Article Text

Abstract
Objective To investigate the long-term clinical and radiographic disease course of hand osteoarthritis (OA) and determinants of outcome.
Methods Clinical and radiographic measures were obtained at baseline and after 6 years in 289 patients with hand OA (mean age 59.5 years, 83.0% women). Clinical outcomes were self-reported pain and functional limitations assessed with the Australian/Canadian Osteoarthritis Hand Index (AUSCAN). Poor clinical outcome was defined as a follow-up score not fulfilling the Patient Acceptable Symptom State. Radiographic outcome was assessed by osteophytes and joint space narrowing (JSN) on standardised hand radiographs using the Osteoarthritis Research Society International (OARSI) atlas. Radiographic progression was defined as a change in osteophytes or JSN, above the smallest detectable change. Change in outcome measures was calculated and baseline determinants for poor clinical outcome and radiographic progression were assessed using logistic regression analysis.
Results Clinical change showed great variation, with half of the population reporting deterioration. Poor outcome in pain was related to high levels of functional limitations and a high number of painful joints at baseline. Poor outcome on functional limitations was related to high baseline pain levels. Radiographic progression was present in 52.5% of patients and associated with high baseline levels of pain, nodes, osteophytes and the presence of erosive OA and nodal OA. Clinical change and radiographic progression were not related.
Conclusions This study gives insight in the clinical and radiographic course of hand OA as well as determinants of outcome. These findings enable better patient information on prognosis. The relationship between clinical and radiographic outcome needs further investigation.
Statistics from Altmetric.com
Introduction
Osteoarthritis (OA) is a common musculoskeletal disorder characterised by degradation of cartilage and changes in subchondral bone leading to pain and disability. The hand is a frequently involved joint site.1 2 The prevalence of symptomatic hand OA is estimated to be as high as 26% in women over 70 years of age.3 It is therefore a burden for the individual and for society, increasing in relevance with an ageing population.3 4 Treatment options are limited to patient education and symptom alleviation.
Despite its high prevalence and disease burden, little is known about the natural history of hand OA and the determinants of outcome. Knowledge of these topics enables the clinician to provide the patient with a more accurate prognosis and information about the disease. From a scientific point of view insight in the disease course and risk factors for an unfavourable outcome may reveal modifiable factors and thus enable the development of new therapies, including much desired structure modifying treatments.
Studies investigating the course of hand OA in patient populations are scarce.5,–,8 Previously, we reported on the course of hand OA over a period of 2 years, showing that a considerable proportion of patients showed clinical as well as radiographic deterioration over this relatively short period.8 Since hand OA is a chronic disease and data on its long-term course and outcome are lacking, we assessed the clinical and radiographic disease course of hand OA over a period of 6 years as well as determinants of poor clinical outcome and radiographic progression in a cohort of patients with hand OA. In addition, we assessed if changes in clinical symptoms are related to radiographic progression.
Patients and methods
Study design and patient population
The ‘Genetics ARthrosis and Progression’ (GARP) study is a cohort study aimed at identifying determinants of OA susceptibility and progression. The study population comprises 192 Caucasian sibling pairs with symptomatic OA at multiple sites in the hand or in at least 2 of the following sites: hand, knee, hip or spine. Patients were recruited from rheumatologists, orthopaedic surgeons and general practitioners. Further details about the recruitment and selection have been published elsewhere.9 The GARP study was approved by the relevant Medical Ethics Committee.
Patients were included for baseline assessment between August 2000 and March 2003. From April 2007 to June 2008 participants who consented for a follow-up evaluation were assessed. All consenters completed questionnaires and part of them visited the outpatient clinic for physical examination and radiographic evaluation.
Patients were eligible for the present study if they had hand OA defined according to the American College of Rheumatology criteria for clinical hand OA10 or if structural abnormalities were present. Structural abnormalities were defined as the presence of radiographic hand OA based on a Kellgren–Lawrence score of ≥2 in at least one interphalangeal (IP) or first carpometacarpal (CMC-1) joint, or the presence of at least two Heberden or Bouchard nodes.
Clinical outcome
Self-reported hand pain and functional limitations were assessed with the pain (five items) and physical functioning (nine items) subscales of the Australian/Canadian Osteoarthritis Hand Index, Likert form 3.0 (AUSCAN LK 3.0).11 On this hand-specific questionnaire items are rated from 0 (none) to 4 (extreme) using a 48-h timeframe. Higher scores indicate worse pain and more functional limitations.
