Article Text

Abstract
Objective: To characterise the immunohistological features of sacroiliitis in ankylosing spondylitis (AS) at different disease stages.
Methods: Biopsy samples from sacroiliac joints (SIJs) of five patients with AS, two with early, three with advanced changes and samples from age matched controls from one necropsy SIJ and two iliac bone marrow (BM) biopsies were studied. Paraffin sections were immunostained in triplicate for T cells (CD3, CD8), macrophages (CD68), and the cytokines tumour necrosis factor α (TNFα), interferon γ, interleukin (IL) 1β, IL6, IL10, and transforming growth factor β1 (TGFβ1). Stained cells were counted over one entire high power field (×400) per section in BM, cartilage, and other connective tissue (CT). Results are the mean of three sections.
Results: CD3+ T cells were numerous in the BM of early AS, and in the CT of one patient with early and one with late AS, with variable proportions of CD8+ T cells. All patients with AS had more CD68+ macrophages than controls in BM and CT; in cartilage, one patient with early and one with late AS had increased CD68+ cells, some being osteoclasts. The patient with very early AS had large numbers of TNFα cells in the three tissular areas; for the other patient with early disease they were found only in CT and cartilage. IL6 was seen in 4/4 patients with AS in most areas. Patients with early disease had more T cells, TNFα, and IL6, and patients with advanced AS more TGFβ1.
Conclusion: The immunohistological findings of a limited sample suggest a role for BM in sacroiliitis, for TNFα and IL6 in early, active lesions, and for TGFβ1 at the time of secondary cartilage and bone proliferation.
- AS, ankylosing spondylitis
- BM, bone marrow
- CT, connective tissue
- IFNγ, interferon γ
- IL, interleukin
- RA, rheumatoid arthritis
- rh, recombinant human
- SIJs, sacroiliac joints
- SpA, spondyloarthritis
- TNFα, tumour necrosis factor α, TGFβ, transforming growth factor β
- ankylosing spondylitis
- sacroiliitis
- immunohistology
- tumour necrosis factor α
- transforming growth factor β
Statistics from Altmetric.com
- AS, ankylosing spondylitis
- BM, bone marrow
- CT, connective tissue
- IFNγ, interferon γ
- IL, interleukin
- RA, rheumatoid arthritis
- rh, recombinant human
- SIJs, sacroiliac joints
- SpA, spondyloarthritis
- TNFα, tumour necrosis factor α, TGFβ, transforming growth factor β
- ankylosing spondylitis
- sacroiliitis
- immunohistology
- tumour necrosis factor α
- transforming growth factor β
Involvement of the sacroiliac joints (SIJs) is a major and characteristic feature of the spondyloarthritides (SpAs). In ankylosing spondylitis (AS)1 and undifferentiated SpA,2 sacroiliitis is the most frequent clinical finding and the presumed first manifestation of the disease. Because it is of major interest to perform histological and immunohistological investigations of sacroiliac inflammation in different stages of SpA we started to biopsy SIJs under computed tomography guidance in combination with intra-articular steroid injections.3 Using this approach, we found that CD4+ and CD8+ T cells and macrophages were major constituents of the detected cellular infiltrates,4 and that cytokine mRNA of tumour necrosis factor α (TNFα) and transforming growth factor β (TGFβ) were present at distinct localities. In another study we confirmed the data of the first study and were also able to correlate the degree of cellularity with quantitative data obtained by magnetic resonance imaging.5 The main problem of the computed tomography guided biopsy technique is that the size of the specimens only allows for limited histological investigation. Another problem is that exact determination of the origin of the specimen is difficult and often not possible.
