Article Text

Abstract
The systemic vasculitides are multisystem disorders with considerable mortality and morbidity and frequent relapses. In the absence of reliable serological markers, accurate clinical tools are required to assess disease activity and damage for treatment decisions, and for the performance of clinical trials. This article reviews and summarises the development and use of disease assessment tools for determining activity and damage in systemic vasculitis and reports ongoing initiatives for further development of disease assessment tools. A literature search was conducted using PubMed and reference lists for vasculitis, assessment, clinical trials, outcome and prognosis. The findings indicate that comprehensive disease assessment in vasculitis requires documentation of disease activity, chronic irreversible damage and impairment of function.
- ANCA, antineutrophil cytoplasmic antibody
- BVAS, Birmingham Vasculitis Activity Score
- BVAS/WG, Birmingham Vasculitis Activity Score for Wegener’s granulomatosis
- DEI, Disease Extent Index
- EUVAS, European Vasculitis Study Group
- FFS, Five Factor Score
- ITU, intensive treatment unit
- OMERACT, Outcome Measures for Arthritis Clinical Trials
- VDI, Vasculitis Damage Index
Statistics from Altmetric.com
- ANCA, antineutrophil cytoplasmic antibody
- BVAS, Birmingham Vasculitis Activity Score
- BVAS/WG, Birmingham Vasculitis Activity Score for Wegener’s granulomatosis
- DEI, Disease Extent Index
- EUVAS, European Vasculitis Study Group
- FFS, Five Factor Score
- ITU, intensive treatment unit
- OMERACT, Outcome Measures for Arthritis Clinical Trials
- VDI, Vasculitis Damage Index
In several complex rheumatic diseases, measurement of disease morbidity is becoming increasingly important. Patients with rheumatoid arthritis, lupus and vasculitis are expected to live for many years, but they also have frequent episodes of relapse, accumulation of damage and drug toxicity.1–3 In this context, indices of clinical disease assessment have become necessary because of the failure of serological markers to provide accurate information to stage patients for appropriate treatments. In rheumatoid arthritis, the widespread use of the Disease Assessment Score4 provides an international comparison among patients as a basis for clinical trials.5,6 In systemic lupus erythematosus, the British Isles Lupus Assessment Group index and other indices have been developed to measure disease activity.7 Disease activity in lupus has been separated from damage (non-healing scars) using the Systemic Lupus International Cooperating Clinics Index.8 In vasculitis, the Birmingham Vasculitis Activity Score (BVAS)9 and other similar scores have been applied to assess disease activity, whereas the Vasculitis Damage Index (VDI)10 provides information on disease damage.
The objective of all scores is to provide a detailed description of the clinical status of patients with chronic rheumatic diseases. The information gathered during clinical evaluation of patients with vasculitis can be transformed into a variety of quantitative scores that may provide a justification for treatment decisions; the same information may be used to give an indication of prognosis, and an extension of this would be to stratify treatment according to probable outcome.
DISEASE ASSESSMENT MEASURES
Several groups have independently approached the problem of multisystem clinical evaluation in systemic vasculitis. A comparison of the underlying dataset of different disease assessment tools in current use suggests that by consensus, clinicians mostly agree on clinical symptoms and signs that represent disease activity in vasculitis treatment decisions (table 1).
Assessment tools and websites
An alternative view of clinical evaluation of patients with systemic vasculitis is that each disease should have its own unique dataset. However, there is considerable evidence that patients with different forms of primary small-vessel or medium-vessel vasculitis share common features.11,12 Intuitively, the common generic dataset should be used with the understanding that not all aspects of the dataset are required in every patient. Indeed, the major European Vasculitis Study (EUVAS) Group trials have grouped together the antineutrophil cytoplasmic antibody (ANCA)-related small-vessel vasculitides for the purposes of treatment and analysis.13 Further, there are a large number of patients in whom a specific diagnostic label cannot be applied and yet who clearly fulfil a diagnosis of vasculitis.14,15
Early measures
Early development of disease activity measures such as the Groningen Index16 for Wegener’s granulomatosis were based on the clinical features of disease with additional laboratory support. The dependence on biopsy findings for evidence of active vasculitis, which is entirely appropriate at diagnosis, made this an impractical tool for use in the follow-up of patients. The Baltimore Group developed a vasculitis activity index, which consists of a rating scale of disease in several organ systems.17 This introduces a possible observer bias and is not widely used.
