high disease activity, respectively.
Recently, a DAS28 based on C-reactive protein (CRP) levels rather than ESR has been suggested. Although the formula for calculating DAS28-CRP values was designed to produce equivalent results to those of the DAS28-ESR, DAS28-CRP values seem to be lower than DAS28-ESR values in clinical practice. Because changes in ESR and CRP levels represent different underlying pathophysiologies, the DAS28-CRP threshold values might be expected to differ from those of the DAS28-ESR. Nevertheless, few studies have been performed to validate and/or compare these two systems. In this study, we have evaluated the DAS28-CRP threshold values that correspond to criteria for remission, low disease activity and high disease activity according to the DAS28-ESR.
METHODS
Participants
We used DAS28 data from the database of a large rheumatoid arthritis observational study (Institute of Rheumatology Rheumatoid Arthritis)7,8 conducted at the Institute of Rheumatology, Tokyo Women’s Medical University, Tokyo, Japan. All patients with rheumatoid arthritis in our institute since 2000 were registered in the Institute of Rheumatology Rheumatoid Arthritis cohort, and systematic data have been collected biannually. In this study, data from 6729 patients with rheumatoid arthritis who participated in surveys conducted between October 2000 and April 2004 were used. Eight patient surveys were conducted during this period, and the latest data for each patient were used in this analysis.
Laboratory values
Blood samples from all patients were measured on-site. ESR was determined by Westergren methods. CRP levels were measured by a standard method using a latex agglutination turbidimetric immunoassay. The CRP detection level was >0 (mg/dl).
Statistical analysis
As DAS28 values were normally distributed, we described them using mean (SD), whereas all other variables were described using median (25th centile, 75th centile). For the same reason, Pearson’s correlation was calculated for DAS28-ESR and DAS28-CRP, whereas Spearman’s rank correlation was used for ESR and CRP. To show relationships between DAS28-CRP and DAS28-ESR values, scatter plots with linear regression line were drawn. Receiver operating characteristic (ROC) curves were constructed to assess the cut-off points of DAS28-CRP values that correspond to DAS28-ESR scores of 2.6, 3.2 and 5.1, respectively. Each cut-off point was calculated on the basis of the best trade-off values between sensitivity and specificity as follows: (sensitivity+specificity)/2. The credibility of each cut-off point was also evaluated with respect to sensitivity and specificity (table 1).
Corresponding Disease Activity Score (DAS)28-erythrocyte sedimentation rate, DAS28-C-reactive protein, sensitivity and specificity values derived from the receiver operating characteristic curves for each criterion
RESULTS
Patient characteristics
A dataset of 6729 patients was used for this analysis: 82.1% female; age, 60 (51, 68) years old; rheumatoid arthritis duration, 9 (5, 16) years; rheumatoid factor positivity 77.3%; tender joint count (28 joints), 1 (0, 3); swollen joint count (28 joints), 1 (0, 3); VAS-GH (global health), 31 (12, 56) cm; ESR, 29 (15.7, 49.2) mm/h; CRP, 0.6 (0.2, 1.6) mg/dl; DAS28-ESR, 3.7 (1.3); DAS28-CRP, 3.1 (1.21). A total of 45.6% of the patients were treated with methotrexate and 0.342% were receiving biological treatments.