Because it has always been rather difficult to obtain open sacroiliac biopsy specimens, only a few investigators have managed to examine sacroiliac material of open surgical biopsies or necropsies in AS.6,7,8,9,10,11,12,13,14,15,16 Moreover, only one systematic controlled study of the SIJ in this disease has been published.16 From these studies, we learn that not enthesitis but mild, destructive synovitis and myxoid subchondral bone marrow (BM) are the earliest changes identified in AS. Such lesions destroy the adjacent articular cartilage and bone, a loss followed by varying degrees of fibrous scarring, and formation of woven bone and new cartilage. The original articular cartilages fuse and chondral fusion is the predominant mode of ankylosis. Para-articular bone undergoes sclerosis which fades over the years. Both original and metaplastic cartilages and also woven bone are replaced by mature lamellar bone to induce, eventually, bony ankylosis.16
However, our knowledge about cell surface markers and the expression of cytokines at the protein level, including their localisation in the SIJ, is still limited. To characterise further the immunohistological features of sacroiliitis, we undertook with considerable effort an investigation of open biopsy material from SIJs of five patients with AS described in previous papers.11,12,16
PATIENTS AND METHODS
Patients
Five patients at different stages of AS had an open surgical biopsy of the left SIJ between 1971 and 1975; one to four blocks of about 400 mm2 were excised. One patient had early sacroiliitis, symptoms lasting <1 year; his radiographs disclosed only doubtful changes and the excised specimen of the SIJ disclosed mild synovitis and subchondral bone changes with only minimal cartilage and bone destruction. The second patient stated that his symptoms had started 1 year ago; however, his radiographs showed bilateral sacroiliitis with extensive erosions and sclerosis; the biopsy contained articular cartilage, eroded subchondral bone limited by sclerotic bone. The three other patients with AS were in later stages of disease, with less inflammation and more ankylosis. Controls were age matched. One died in 1973 from neuroblastoma; at necropsy the entire SIJ was removed. Two other patients, without inflammatory rheumatic disease, underwent an iliac BM biopsy, showing only unspecific reactive changes.
Samples
All AS samples contained part of the sacroiliac interosseous ligament. The two patients with early disease and one with more advanced AS had some articular cartilage as well; the other two had metaplastic cartilage; all five had entheseal fibrocartilage; one sample contained the growth plate of a dorsal iliac secondary ossification centre. The control SIJ was removed entirely, transverse slabs were cut and, for technical reasons, subdivided into smaller blocks. The iliac bone biopsy specimens were devoid of fibrous connective tissue (CT); one contained an island of cartilage, but not in all slides. Of course, the sacroiliac articular cartilages were present in the necropsy case. So, BM was present in every section, CT, and cartilage or chondroid tissue in all AS sections. Table 1⇓ summarises the main characteristics of patients and tissue samples.
Main characteristics of patients and tissue samples
Immunohistochemical procedures
The paraffin sections were investigated by immunohistology using antibodies against markers of T cells (CD3, CD8), and macrophages (CD68), and against the cytokines TNFα, interferon γ (IFNγ) interleukin (IL) 1β, IL4, IL6, IL10, and TGFβ1 (table 2⇓).
Antibodies and serum samples used for the immunohistochemical staining
Before staining, the sections were deparaffinised in xylene, rehydrated, and washed with Tris buffer (pH 7.4). To analyse the T cell population and the cytokine expression at the protein level and the cytokine distribution in articular cartilage, the sections were stained with primary antibodies and developed with alkaline phosphatase. As primary antibodies, mouse monoclonal antibodies recognising CD3, CD8, CD68, and TNFα, polyclonal rabbit antisera recognising IFNγ, IL1β, IL4, and IL10, a polyclonal goat antiserum recognising IL6, and a polyclonal chicken antiserum recognising TGFβ1 were used (table 2⇑). Immunostaining was performed using the avidin-biotin complex method. As a first step, endogenous biotin was blocked using an avidin-biotin blocking kit (Vector, Burlingame, CA, USA). To avoid non-specific binding of antibodies, the sections were incubated with phosphate buffered saline containing 3% bovine serum albumin and 5% human serum for 15 minutes. The buffer was blotted and sections were incubated with the primary antibody sera (table 2⇑) in a humidified chamber for 1 hour. After washing twice in Tris buffer (pH 7.4) the slides were incubated with the biotin-streptavidin conjugated secondary antibodies for 1 hour. The slides were washed again, stained with affinity purified streptavidin/alkaline phosphatase (Sigma, St Louis, MO, USA) for 45 minutes and the staining was visualised using fuchsin as an alkaline phosphatase substrate. Counterstaining of the nuclei was performed with Papanicolaou’s haematoxylin (Merck, Darmstadt, Germany) and the slides were mounted in Kaisers’ glycerol gelatin (Merck, Darmstadt, Germany). All steps were performed at room temperature.