THE BIRMINGHAM VASCULITIS ACTIVITY SCORE
The current standard assessment tool for scoring disease activity in systemic vasculitis is the BVAS.9 The important principle that applies to all assessment measures is to ensure that an abnormality is recorded only when it is attributed to active vasculitis. The reason for this important distinction is that many of the features that occur in vasculitis could equally occur as a result of other causes. For example, the presence of haematuria could be due to vasculitis, urinary infection or cyclophosphamide bladder toxicity.
After initial validation in patients with vasculitis in a variety of disease states, the first version of BVAS was published in 1994.9 Since then, the list of clinical features has been revised for use in European vasculitis studies by the EUVAS by omitting four of the initial items that were thought to occur only rarely and by adding seven new items including features available after specialist (eg, ophthalmology) opinion and tests.18 Altogether, 66 clinical features are included. These items are grouped into nine different organ systems. Each item is given an arbitrary numerical value according to its perceived clinical relevance. For example, nasal crusting carries a value of 2 whereas haematuria has a value of 6. The different organ systems are also weighted according to clinical relevance by applying maximal scores for each system. For example, ENT has a maximal score of 6, whereas the renal system has 12. In the latest version of BVAS called BVAS 2003, which is currently undergoing validation, the list of the clinical features has been further revised (fig 1). Four new items have been added, four items of low specificity for vasculitis have been omitted and items that are due to the same underlying pathological process have been grouped together. Figures 2 and 3 give details of the glossary and scoring in the BVAS 2003.
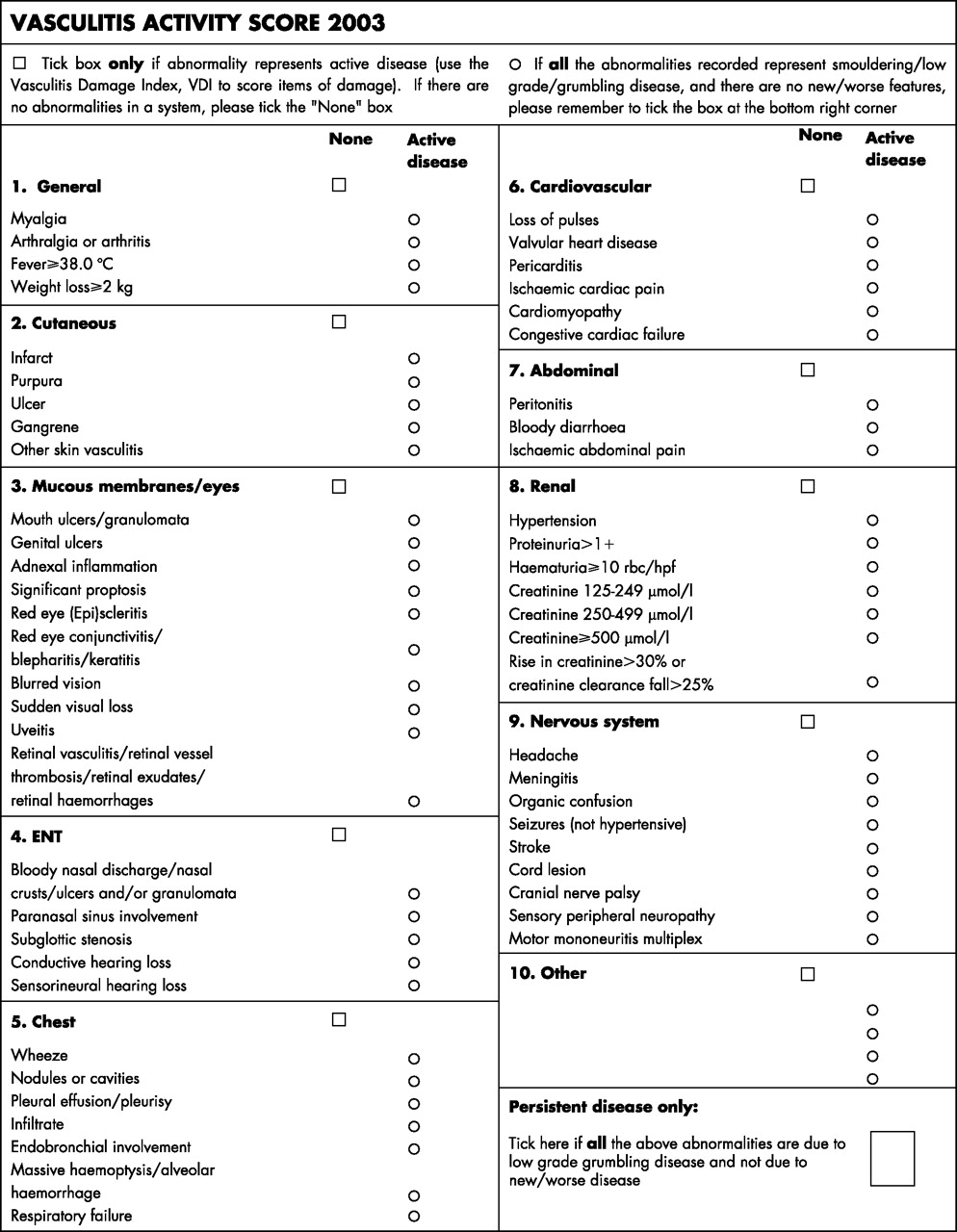
(A)Vasculitis activity score 2003.

