Article Text

Abstract
Objective: To examine the impact of added abatacept treatment on health related quality of life (HRQoL) in patients with rheumatoid arthritis (RA) who have inadequate response to methotrexate (MTX).
Methods: The impact of abatacept treatment on HRQoL was examined in a longitudinal, randomised double blind, placebo controlled clinical trial. Effects of treatment on HRQoL were examined using repeated measures analysis of covariance and comparing rates of change in HRQoL across treatment groups. The relationship between American College of Rheumatology (ACR) clinical markers and disease duration with changes in HRQoL indicators was also examined. Finally, a responder analysis was used to examine the percentage of patients who improved by 0.5 SD in 12 months or who reached the normative levels seen in the US general population.
Results: Statistically significant improvements in the abatacept group relative to controls were observed across a range of HRQoL measures, including physical function, fatigue, all eight domains of the SF-36, and the physical and mental component summaries (PCS and MCS). Improvements were seen as early as day 29 for fatigue and for five out of eight SF-36 domains. By day 169, all HRQoL measures were significantly better with abatacept than with placebo. HRQoL gains were associated with greater ACR clinical improvement, and the effects were consistent for patients with different disease duration. A significantly greater percentage of patients treated with abatacept reached normative levels of PCS, MCS, physical functioning, and fatigue compared with patients treated with MTX alone.
Conclusion: Combined abatacept and MTX treatment produces significant improvements across a wide range of HRQoL domains in patients with RA.
- ACR, American College of Rheumatology
- ANCOVA, analysis of covariance
- ANOVA, analysis of variance
- DMARDs, disease modifying antirheumatic drugs
- HAQ, Health Assessment Questionnaire
- HAQ-DI, HAQ Disability Index
- HRQoL, health related quality of life
- ITT, intention to treat
- LOCF, last observation carried forward
- MCS, mental component summary
- MTX, methotrexate
- OMERACT, Outcomes Measures in Rheumatology Clinical Trials
- PCS, physical component summary
- RA, rheumatoid arthritis
- SF-36, Short Form-36
- VAS, visual analogue scale
- rheumatoid arthritis
- abatacept
- methotrexate
- quality of life
- patient-reported outcomes
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- ANCOVA, analysis of covariance
- ANOVA, analysis of variance
- DMARDs, disease modifying antirheumatic drugs
- HAQ, Health Assessment Questionnaire
- HAQ-DI, HAQ Disability Index
- HRQoL, health related quality of life
- ITT, intention to treat
- LOCF, last observation carried forward
- MCS, mental component summary
- MTX, methotrexate
- OMERACT, Outcomes Measures in Rheumatology Clinical Trials
- PCS, physical component summary
- RA, rheumatoid arthritis
- SF-36, Short Form-36
- VAS, visual analogue scale
Rheumatoid arthritis (RA) is a chronic, systemic disease with a worldwide prevalence of about 1% and an annual incidence of approximately 3 in 10 000 adults.1 Joint damage frequently begins within the first year after disease onset2 and an estimated 70% of patients show radiographic disease progression after 2 years.3 Patients with active RA have been shown to have deficits in health related quality of life (HRQoL) for a number of physical functioning and mental health dimensions.4–,8 Fatigue is a particularly common symptom in RA and has been identified by the Outcomes Measures in Rheumatology Clinical Trials (OMERACT) consensus effort as one of the most important problems for patients.9 Inadequate relief of fatigue was also rated among the top three concerns by patients with RA in a recent survey conducted by the Arthritis Foundation.10 The burden of RA on patients’ quality of life can often be decreased through effective pharmacological treatment.11–,15
The use of some disease modifying antirheumatic drugs (DMARDs) has been shown to slow the progression of joint destruction and improve the signs and symptoms of RA in many patients.16–,23 However, some patients with RA fail to show an adequate therapeutic response to methotrexate (MTX), while others may need to stop treatment owing to serious adverse reactions.24–,28 Indeed, more than two thirds of patients with RA receiving DMARDs still experience significant fatigue despite treatment.9 Combining MTX with other DMARDs has been shown to improve outcomes.29–,31
Recently, pharmacological treatment has focused on the use of biological agents, such as anti-cytokines, which have been shown both alone and in combination with MTX to improve physical functioning in patients with RA.11,32–,35 Abatacept (CTLA4Ig), a first-in-class selective T cell costimulation modulator,36,37 has recently been shown in phase IIb and III clinical trials to improve the signs and symptoms of RA significantly.38,39
The present clinical trial (AIM—Abatacept in Inadequate responders to Methotrexate) examines the impact of abatacept treatment on HRQoL in patients with RA with an inadequate response to MTX.39 HRQoL was assessed across a wide range of commonly measured domains from physical functioning to general mental health and emotional wellbeing.