To control the immunostaining, the specificities of the primary antibody sera were tested twofold. As isotype controls for the monoclonal antibodies recognising CD3, CD8, CD68, and TNFα, mouse antibodies of the IgG1 and IgG2 isotypes were used. The isotype controls for the polyclonal sera were normal rabbit, normal goat, and normal chicken sera. The specificities were further tested by absorption of the antibody sera with a fivefold mass excess of the corresponding antigen for 1 hour at room temperature, using recombinant human (rh) IL1β, rhIL6, and rhTGFβ1 (Immuno Kontact, Frankfurt, Germany), rhIL1α, rhIL4, rhIL10, rhIFNγ, and rhTNFα (Biozol, Eiching, Germany). Subsequently, cartilage sections were stained using the supernatant instead of the pure antibody sera. None of the controls resulted in a positive staining. As a control for the blocking experiment, the polyclonal sera recognising IL4, IL10, and IFNγ were additionally preincubated with rhIL6. As expected, the resulting supernatants gave rise to stainings identical to unblocked sera. Sections were examined under a light microscope (Olympus BX60).
Reading and grading of immunohistochemical staining
The sections were stained in triplicate. The percentages of positively stained cells were determined by counting the positive cells over the entire area of one high power field (magnification ×400) for each section. The means calculated from the three sections and the corresponding standard errors of the mean (SEM) are shown in table 3⇓. For the localisation of the immunostained cells, three areas/tissues were considered.
Percentages of CD3+, CD8+, and CD68+ cells
The sections studied comprised (a) BM; (b) sacroiliac ligaments, capsules, synovium, and periosteum, together named CT; and (c) any kind of cartilage. Not every section contained all three components. Most of the material had been decalcified, embedded in paraffin, and cut many years ago.
The reader (LN) was not informed about the origin of the material or about the expected results. However, the control material could be potentially identified by its size (the necropsy case) or shape (cylindrical bone biopsies). Early and late AS cases could not be distinguished.
Statistical analysis
Owing to the small sample size, no statistical analysis besides calculating means and SEM was performed. Only striking differences in the quantitative data were taken into consideration. Thus, this is a detailed description of findings in rare valuable material rather than a randomised controlled study.
RESULTS
Histology
In an overview of a control SIJ and of an AS biopsy specimen (fig 1⇓) the ligamentous union can be distinguished from the diarthrodial or synovial joint. A difference in thickness due to focal thickening of the iliac cartilage was seen in the AS (fig 1B⇓) in comparison with the normal sample (fig 1A⇓). The iliac bone appeared denser than the sacral bone. In the AS case, the sacral BM looked normal but the iliac BM had a myxoid appearance. An artificial crack was seen in the subchondral iliac bone, probably due to the fragility caused by the rheumatic inflammation.

Overview of sacroiliac joints. (A) Control joint from an 18 year old woman; (B) sacroiliitis in a 20 year old man, with a disease duration of 1 year: L, ventral part of the ligamentous union; D, diarthrodial or synovial joint; S, sacrum; arrows, cartilage. Haematoxylin and eosin (×4).
Qualitative immunohistology of cells
In the two patients with AS with early changes, there was an accumulation of CD3+ T cells in the BM (fig 2A⇓). Sometimes the infiltrating T cells were aggregated (fig 2B⇓); this was not seen in controls. Many CD3+ T cells were also present in the synovium of the very early case and in the sacroiliac ligament of one late case (not shown). A variable number of these T cells were CD8 positive. A peculiar observation was the clear presence of T cells in a resorption cavity (fig 2C⇓).