Relationship between DAS28-ESR and DAS28-CRP values
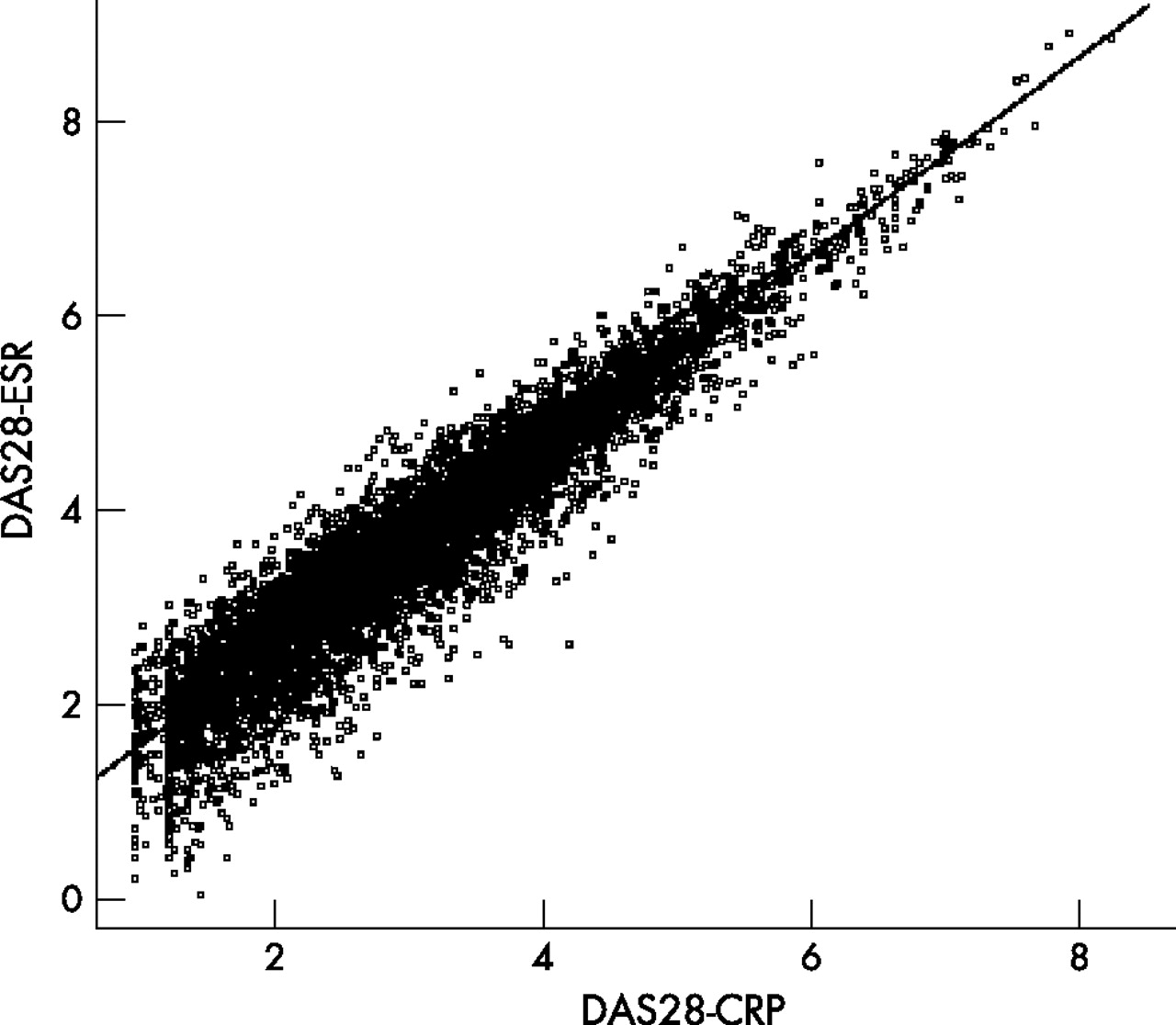
The correlation coefficient of ESR versus CRP was 0.686 and that of DAS28-ESR versus DAS28-CRP was 0.946, indicating that the DAS28-ESR and DAS28-CRP were strongly linearly correlated, suggesting that the DAS28-CRP can be used as an alternative to the DAS28-ESR. Both DAS28-ESR and DAS28-CRP scores were distributed normally (data not shown); however, DAS28-ESR and DAS28-CRP scores exhibited slightly different distributions, with the peak of the DAS28-CRP distribution being to the left of that of the DAS28-ESR. Figure 1 shows the scatter plot of DAS28-ESR and DAS28-CRP scores with the regression line (DAS28-ESR = 1.01×(DAS28-CRP)+0.590). The residuals were distributed widely at the lower DAS28 values, with the correlation between DAS28-ESR and DAS28-CRP scores being relatively weak at these lower values. This tendency was also confirmed using Bland–Altman plotting9 (see supplementary fig A online at http://ard.bmjjournals.com/supplemental).