Glossary and scoring for the BVAS 2003 (general, cutaneous, mucous membranes/eyes and ENT). CT, computed tomography; MR, magnetic resonance.

Glossary and scoring for the BVAS 2003 (chest, cardiovascular, abdominal, renal, nervous system, other). CT, computed tomography; MR, magnetic resonance; RBC, red blood cells; VDI, Vasculitis Damage Index.
Without specific training in the use of BVAS, even doctors who were experienced at managing vasculitis struggled to use the score as originally intended. The result was wide interobserver variation, which improved dramatically after group discussion and a better appreciation of the nature of the score. Areas of greatest contention were of two varieties. Firstly, there was a tendency to overscore patients who had established fixed lesions such as stroke or chronic kidney disease, which appeared as items on the BVAS list but did not represent new or worsening disease or even grumbling disease. The second area of controversy was related to the distinction between active vasculitis and infection, especially in the upper airways. As a result of some of these discussions, a glossary of terms was developed for the BVAS and published along with the new version of the assessment tool,19 emphasising the requirement to score an item only if it is due to active vasculitis based on clinical judgement.
In the next phase of development of the BVAS, the International Network for Study of Systemic Vasculitis reviewed and revised the BVAS for use in a clinical trial of patients with Wegener’s granulomatosis. This tool is called the Birmingham Vasculitis Activity Score for Wegener’s granulomatosis (BVAS/WG).20 The focus of the trial was on Wegener’s granulomatosis, and features that were less common or absent in Wegener’s granulomatosis were therefore omitted. Items due to similar pathological processes were merged and new items more specific for Wegener’s granulomatosis (eg, endobronchial disease) were introduced. The arbitrary weighting in the original BVAS was reviewed and changed, with a further arbitrary weighting assigning one point to any item judged to be of a minor nature and three points to any item of a major nature. A major item was one that would normally require the clinician to introduce aggressive treatment such as cyclophosphamide, whereas a minor item required an increased dose of steroids or the introduction of a less toxic immunosuppressant such as methotrexate. The BVAS/WG was supplemented by a visual analogue scale of physician’s global assessment of disease activity and an opportunity to assign patients to specific disease states of remission, minor flare or major flare. The BVAS/WG was validated and introduced for the purposes of that particular clinical trial, and has the advantage of greater disease specificity over the original BVAS in patients with Wegener’s granulomatosis; however, is has not been validated outside this specific disease, and therefore cannot be recommended for general use.20
Grumbling disease
An apparent problem in the initial use of the BVAS was how to record low grade or “grumbling” disease activity. Some patients, although clearly improving on treatment, have ongoing low-grade manifestations of vasculitis, which are usually not thought to warrant an intensification of treatment. The original score included only clinical features that were either new or worse in the month before the assessment. For this reason, a second column, labelled BVAS2, was added when the original score was revised by the EUVAS Group (in addition to the first column that is used to record the presence of new or worsening features of vasculitis).21 However, the addition of the BVAS2 led to confusion among researchers. It was often impossible to distinguish between ongoing symptoms due to active vasculitis and symptoms due to scarring without an underlying active vasculitic process. For this reason, the separate BVAS2 column has been omitted from the BVAS 2003 version. In this version, there is the opportunity to record “persistent only disease” if all positive items are thought to be due to active but not new or worse disease activity. This certainly does not provide a final answer for this intractable problem. However, there is a limit on how much complexity can be introduced without the tool becoming too clumsy to be useful in practice.