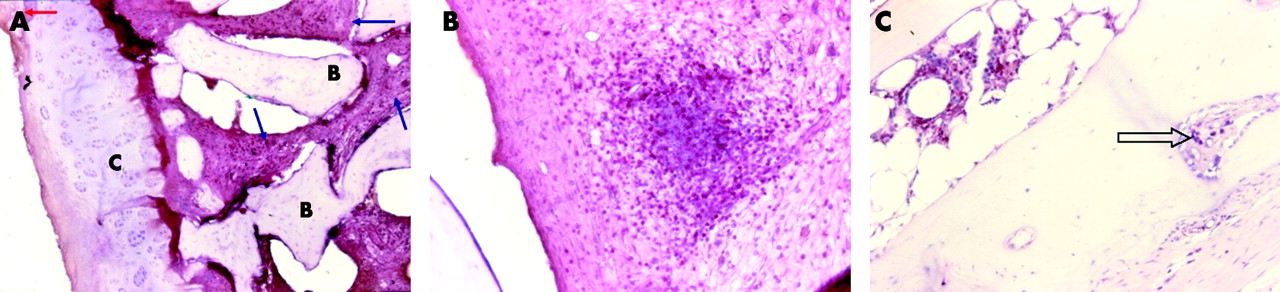
CD3+ T cells. (A) Diffuse infiltrate in the bone marrow of AS patient 2: blue arrows, CD3+ T cells; red arrow, the edge of the pannus creeping over the cartilage; B, bone; C, cartilage (×10). (B) Focal infiltrate in the bone marrow of AS patient 2 (×20). (C) In a resorption cavity of AS patient 4 (×20).
Macrophages were seen in the BM (fig 3A⇓), in the marrow spaces of the sclerotic iliac bone and in the pannus invading superficially the articular cartilage (fig 3B⇓). Osteoclasts, which are also CD68+, were seen in areas of enchondral ossification.
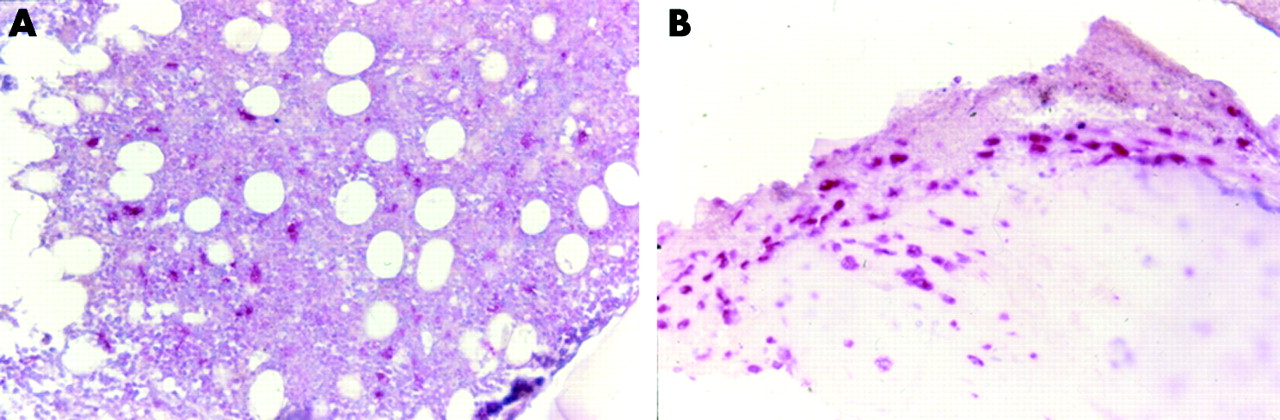
CD 68+ cells. (A) In the iliac bone marrow of AS patient 1 (×20). (B) In the pannus and in the superficial chondrocytes of the articular cartilage in AS patient 2 (×20).