METHODS
Study population and design
A total of 652 patients with RA and inadequate response to MTX participated in this 12 month, double blind, randomised, placebo controlled trial comparing the safety and efficacy of combined abatacept and MTX (“abatacept” group; n = 433) treatment versus MTX and placebo (“placebo” group; n = 219).39 Abatacept was given by intravenous infusion in a fixed dose of 10 mg/kg at days 1, 15, 29, and every 28 days thereafter for up to 1 year. All patients received MTX (⩾15 mg/week) for the duration of the study. Before day 169, no adjustments in MTX dose were allowed other than for toxicity.
To participate, patients satisfied the following inclusion criteria: (a) diagnosis of RA according to the American Rheumatism Association40 and classification within functional status I, II, or III according to the revised criteria of the American College of Rheumatology (ACR)41; (b) RA disease duration of >1 year from initial diagnosis; (c) treatment with MTX for at least 3 months, and at a stable dose for 28 days before treatment; (d) washout of all DMARDs other than MTX at least 28 days before treatment; and (e) active disease, characterised by ⩾10 swollen joints, ⩾12 tender joints, and C reactive protein ⩾10 mg/l. Patients were permitted to continue taking oral corticosteroids, provided that the prescribed dose was reduced to the equivalent of ⩽10 mg prednisone daily for 28 days and remained stable for at least 25 out of 28 days before treatment.
This study complied with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Boards.
Health outcomes measures
SF-36 health survey
The Short Form (SF)-36 Health Survey, a well validated measure of general health was used to assess HRQoL,42–,44 The SF-36 consists of eight scales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health, which are aggregated to produce physical and mental component summary measures (PCS and MCS). All SF-36 scales and summary measures were scored using norm based methods that standardise scores to a mean of 50 and a standard deviation (SD) of 10 in the general US population; higher scores indicate better health.44,45 The SF-36 was self administered at baseline and 1, 3, 6, and 12 months after treatment.
Health Assessment Questionnaire (HAQ)
The Health Assessment Questionnaire (HAQ),46–,48 a reliable RA validated tool,47 was used to assess physical functioning. Patients completed the HAQ Disability Index, which consists of 20 items scored to produce eight scales: dressing and grooming, arising, eating, walking, hygiene, reach, grip, and activities. The HAQ was self administered at baseline and at multiple follow-up times during treatment (days 15, 29 and every 28 days thereafter).
VAS fatigue scale
Fatigue was assessed on a 10 cm visual analogue scale (VAS).49 Participants were asked to indicate the degree of fatigue they had experienced because of RA over the past week by placing a mark on a horizontal line anchored by “no fatigue” (0 cm) to “extreme fatigue” (10 cm). The VAS fatigue scale has been shown to correlate reasonably well with clinical measures of fatigue.49
Statistical analysis
All statistical results reported in this study were based on an intention to treat (ITT) analysis using the last observation carried forward (LOCF).