Scatter plot of Disease Activity Score (DAS)28 C-reactive protein (CRP) (x axis) versus DAS28-erythrocyte sedimentation rate (ESR) (y axis) values with a regression line. Each point shows a single patient’s data. The slope and intercept of the regression line were 1.01 and 0.59, respectively.
DAS28-CRP threshold values
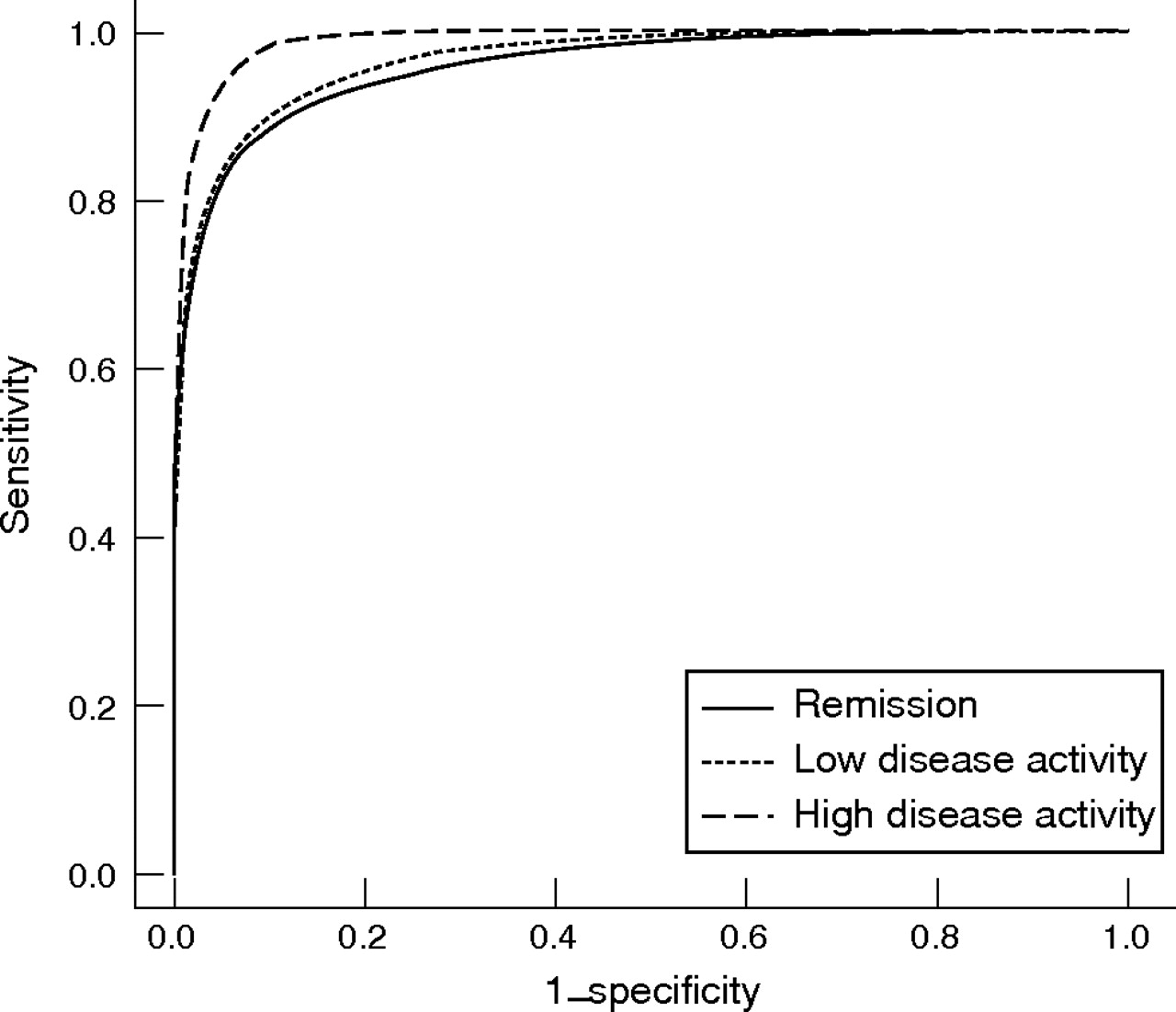
Figure 2 shows the ROC curves for DAS28-CRP values that corresponded to the DAS28-ESR values of 2.6, 3.2 and 5.1. The area under the ROC curves was 0.960 for remission, 0.967 for low disease activity and 0.989 for high disease activity. The best trade-off DAS28-CRP values corresponding to DAS28-ESR values of 2.6, 3.2 and 5.1 were 2.3 (sensitivity 92.1%; specificity 86.9%), 2.7 (sensitivity 90.8%; specificity 89.3%) and 4.1 (sensitivity 92.5%; specificity 97.0%), respectively.