Qualitative immunohistology of cytokines
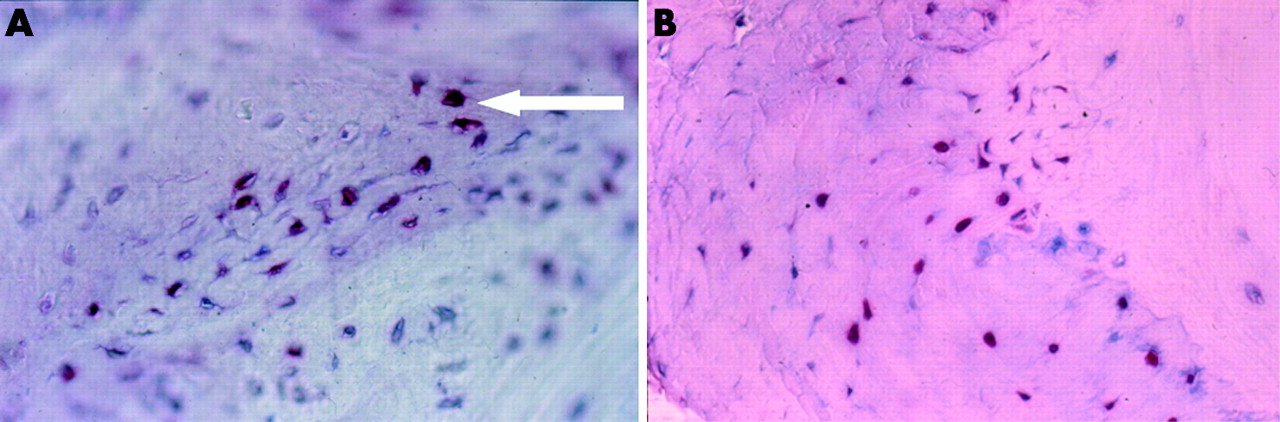
Cytokine containing cells were found in BM, cartilage, and CT of both patients with AS and controls. Figures 4⇓–7⇓ show selected examples of positive staining. TNFα was demonstrated in the BM of AS patient 1 (fig 4A⇓) and in the superficial layer of the articular cartilage in AS patient 2 (fig 4B⇓). IL1β was visible in the BM of AS patient 2 (not shown) and in the interosseous SI ligament of AS patient 4 (not shown). IL6 was recovered in the BM of AS patient 2 (fig 5⇓) and in the repair cartilage of AS patient 4 (not shown). IFNγ was displayed by chondrocytes, BM, and fibrous CT (not shown). TGFβ1 was present in chondroid tissue of patient 3 (fig 6A⇓) and at the bone cartilage of AS patient 4 (fig 6B⇓). IL10 was observed in the resorbing front of a resorption canal in the bone of AS patient 4 (Fig.7). Immunostaining for IL4 was generally unsuccessful.

TNFα. (A) Each intense red dot represents abundant TNFα in the iliac BM of AS patient 1 (×20). (B) TNFα expression in the superficial chondrocytes of articular cartilage of AS patient 2 (×20).

IL6. In the BM of AS patient 2 (×40).

TGFβ1. (A) In chondroid tissue of AS patient 3 (×40). (B) At the interface between cartilage (left) and subchondral bone (right) in an ankylosed area of AS patient 4 (×40).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
IL10. Resorption canal in the bone of AS patient 4, lined by a row of active osteoblasts (thin arrows); the osteoblasts of the resorbing front contain IL (thick arrow) (×20).
Quantitative findings
Individual findings
As shown in table 3⇑, the BM of patients with AS in early disease stages contained high amounts of CD3+ T cells. In the CT, only AS patients 1 and 4 had significant amounts of T cells. No T cells were seen in the cartilage.
The percentages of CD8+ T cells in the BM were between 0.8% and 10% (table 3⇑). As expected, numbers of CD8+ cells were generally lower than numbers of CD3+ cells.
More CD68+ macrophages were found in all the patients with AS than in controls, both in the BM and in the CT (table 3⇑). In the cartilage, patients with AS 2 and 4 had about 15% CD68+ cells, some appearing as osteoclasts.
Compared with the controls, only the patient with very early AS had increased numbers of TNFα+ cells. This was the case in all three tissular areas (table 4⇓).
Percentages of TNFα+, IL6+, and TGFβ1+ cells
IL1β was present in the BM of control patient 1 and in AS patients 2 and 4; the last of these patient also had high amounts in the CT (not shown). IL6 could technically not be investigated in AS patient 1. IL6 was seen in all other AS cases in all areas, except in the cartilage of AS patient 3 (table 4⇑).