Impact of treatment on HRQoL
The impact of treatment on HRQoL was first examined using a one way repeated measures analysis of covariance (ANCOVA) with contrasts to test for differences in mean SF-36 scores between the two treatment groups at each visit. Each SF-36 domain scale and summary score was evaluated in separate ANCOVA models with baseline values used as the covariate. All ANCOVA results are reported with estimates of effect size (partial η2). Partial η2 is interpreted as the proportion of total variability accounted for by the associated effect relative to overall variability (effect + error). Estimated effect sizes between treatment arms at the end point (fig 1⇓) were calculated using Cohen’s D = (mean of abatacept group – mean of placebo group)/pooled variance. Confidence intervals for Cohen’s D were calculated using non-central t-distribution estimates.

Mean SF-36 domain scores at the end point (12 months) for each treatment group (*p<0.01; **p<0.001). Treatment groups are “Abatacept” = abatacept + MTX and “Placebo” = placebo + MTX. PF = physical functioning; RP = role physical; BP = bodily pain; GH = general health; VT = vitality; SF = social functioning; RE = role emotional; MH = mental health. Error bars reflect standard deviation. Estimated effect sizes between treatment arms at the end point were calculated using Cohen’s D = (mean of abatacept group – mean of placebo group)/pooled variance. Confidence intervals for Cohen’s D were calculated using non-central t-distribution estimates.
Responder analysis
A responder analysis approach was used (based on the ITT-LOCF data) to determine the percentage of patients from each treatment arm with HRQoL improvements that reached normative benchmark levels commonly seen in the US general population. US general population norms for the SF-36 were estimated from responses to the 1998 National Survey of Functional Health Status.44 Age and sex adjusted means and 95% confidence intervals were used to define a range of PCS and MCS scores that were within normative benchmark levels of the US general population. Because US general population data are not yet available from healthy adults for the HAQ and fatigue VAS measures, a second responder analysis was conducted to determine the percentage of patients from each treatment arm who showed improved HRQoL scores of at least 0.5 SD by 12 months.50
Relationship between HRQoL measures and clinical markers
The average change (over 12 months) in HRQoL was related to specific clinical markers using the method of “known-groups validity”.51 This method is used to determine how well a measure distinguishes groups that are known to differ for a specified criterion variable. In this study, two separate analyses were performed using this technique. The first analysis evaluated to what extent the HRQoL measures distinguished RA groups that had differing levels of clinical improvement according to ACR criteria. A second analysis examined HRQoL improvements in patients with RA who began the trial with differing periods of disease duration. Disease duration was categorised into the following groups: ⩽2 years, >2 years; and ⩽5 years, >5 years; and ⩽10 years; >10 years. Data were analysed using a two factor analysis of variance (ANOVA) with treatment arm and clinical indicator as the independent variables and HRQoL score as the dependent variable.
RESULTS
Patient characteristics
Table 1⇓ shows the baseline demographics and disease characteristics of patients enrolled in the study. The mean age of patients was 51.5 (18–87) years, 79.2% were female, 87.7% were white, 80% were rheumatoid factor positive, and the mean duration of RA was 8.6 years. Results from χ2 analyses showed no significant differences in distribution of sex, race, and disease duration (table 1⇓).
Patient baseline characteristics: χ2 and ANOVA tests showed no significant differences in primary demographics, HRQoL indicators, or clinical characteristics at baseline as a function of treatment group, indicating that randomization was sufficient
In table 1⇑, we show that at baseline, mean SF-36 scores for most subscales were approximately 1 SD or more below the US population norm of 50. The mean (SD) PCS score of patients receiving abatacept was 30.6 (7.3), which is roughly 2 SD below the US population norm of 50. Their mean MCS score of patients was 41.8 (11.4) which is approximately 1 SD below the US population norm of 50. Patients also had poor physical functioning and moderate to severe fatigue. Thus, at baseline, the patients with RA in our study group were experiencing a high disease burden in both physical and mental health domains in comparison with the general US population.
Effect of treatment on HRQoL
Results from the repeated measures ANCOVA demonstrated significant differences between abatacept and placebo at the end point (12 months) for all eight SF-36 domains (fig 1⇑). Indeed, for five of the eight domains (self reported bodily pain, role physical, general health, vitality, and social functioning), the two groups differed significantly by day 29. The scores for the abatacept group were significantly better than for the placebo group for the physical function domain at day 85, and for the role emotional and mental health domains by day 169 (data on SF-36 scores over time not shown). After 3 months of treatment, the difference between abatacept and placebo widened for all of the SF-36 domains.