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves of Disease Activity Score (DAS)28-C-reactive protein values corresponding to DAS28-erythrocyte sedimentation rate remission, low disease activity and high disease activity. The best trade-off values were calculated through the contact point of the ROC curve and line with slope = 1 at which the sum of sensitivity and specificity was the highest.
DISCUSSION
Using a ROC curve analysis of data from a large observational study of patients with rheumatoid arthritis in Japan, we estimated DAS28-CRP threshold values corresponding to DAS28-ESR remission, low disease activity and high disease activity to be 2.3, 2.7 and 4.1, respectively. As each of these threshold values is lower than the corresponding DAS28-ESR threshold values, disease activity in patients with rheumatoid arthritis may be underestimated if the DAS28-CRP is used, potentially diminishing or eliminating the capacity of therapeutic strategies designed to tightly control disease activity. Therefore, caution must be exercised when using the DAS28-CRP.
Considering the strong linear relationship between DAS28-ESR and DAS28-CRP values (correlation coefficient 0.946), we suggest that the DAS28-CRP can be used as an alternative to the DAS28-ESR and would be useful in situations in which only CRP data are available. CRP measurements are widely used in the routine evaluation of several inflammatory diseases, further supporting the notion that utilisation of the DAS28-CRP may be beneficial in clinical practice of rheumatology. However, because our cohort consists of Japanese patients with rheumatoid arthritis, multicultural comparisons are required to determine whether the DAS28-CRP can be used as an alternative to the DAS28-ESR in people of other ethnic groups.
From the residuals distribution and sensitivity/specificity derived from ROC curves, we found a relatively large fluctuation in the correlation of lower DAS28-ESR and DAS28-CRP values. This may have been caused by the difference in the distribution profile of DAS28-ESR and DAS28-CRP scores, as the DAS28-CRP exhibited a slightly skewed distribution toward the left compared with the DAS28-ESR. Consequently, the sensitivity and specificity of remission and low disease activity criteria were lower than those of high disease activity. Inconsistency of DAS28-ESR remission criteria and of Pinals’s criteria have been noted elsewhere,10 suggesting that the DAS28 system itself may have some inherent uncertainty when lower values are considered. When the proposed threshold values for the DAS28-CRP were used in this study, the frequency of misclassification between the DAS28-ESR and the DAS28-CRP was 6.9% in patients with high disease activity and 11.2% in those in remission. Hence, when making clinical decisions based on remission or low disease activity criteria using the DAS28-CRP in the place of the DAS28-ESR, we should consider this divergence between these scoring systems.
In conclusion, we have evaluated the threshold values of the DAS28-CRP that correspond to DAS28-ESR values for remission, low disease activity and high disease activity criteria (2.3, 2.7 and 4.1, respectively) in Japanese patients with rheumatoid arthritis. Further study is required to determine the applicability of this scoring system in people of other ethnic groups and in those who fulfil remission or low disease activity (rather than high disease activity) criteria.
Acknowledgments
We thank Professor Gurkirpal Singh, Stanford University, Palo Alto, USA, for useful discussions.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Funding: This study was financially supported by the research-consortium of 32 pharmaceutical companies.
-
Competing interests: None declared.
-
Published Online First 22 August 2006