In the BM, the percentage of IFNγ+ cells was not different between patients and controls (not shown). Some IFNγ+ was seen in the CT and the cartilage of patients with AS. IL10 was somewhat more common in the BM of patients with AS (mainly patient 2) than in controls (not shown). Staining for TGFβ1 was unsuccessful in control patient 1. Not enough material was available in AS patient 1 (table 4⇑).
Pooled results
When the results of the patients 1 and 2 with “early” AS were compared with those of the patients 3–5 with “late” AS, some striking differences between early and late cases were seen: early cases showed more T cells, TNFα, and IL6, and late cases more TGFβ1.
DISCUSSION
As far as we know, this is the first study on the relative frequency of immune cells and cytokines in open sacroiliac biopsies of patients with AS at different stages of the disease.
Although our samples were obtained decades ago, most specimens could still be nicely stained. However, we cannot exclude the possibility that the failure to stain for IL4 was due to the age of the material.
In contrast with sacroiliac needle biopsies, the major advantage of this study is the rather exact localisation of cells and cytokines within the SIJ. Because it is very difficult to obtain such material, the number of samples was limited. Therefore no advanced statistical analyses were performed. However, this is unique and rare material, and similar biopsies have not been performed for decades.
A remarkable observation in this study is the relatively large number of CD3+ T cells and CD68+ cells (mainly macrophages and osteoclasts) in the BM of patients with AS. While T cells were mainly seen in early cases, macrophages were seen similarly often in both disease stages. This finding, confirming previous data obtained by needle biopsy in active sacroiliitis in patients with AS4 and SpA5, is consistent with a pathogenetic role for such cells in the BM in early AS.
Involvement of the BM in AS has already been suspected in earlier studies.6,10–,16 Increased numbers of T cells, predominantly CD8+ cells, have been described in the BM adjacent to entheses at specimens obtained from hip and knees during endoprosthetic surgery.17 In contrast, a paucity of lymphocytes was seen in needle biopsies of calcaneal insertions18 where macrophages were the predominant cells in the infiltrate, but the bone component was limited in that study. In our study T cells were observed in the synovium of the patient with very early AS and in an inflammatory infiltrate in the sacroiliac ligament in a patient with advanced AS. In contrast, no T cells were seen in the cartilage. There were aggregates of CD8+ T cells. No CD4+ staining was possible for technical reasons. In an earlier study on sacroiliac needle biopsies more CD4+ than CD8+ T cells had been found.4 In synovial knee biopsies of patients with AS about equal amounts of CD4+ and CD8+ T cells have been described.19
In the present study, macrophages and chondroclasts or osteoclasts were present in the eroded articular cartilage of patient 2 with early disease and in the chondro-osseous ankylotic area of patient 4. Recent work has emphasised the role of macrophages in SpA by showing an increased expression of the scavenger receptor CD163 in the synovium as well as in the colonic lamina propria in specimens of patients with AS.20
Our earlier study4 had already reported a large amount of TNFα messenger RNA close to cellular infiltrates in inflamed SIJs. In the present study, this finding is clearly confirmed at the protein level with better localisation. Large numbers of cells containing TNFα, clearly more than in the control cases, were seen in all three tissues of patient 1 with early AS, and also in the CT and the cartilage of the other patient with early disease (No 2). This does not exclude the possibility that the other patients also had an increase in TNFα secretion in another area that was not detected. The cellular source of this proinflammatory cytokine is not clear. It is known that mainly macrophages but also lymphocytes can produce TNFα. This observation lends further pathophysiological support to the treatment of AS with anti-TNFα agents. At least it might partly explain the impressive efficacy of anti-TNFα therapy in active AS which has been demonstrated both clinically 21–,23 and by magnetic resonance imaging (MRI) studies.24
In follow up immunohistological studies after anti-TNFα therapy a reduction of histopathological changes in the synovium of peripheral joints has been seen25,26: decreasing lining layer thickness, less vascularity, lower numbers of macrophages, and down regulated matrix metalloproteinases. Anti-TNF agents may influence a compromised Th1 cytokine pattern, including low TNFα secretion of patients with AS.27–,31 The data on serum levels of TNFα in AS are similarly conflicting.32,33 Taken together, there is a clear role for TNFα in the pathogenesis of AS. Studies on this subject should include the BM as a possible early source and the potential origin of this important cytokine.