Clinical trials
The BVAS has been used in >10 published therapeutic trials on vasculitis by various groups over the past 5 years22–31 (table 2). It has become the standard disease activity measure in clinical trials on patients with various forms of vasculitis and for the development of serological markers of disease activity, and it has stood the test of time.
Use of Birmingham Vasculitis Activity Score and Birmingham Vasculitis Activity Score for Wegener’s granulomatosis in clinical trials
In comparatively rare diseases such as the vasculitides, it is highly desirable that a single standard structured clinical disease activity measure is used, in order to allow comparisons between different studies.
The BVAS has also been shown to have prognostic value, at least in short- to medium-term mortality, which makes clinical sense. The relationship between initial disease activity and subsequent risk of mortality is probably going to become less clear over time. Damage measures are possibly better at predicting long-term outcome. In one cross-sectional study of 213 consecutive patients, mortality occurred only in patients with an initial BVAS >8.9 In a retrospective series of 278 patients, BVAS was markedly higher in a patient who subsequently died than in survivors.34 Although no separate analysis was performed, it seemed that the greatest divergence in the Kaplan–Meier survival curves was in the initial 18 months. In another retrospective analysis of 26 patients in the intensive treatment unit (ITU), the BVAS at the time of admission to the ITU was predictive of survival at the end of follow-up after a mean of 31.4 months but not predictive of survival in the ITU.35 However, other retrospective studies did not confirm a prognostic value of baseline BVAS for survival after a mean follow-up of 56.5 and 26 months in 56 and 99 patients with vasculitis, respectively.36,37 A large prospective study is under way to resolve this issue.
Future development
Evolution of BVAS is necessary, just as in any clinical tool where there is no gold standard. The cycle of design followed by implementation, evaluation, redesign and further testing is constant, which means that we will never have a perfect instrument, but each cycle will lead to data-driven improvement. These principles are applied to many of the clinical measures tested by the Outcome Measures for Arthritis Clinical Trials (OMERACT) Consensus Group.38 The next phase of development for the BVAS is to draw together some of the lessons from the previous versions and improve the instrument. Current discussions in the OMERACT Group39 are designed to resolve these problems.
OTHER DISEASE MEASURES
The Disease Extent Index (DEI) scores the number of organ systems affected, is unweighted and correlates with the BVAS.40 It complements the BVAS in that a combination of both scores shows whether, for example, a high BVAS is due to severe manifestation in only one organ system or is due to multisystem disease.
The Five Factor Score (FFS)41 was developed using the prognostic value on outcome of different clinical features in a large number of patients with polyarteritis nodosa and Churg–Strauss syndrome. Five relevant risk factors at presentation for poor prognosis were derived from the data (renal impairment, proteinuria and involvement of the cardiovascular, gastrointestinal and central nervous systems). The FFS provides a useful prognostic index in these two diseases and may be of value for prognosis of other diseases, but it has not been widely tested in patients with Wegener’s granulomatosis or microscopic polyangiitis. Its effectiveness in distinguishing outcome has led investigators to use the FFS score at the onset to determine the treatment strategy chosen. The FFS and the DEI can be derived from the dataset recorded for the BVAS.
A recent comparison of the BVAS, BVAS/WG, BVAS 2003 and DEI showed a good correlation among these different indices.42 As all these tools use more or less the same disease features to record activity, it was suggested that differences in the arbitrary weighting of individual items was not of major importance. This topic is being actively investigated by the OMERACT Group.
DEFINING DISEASE STATUS
Definitions of disease status are an important requirement to measure the effectiveness of different treatments in clinical trials. The loose clinical definitions of remission, relapse and partial remission used in previous studies are no longer satisfactory. These definitions need to be more precise and more reproducible so that they can be standardised. The EUVAS Group has used definitions based on the BVAS in their clinical trials.21
International discussions are under way to arrive at agreed definitions of different disease states. Table 3 summarises some of the potential roles of disease assessment tools in systemic vasculitis.
Role of disease assessment in systemic vasculitis
Damage assessment in vasculitis
Damage caused by vasculitis or its treatment may ultimately prove more troublesome than disease activity to the individual patient. Damage is defined as a non-healing scar that is unlikely to respond to immunosuppressive treatment.