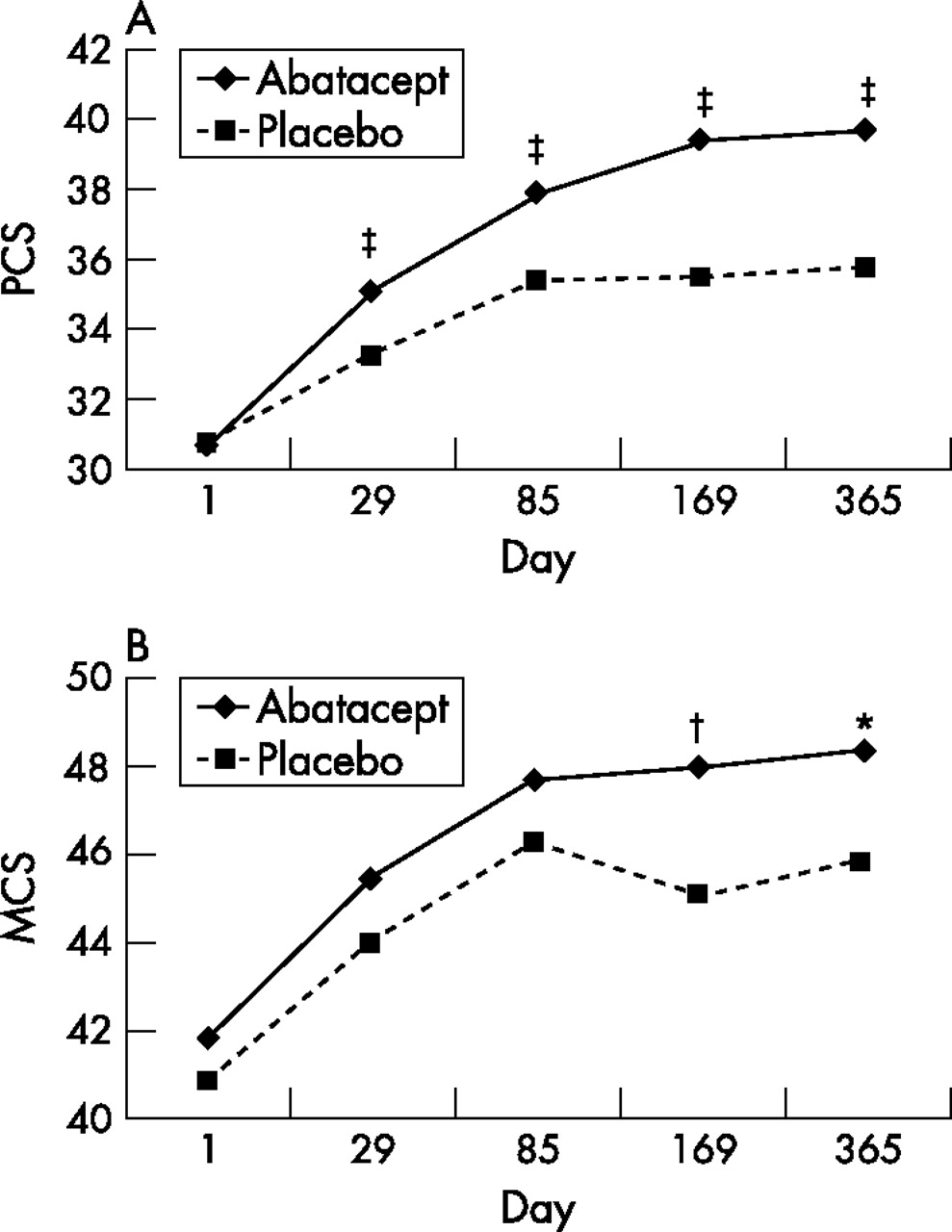
Figure 2⇓ compares the PCS and MCS scores across the two treatment groups. PCS scores improved significantly for the abatacept group relative to patients receiving placebo as early as day 29 (F = 12.18; p<0.001; partial η2 = 0.014) and were maintained thereafter (fig 2A⇓). MCS scores improved significantly for patients receiving abatacept by 6 months relative to the placebo group (F = 7.15; p<0.01; partial η2 = 0.010) and were maintained thereafter (fig 2B⇓). Figures 3A and B⇓ present the results from ANCOVA for fatigue and physical functioning (computed from the HAQ-DI scale), respectively. Fatigue scores declined (indicating improvement) from baseline significantly more in the abatacept group than in the placebo group by day 29 (F = 8.64; p<0.01; partial η2 = 0.008), which was consistent with the observation from the SF-36 vitality domain. Physical functioning scores improved from baseline significantly more in the abatacept group relative to the placebo group by day 57 (F = 5.86; p<0.05; partial η2 = 0.007).