The present study demonstrates IL6 in all tissues of 4/5 patients with AS, not enough material being available to test the remaining case. The highest levels were found in the very active inflammatory and destructive changes of AS patient 2. Raised levels of IL6 have been recovered in the synovial fluid of patients with different forms of arthritis, including some cases of AS.34,35 In accordance, we found more IL6 in the CT and in the cartilage but not in the BM, in the one early case as compared with the three late cases. Increased serum levels of IL6 have been detected in patients with AS by several32,36,37 but not all investigators.33 A positive correlation between IL6 and erythrocyte sedimentation rate was described in patients with SpA.38 Taken together, there is some evidence for a role of IL6 in the pathogenesis of AS.
In the BM of AS patients 2 and 4 we did also find IL1β. Peripheral blood mononuclear cells of patients with AS were shown to produce IL1β to a greater extent than controls,39 whereas serum levels of IL1β were reportedly normal.32,33,40 Nevertheless, on the basis of recent genetic findings which point to an increased prevalence of an IL1 polymorphism in AS, a role for IL1β seems probable.41–,43
IL10 was recovered in the BM of all our patients with AS in higher amounts than in the controls, with a maximum in AS patient 2 with early disease. IL10 plasma levels have been shown to correlate with disease activity in patients with SpA.44 This has also been interpreted as an indication of a Th2 pattern of cytokine response. However, there has been quite an argument about this, and it is not clear which type of immune response predominates at which stage of disease.
TGFβ1 was recovered in high amounts in the connective tissues and cartilage of the three patients with more advance AS (Nos 3–5), in sharp contrast with AS patient 2 with early disease. This is not surprising in the repair phase after destruction, because repair is characterised by cartilage and bone proliferation, and because TGFβ1 is known to be one of the most important anabolic factors in articular cartilage and bone.45,46 In the newborn rat femur, TGFβ injected subperiosteally induced localised intramembranous bone formation and chondrogenesis; the dose of TGFβ determined what type of tissue would predominate, a high dose giving rise to more cartilage than bone.46 TGFβ is autoregulatory for itself and T cells, limiting their clonal expansion,47 and more so for CD4+ than for CD8+ T cells.48 Serum levels of TGFβ1 were found to be increased in oriental but not in European patients with AS, independently of TGFβ1 genotypes.49,50 Patients with AS produced more TGFβ1 upon non-specific stimulation than controls,49 while synovial levels of TGFβ1 were found to be increased in patients with SpA and rheumatoid arthritis (RA) compared with osteoarthritis.51 However, genetic studies have not found a strong role for TGFβ1 gene polymorphisms in AS.52
Chondro-osseous ankylosis is one of the characteristic changes of AS16—one of the possible features distinguishing AS from RA. Such a difference could be the consequence of TGFβ in the tissue, which may favour chondrogenesis over direct ossification.46 Whether synovial tissue levels of TGFβ are higher in AS than in RA is not known. Plasma,53 synovial fluid,52 synovial tissue54,55 levels of TGFβ are raised in RA, and TGFβ mRNA is expressed in rheumatoid synovial fluid cells.56 A higher secretion of TGFβ by T cells, plasma cells, and macrophages was seen in patients with reactive arthritis than in patients with RA.57 The particular tendency towards chondrogenesis in AS has been explained by a high response to TGFβ1 in mice with progressive ankylosis.58 On the whole, the task of studying mediators of new bone formation in AS continues and there is some evidence that TGFβ1 may have a role in that very characteristic feature of this disease.
In summary, the present work confirms the important role played by the BM in AS. It shows a different tissular pattern of cytokines in patients with early disease and in more advanced cases, with more TNFα and IL6 in early cases, and more TGFβ1 in late cases.
Acknowledgments
We thank Dr F Cornillie for valuable assistance with handling of the images.
REFERENCES
Footnotes
Published Online First 25 October 2005