Recurrent and persistent disease activity is largely responsible for the damage caused to patients with Wegener’s granulomatosis. In the longitudinal Wegener’s granulomatosis cohort from the National Institutes of Health, 86% of patients had permanent damage as a consequence of the disease itself and 42% had treatment-related morbidity. This damage included, for example, end-stage renal disease, chronic pulmonary dysfunction, diminished hearing, saddle-nose deformities, blindness and death.43
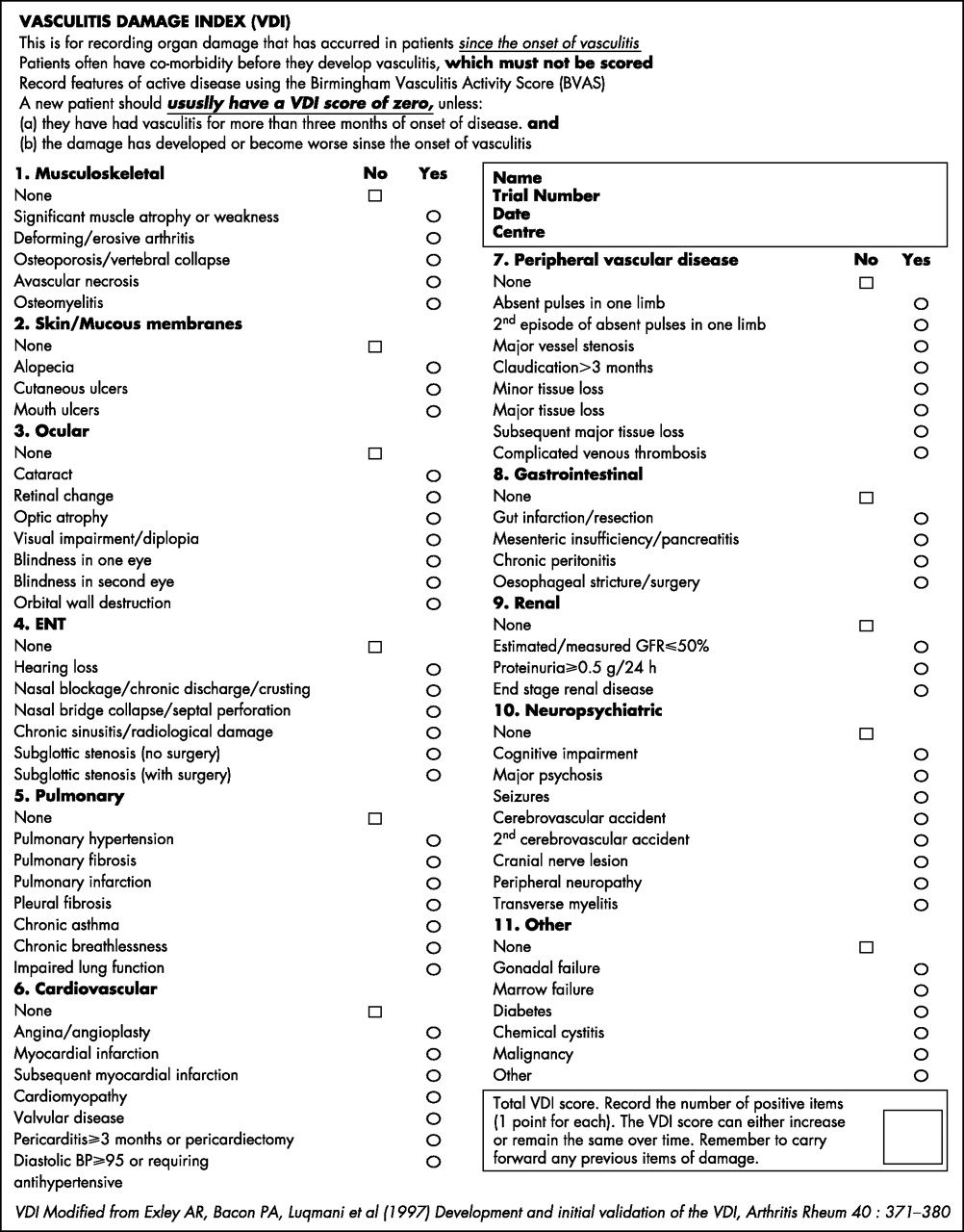
The VDI is comprised of 64 items of damage (grouped into 11 organ-based systems) defined by a consensus of experts to represent forms of damage occurring in patients with systemic vasculitis (fig 4). As the clinical distinction between activity and damage may be challenging, it is helpful to define damage over time—that is, if a disease manifestation does not respond to appropriate treatment for a certain time, then it should be scored as damage. In the VDI, damage was defined as an irreversible scar lasting >3 months. In the case of defined events, such as gut resection (which is inherently irreversible), scoring was deferred for 3 months to ensure consistency. Items of damage were not weighted. All damage that occurred after the onset of the first symptoms related to the vasculitis was scored, regardless of attribution (to avoid introducing yet another layer of variability). Finally, the VDI was constructed to be a cumulative index; therefore, the VDI score could not decrease over time.44

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Vasculitis Damage Index.