Radiographic outcome
Hand radiographs (dorsal–volar) were obtained at baseline and follow-up by a single radiographer, employing a standard protocol with a fixed film focus distance (1.15 m). Radiographs were scored paired in chronological order blinded for patient characteristics by consensus opinion of two experienced readers (JB, IW) using the Osteoarthritis Research Society International (OARSI) atlas.12 Osteophytes and joint space narrowing (JSN) were graded 0–3 in the distal interphalangeal (DIP), proximal interphalangeal (PIP), first interphalangeal (IP-1), CMC-1, metacarpophalangeal (MCP) and scaphotrapezotrapezoidal (STT) joints with total scores ranging from 0 to 96. Intraclass correlation coefficients for intrareader reproducibility based on 25 randomly selected pairs of radiographs were 0.94 for osteophytes and 0.87 for JSN.
Determinants of outcome
All determinants were measured at baseline. Demographic variables were age, sex, body mass index (BMI) and postmenopausal status.
Clinical determinants were pain and functional limitations measured with the AUSCAN, pain intensity score and the number of self-reported painful joints. The pain intensity score was obtained by grading pain on joint pressure from 0 to 3 in 30 hand joints (0=no pain, 1=with pain, 2=with pain and wincing, 3=with pain, wincing and withdrawal of joint). The number of painful joints was obtained using a standard diagram including 30 hand joints on which the patient marked the joints where pain was experienced on most days of the preceding month.
Determinants reflecting structural abnormalities were osteophytes, JSN and the number of nodes in IP joints plus CMC-1 squaring. The latter was assessed by joint palpation.
In addition, three proposed hand OA subsets were evaluated as outcome determinants.13 Erosive OA was defined as the presence of erosive radiographic features according to the Verbruggen–Veys score in at least two IP joints.14 Nodal OA was defined as the presence of Heberden or Bouchard nodes affecting at least two rays of either hand.15 The last subset comprises symptomatic thumb base OA, which was defined as the presence of pain or stiffness in the CMC-1 joint on most of the days of the preceding month.
The use of medication for OA joint symptoms at baseline and follow-up and hand surgery performed over the follow-up period were recorded.
Statistical analysis
Data were analysed using SPSS V.16.0 (SPSS, Chicago, Illinois, USA). Mean changes with 95% CI for AUSCAN pain, AUSCAN functional limitations, osteophyte and JSN scores were calculated. Cumulative probability plots were used to visualise change in these measures. To evaluate the proportion of patients with clinically relevant change in pain and functional limitations, the minimum clinically important improvement (MCII) of 1.49 and 1.25, respectively, was used.16 Those with a change on AUSCAN pain and functional limitations below −1.49 and −1.25, respectively, were classified as improved. Patients with change on AUSCAN pain and functional limitations above 1.49 and 1.25, respectively, were classified as deteriorated. For osteophytes and JSN the smallest detectable change (SDC) was used to assess change above measurement error.17 The SDC was 1.3 for osteophytes and 1.5 for JSN.
Poor clinical outcome was defined as AUSCAN pain and functional limitation scores at follow-up above the Patient Acceptable Symptom State, which were 8.2 and 16.1, respectively.18 Generalised estimating equation (GEE) models were used to estimate the risk for poor clinical outcome after 6 years for tertiles of baseline determinants with robust variance estimators to account for family effects within sibling pairs. Adjustments were made for baseline tertiles of AUSCAN pain and functional limitations depending on the outcome and for follow-up time.
Radiographic progression was defined as a change in osteophytes or JSN above the SDC. The risk for radiographic progression was estimated for tertiles of baseline determinants using GEE analysis to account for family effects within sibling pairs. Corrections were made for tertiles of baseline osteophyte and JSN scores and follow-up time.
ORs were subsequently transformed to risk ratios (RRs) using the approximation formula described by Zhang and Yu because ORs for common outcomes in a fixed cohort are not good approximations of RRs.19
The association between change in symptoms and radiographic progression was assessed by estimating mean differences of change on AUSCAN pain and functional limitations between patients with and without radiographic progression using linear mixed models. Adjustments were made for age, sex, BMI, baseline AUSCAN, baseline osteophytes, baseline JSN, follow-up time and family effects within sibling pairs.