Mean SF-36 (A) Physical (PCS) and (B) mental (MCS) component summary score by treatment group and visit (*p<0.05; †p<0.01; ‡p<0.001). Treatment groups are “Abatacept” = abatacept + MTX and “Placebo” = placebo + MTX.

{kind=link}
{kind=link}
{kind=link}
Mean (A) Fatigue VAS score and (B) HAQ-DI score by treatment group and visit (*p<0.05; †p<0.01; ‡p<0.001). Treatment groups are “Abatacept” = abatacept + MTX and “Placebo” = placebo + MTX.
Responder analysis
Responder analysis demonstrated that a significantly greater percentage of patients from the abatacept group exhibited HRQoL improvements to normative benchmark levels commonly observed in the US general population than in the placebo group. χ2 Analyses showed significant treatment group differences for PCS (χ2 = 7.5; p<0.01) by day 29 that persisted for the duration of the study. By 6 months, 47.1% of the abatacept group had achieved normal PCS score levels relative to the US general population, while 30.7% of the placebo group reached this threshold. Based on this approximately 16% differential effect, the number needed to treat to bring another patient within normative PCS levels is six.
Significant, but smaller differences between the treatment groups were observed for MCS scores by 6 months (χ2 = 5.9; p<0.01), with 60.4% of the abatacept group achieving normative levels relative to the US general population and 50.5% of the placebo group reaching the same threshold. Based on this approximately 10% differential effect, the number needed to treat to bring another patient within normative levels for MCS is 10.
Because US general population norms based on healthy adults were not available for the HAQ and fatigue VAS scales, an additional responder analysis was conducted to determine the percentage of patients who exhibited improved HRQoL scores by at least 0.5 SD over the 12 month period of the study. For each HRQoL measure, a greater proportion of patients receiving abatacept treatment reached the 0.5 SD threshold of improvement than those receiving placebo. χ2 Analyses disclosed significant treatment group differences for PCS (67.2% v 51.1%; χ2 = 12.9; p<0.001), HAQ (72.4% v 55.2%; χ2 = 13.6; p<0.001), and fatigue (64.9% v 47.4%; χ2 = 16.2; p<0.001) scores.
Clinical indicators and change in HRQoL scores
In table 2⇓ we show the mean 12 month change scores in HRQoL measures by different levels of improvement in ACR clinical criteria. A series of two factor ANOVAs indicated that mean change scores of all HRQoL indicators varied systematically with the degree of clinical improvement in ACR criteria. In general, greater HRQoL gains were associated with greater ACR clinical improvement. The strongest association between changes in an HRQoL indicator and changes in ACR clinical criteria was observed for physical functioning (HAQ), followed by PCS, and bodily pain scores.
Mean change scores in HRQoL domains over 12 months as a function of different levels of change in clinical markers based on the ACR criteria
Analysis of mean 12 month change scores in HRQoL measures as a function of disease duration and treatment group (two factor ANOVAs) resulted in no significant main effects for disease duration and no significant interactions (table 3⇓). The only consistent pattern seen in these data was a main effect for treatment group across most HRQoL indicators. Thus, patients receiving abatacept generally had larger HRQoL improvements than patients receiving placebo regardless of disease duration.