Use of the VDI in patients with vasculitis has shown that the accumulation of damage is bimodal, with an earlier phase due to the vasculitis itself, and a later phase due to treatment. A high BVAS and BVAS/WG at presentation is predictive of a higher eventual VDI score.33,45 The early phase accounts for most damage in patients. Early damage is predictive of mortality. A retrospective study showed that 2 years after diagnosis, a 6-month VDI score >4 was associated with an odds ratio of 12.4 for mortality (95% confidence interval 4.2 to 36.9).46 Patients who died had more organ systems involved and a higher total VDI score when measured after 2 years of disease compared with those having non-fatal vasculitis.10 A baseline VDI score ⩾1 was strongly predictive of mortality after a median follow-up of 56.5 months in a retrospective analysis of 56 patients with Wegener’s granulomatosis.37
Future developments
The VDI provides the vocabulary and framework to describe the longer-term outcomes in patients with vasculitis. The VDI remains an important outcome for clinical trials; it allows a record to be made of the natural history of treated disease, it enables clinicians to record abnormalities in patients and also assists in the separation of disease activity items that warrant immunosuppression from damage items that do not warrant immunosuppression. The current damage index concepts may need to be revised in the light of use. Irreversibility of all items may not be appropriate, especially if the clinical effects have completely disappeared. The scoring of damage irrespective of attribution could be challenged. It would be helpful to examine the prognostic value of specific items that are either related or not related to disease or its treatment. The index does not involve any specific weighting of items, although subgroups of items may provide subindices. Exploring gradation of damage—for example, the severity of renal impairment rather than the presence or absence of a considerable renal impairment—may be valuable.
TRAINING TO USE DISEASE ASSESSMENT SCORES
Training has become an essential part of any of these assessment packages. Our early experiences within the EUVAS Group showed that even in clinicians who were experienced in managing vasculitis, the consensus between observers for assessing the BVAS and VDI scores was very poor. However, after training there was a dramatic improvement in observer agreement.47
QUALITY OF LIFE AND SOCIOECONOMIC COSTS
Systemic vasculitis leads to a major impairment in the quality of life48,49 and carries a high socioeconomic burden.50 The measures for physical and mental health at diagnosis are markedly impaired in patients compared with the normal population, and this impairment is sustained even after disease remission is achieved, although function improves considerably with treatment.25
The standard measure of the quality of life in vasculitis is currently the Medical Outcomes Study-Short Form 36 questionnaire.51 It has been used both in the EUVAS trials and the Wegener’s Granulomatosis Etanercept Trial.22,25,52 However, because of its generic nature, it might fail to capture items more specific for patients with systemic vasculitis.53
After a disease duration of 4–5 years, about a third of previously employed patients with systemic vasculitis in the US but only 5% of Dutch patients receive a permanent disability allowance, and a much higher proportion report difficulties with normal daily activities, which can lead to financial loss and strain on relationships. Patients with systemic vasculitis require regular medical monitoring because of frequent relapses and need to continue with potentially toxic treatment often for many years. This leads to high utilisation of medical services.49,54,55
Currently, few data are available on the overall socioeconomic effect of the newer medical treatments for vasculitis. Although most of the newer treatments are much more expensive than the current standard treatments, there is the potential of substantial savings if they prove to be more effective and safer in the long-term control of systemic vasculitis.
SUMMARY AND CONCLUSIONS
In vasculitis, there is a need for standardised clinical tools to assess disease activity, damage and function. No universally applicable serological markers are available to assess disease activity or outcome. Clinical tools have been developed to assist in the evaluation of individual patients and help to justify treatment decisions. They can also provide prognostic information. The development of assessment tools in vasculitis has been vital to the success of large international randomised trials which now provide an evidence base for the management of these diseases. The past 15 years have seen the development and wide application of the BVAS and the VDI, which have become the standard measures for disease activity and damage in vasculitis and can be recommended for universal use. The application of these tools requires training, experience and continuous development.
REFERENCES
Footnotes
-
Published Online First 25 May 2006
-
Competing interests: None