Results
Study population
Of the 357 patients with hand OA at baseline 300 (84.0%) consented to participate in the follow-up study of whom 242 completed questionnaires and visited the outpatient clinic and 58 completed questionnaires only. Consent was not given by 43 (12.0%) patients, 12 (3.3%) were deceased and 2 (0.6%) were lost to follow-up. Most frequent reasons for non-consent were loss of interest (n=13), health problems not related to OA (n=7), unavailability of transport (n=7) and emigration (n=2). Of the 300 eligible patients complete clinical or radiographic follow-up data were available in 289 patients. These patients were included in the present study. Of these 289 patients, 18 had no baseline AUSCAN due to delayed validation of the Dutch AUSCAN. Of the 242 patients visiting the outpatient clinic, 6 had incomplete data due to missing radiographs.
The mean follow-up time was 6.1 years (range 5.0–7.8 years). Baseline characteristics are shown in table 1. Patients not included were somewhat older. Other demographic characteristic as well as disease characteristics did not differ between these groups (data not shown). Looking at hand OA subsets, 22 patients had erosive OA and thumb base OA comprising 52.4% and 16.2% of the patients with erosive OA and thumb base OA, respectively.
Baseline characteristics of 289 patients with hand osteoarthritis (OA)
Clinical course of hand OA over 6 years
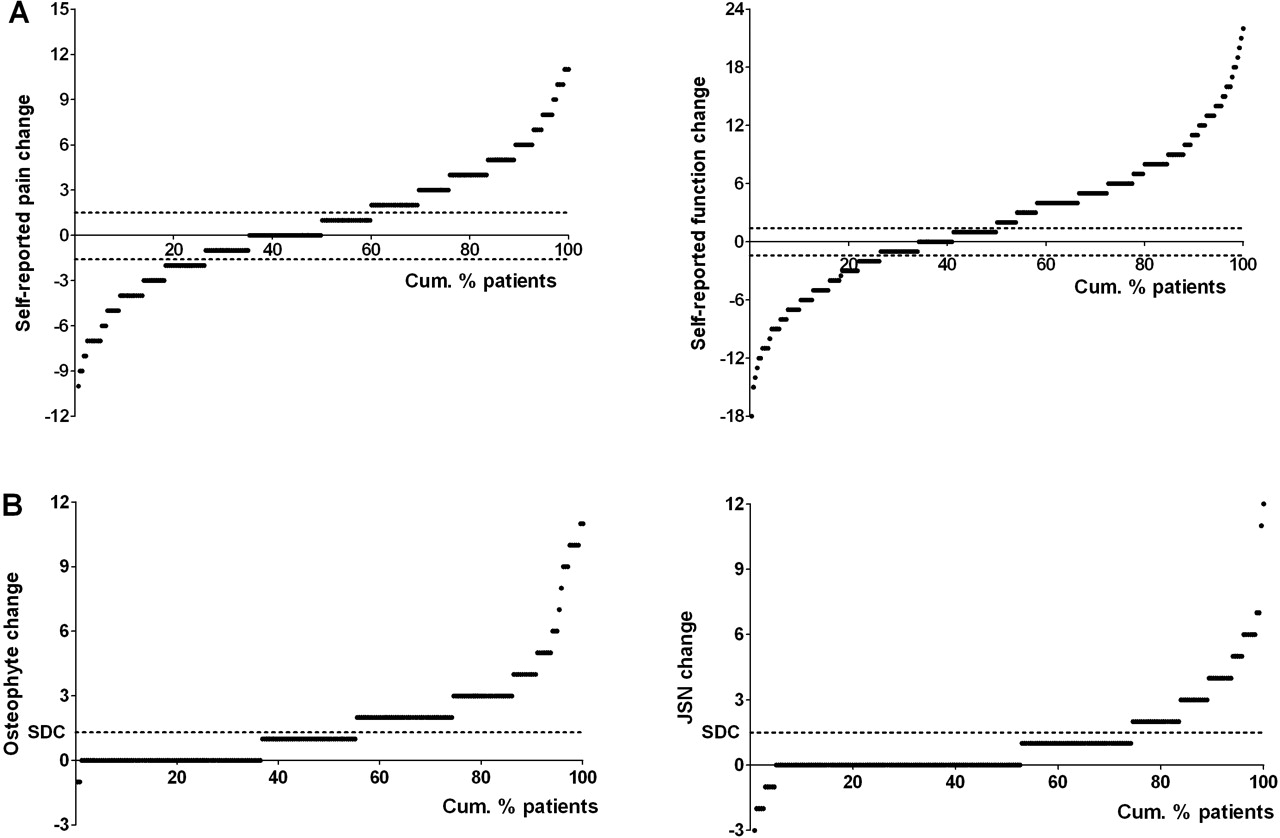
The mean increase in self-reported pain was small (table 2). However, there was great variation on the individual level as shown in figure 1A. An increase in pain was present in 109 patients (40.2%) whereas 71 patients (26.2%) reported less pain. The same was found for change in functional limitations: 136 patients (50.2%) patients reported more functional limitations and 71 patients (26.2%) improved (figure 1A).