Mean change in HRQoL domains over 12 months related to baseline disease duration
DISCUSSION
The AIM study demonstrated that abatacept with background MTX is effective at reducing the symptoms of RA and slowing the progression of structural damage in patients with moderate to severe disease.39 Our study expands these findings by demonstrating the impact of combined abatacept and MTX treatment on a wide range of HRQoL domains, including physical and mental wellbeing, physical functioning, and fatigue. Results from the statistical analyses showed that combined abatacept and MTX treatment produced significantly greater improvement across all HRQoL domains than MTX treatment alone. In particular, significantly greater improvement was seen in patients receiving combined abatacept and MTX than in those receiving MTX alone in role physical, bodily pain, general health, vitality, social functioning, and fatigue scores by day 29. The fast relief of fatigue is particularly noteworthy because it has been identified as one of the most important patient centred issues by the OMERACT consensus group9 and the Arthritis Foundation.10
Physical functioning (measured by the HAQ-DI), improved significantly more in the abatacept group than in the placebo group by day 57. In the AIM study,39 patients in the combined therapy group exhibited significantly greater improvement in several ACR components and ACR20 response within 15 days of treatment compared with those receiving only MTX. Taken together these results demonstrate that abatacept treatment with background MTX produces significantly greater improvements in both clinical markers and HRQoL indicators than MTX alone in a relatively short period of time.
Of particular interest, significant improvement in the MCS score for combined abatacept and MTX treatment relative to MTX alone was observed by 6 months of treatment, and this effect remained undiminished through 12 months. A similar level of improvement in MCS was seen in a phase II study at both 6 and 12 months in patients with an inadequate response to anti-tumour necrosis factor (TNF) treatment (ATTAIN—Abatacept Trial in Treatment of Anti-TNF INadequate Responders).52 This result is especially noteworthy given that the average normalised MCS score of the entire study group was less than 42 at baseline, an established threshold used to screen for major depressive disorder.44
The marked burden of RA on a person’s quality of life is well documented in many studies using different measurement tools.4–8,53 Indeed, our findings are consistent with those reported elsewhere. The mean PCS score at baseline for all patients in this clinical trial was 30.6, approximately two standard deviations below the mean observed in the US general population. Based on the PCS scores alone, the physical functioning of these patients is comparable to that of patients with congestive heart failure in the general US population.44
In this study we also examined the percentage of patients from each treatment group who exhibited improved PCS and MCS scores to normative benchmark levels that are commonly seen in the US general population (adjusted for age and sex). A significantly greater percentage of patients receiving combined abatacept and MTX treatment improved to normal levels of PCS scores by day 29 and MCS scores by 6 months compared with those receiving MTX alone. After 6 months of treatment with abatacept, nearly half of the patients achieved normal PCS scores, and over 60% had normal MCS scores. Similar results were observed for the HAQ and fatigue VAS scores.
Standard ACR indicators were used to compare how changes in clinical characteristics were related to changes in the various HRQoL domains measured. Overall, results from the analyses indicated that changes in clinical markers were systematically related to changes in HRQoL outcomes independently of the treatment group. This demonstrates the existence of a positive relationship between the level of ACR criteria improvement and the level of improvement in HRQoL scores and provides further evidence that HRQoL measures are useful benchmarks for evaluating the effectiveness of RA treatment.
Finally, we examined how changes in HRQoL domains over 12 months were related to differences in disease duration. HRQoL was improved significantly more with abatacept than with placebo, regardless of disease duration.
In conclusion, combined abatacept and MTX treatment provide significant improvements to patients with RA across a range of HRQoL domains, including both physical and mental health, physical functioning, and fatigue.
Acknowledgments
We thank Mark Kosinski, Nan Luo, and Margaret Codianni for their assistance with this project. We acknowledge Bristol-Myers Squibb’s financial support for this project.
REFERENCES
Footnotes
Published Online First 20 December 2006