{kind=link}
Cumulative probability plots of change in self-reported pain and functional limitations, osteophytes and joint space narrowing (JSN) in patients with hand osteoarthritis over a 6-year period. A. Change in self-reported pain and functional limitations. The dotted lines represent the cut-off for deterioration and improvement based on the minimum clinically important improvement. Patients above the upper dotted line have deterioration of pain or functional limitations. Patients below the lower dotted line have improvement of pain or functional limitations. B. Change in osteophytes and JSN. All patients above the dotted smallest detectable change (SDC) line are classified as having progression in osteophytes or JSN.
Baseline, follow-up and change scores on self-reported pain and functional limitations (n=271), osteophytes and joint space narrowing (n=236) in patients with hand osteoarthritis followed for 6 years.
At baseline and follow-up 137 (47.4%) and 157 (54.3%) patients used medication for joint symptoms, respectively. Non-steroidal anti-inflammatory drugs and paracetamol were most frequently used: at baseline by 67.2% and 52.6%, respectively and at follow-up by 45.2% and 75.2%, respectively. Hand surgery was performed in 46 (15.9%) patients, comprising mostly of surgery for carpal tunnel syndrome and in 4 cases of joint surgery.
Radiographic course of hand OA over 6 years
Osteophyte and JSN scores increased over time (table 2). Progression of osteophytes and JSN was present in 106 (44.9%) and 61 (25.8%) patients, respectively (figure 1B). In 124 (52.5%) patients radiographic progression, defined as progression in osteophytes or JSN, was present. Most change was seen in the DIP joints followed by the PIP joints and CMC-1 joints (table 3).
Distribution of changes in osteophytes and joint space narrowing of the hand over 6 years in 236 patients with hand osteoarthritis
Determinants of poor clinical outcome in hand OA after 6 years
Poor outcome in pain was related to high levels of functional limitations and a high number of painful joints at baseline (table 4). More pain at baseline, reflected by AUSCAN pain and the number of painful joints, was associated with a higher risk of poor outcome in functional limitations. Determinants reflecting structural abnormalities, demographic characteristics (data not shown) and hand OA subsets were not associated with poor clinical outcome. Adjustment for medication use or hand surgery did not substantially influence the estimates.
Risk of poor clinical outcome of hand osteoarthritis on self-reported pain and functional limitations defined as not fulfilling the Patient Acceptable Symptom State after 6 years, for tertiles of baseline determinants and hand osteoarthritis subsets
Determinants of radiographic progression of hand OA over 6 years
Demographic characteristics were not related to radiographic progression (data not shown). Of the clinical variables, high levels of self-reported pain and pain intensity were associated with a higher risk of radiographic progression, whereas self-reported functional limitations were not (table 5). A high number of nodes and osteophyte scores were also related to radiographic progression. Patients with erosive OA had a higher risk of radiographic progression than patients with non-erosive OA. Nodal OA was associated with a two times higher risk of radiographic progression. Correction for medication use or hand surgery did not change these results.
Risk of radiographic progression of hand osteoarthritis over 6 years for tertiles of baseline determinants and hand osteoarthritis subsets
Relationship between clinical change and radiographic progression in hand OA
The mean change in self-reported pain and functional limitations was not different between patients with and without radiographic progression, with adjusted mean differences (95% CI) of −0.14 (−1.21, 0.92) and −0.57 (2.36, 1.22) for pain and functional limitations, respectively. This means that clinical change and radiographic progression are not related.
Discussion
This study is the first to assess the long-term course of symptoms and radiographic abnormalities in patients with hand OA and determinants of poor outcome. In contrast to the ongoing radiographic progression, clinically, deterioration and improvement were observed. Poor clinical outcome after 6 years was associated with high levels of pain and functional limitations at baseline. More pain, structural abnormalities and the presence of erosive OA and nodal OA were associated with a higher risk of radiographic progression over 6 years. Change in symptoms and radiographic progression were not related. These findings give insight in the long-term disease course of hand OA and factors associated with poor outcome. As a consequence the clinician can provide the patient with more accurate information on prognosis. From a scientific point of view these findings imply that the clinical and radiographic course of hand OA are distinct, making development of structure modifying treatments with clinical benefit challenging.
Very few studies report on the clinical course of hand OA. We found that over a period of 6 years 40% to 50% of patients experienced more pain and functional limitations whereas about a quarter improved. These proportions are similar to the proportions reported over a 2-year period in the GARP study.8 Our findings are in line with a study by Dieppe et al who found that around half of the population reported worse overall OA condition over 3 and 8 years, whereas about a quarter improved over both periods.20 Allen et al showed that the average change on AUSCAN scores over 4 years was small, but again almost half of the individuals reported worse hand symptoms.21 It seems that the evolution of clinical symptoms is heterogeneous. Furthermore, the proportion of patients who deteriorate and improve does not differ much in the short and long term. This may be due to adaptation to a chronic condition over time or other psychosocial factors rather than genuine improvement of the disease. The follow-up assessment took place at an arbitrary time point. The change may therefore not reflect the evolution of the disease over the whole time period, although on average it is valid.
The radiographic course of hand OA has been studied more extensively, but still the number of studies is limited. Most studies have been conducted in samples from the general population. In our patient sample we found that 52.5% of patients had radiographic progression: 44.9% had progression of osteophytes and 25.9% had progression of JSN. A study over 10 years found that 90% and 74% of patients with hand OA had progression of osteophytes and JSN, respectively.6 These studies illustrate that the radiographic course of hand OA is an ongoing process.
There are a number of potential limitations to this study. The first concerns the possibility of bias due to differences between consenters and non-consenters. However, demographic and disease characteristics did not differ between these groups, except for a higher age of non-consenters. We expect that this age difference has no effect on the study outcome, since age was not associated with any of the outcomes. Radiographic follow-up data were not available in all patients since a proportion only completed questionnaires. However, baseline radiographic scores did not differ between those with and without complete data indicating that selection bias is probably absent. Third, our sample consists of patients with familial OA at multiple sites. Whether the results can be generalised to patients with other hand OA phenotypes has to be investigated. Another issue concerns the use of the MCII as cut-off for improvement and, conversely, for deterioration on the AUSCAN. This was used because there are no cut-offs available for clinically relevant deterioration on the AUSCAN. Finally, we used a self-reported outcome measure for functioning because performance measures were not available. Since performance is thought to reflect other aspects of functioning it would be interesting to investigate the evolution of hand performance over time as well as determinants of outcome.
To date, the only information the clinician could provide patients with hand OA was that their condition would deteriorate over time. At what pace and what the chances for worsening of the disease are, was unknown. This study enables more accurate information on the disease course and prognosis. We have shown that clinical improvement is seen in a substantial proportion of patients and some of the patients remain stable, even over a long time period. Thus, clinical deterioration is not inevitable for each patient. In contrast, radiographic abnormalities will worsen over time. It is important to bear in mind and inform patients that the evolution of symptoms and radiographic abnormalities are not related. With respect to patient prognosis, this study highlights parameters that are easy to obtain in order to identify patients at risk for poor outcome. If patients report high levels of pain and functional limitations at presentation they are at risk to have poor outcome on pain and functional limitations in the long term. The same is true for patients with more than eight painful joints. Patients with high levels of symptoms at presentation, nodal OA, erosive OA or a considerable amount of osteophytes are most likely to show progression of radiographic signs of OA. Since symptoms are most important to patients and predictive for clinical and radiographic outcome of hand OA, they are of greater value in the evaluation of patients with hand OA than radiographic OA signs.
We found that change in symptoms was not related to structural changes. This discordance, for hand OA and for OA in general, has been known well from cross-sectional studies and to lesser extent from longitudinal studies.8 22 This has important implications for the development of structure modifying treatments. Since symptomatic hand OA is considered the disease of clinical and public health interest, it is desirable if these treatments influence symptoms and not just structural abnormalities.23 These data show that change in symptoms does not coincide with change in structure. Whether the explanation is that there is really no association or that the current outcome measures are not sensitive enough is unknown, warranting more research.
In conclusion, this study gives insight in the long-term clinical and radiographic disease course of hand OA as well as in determinants of poor outcome. This enables more accurate patient information on prognosis. It also shows that the clinical and radiographic course of hand OA is distinct, making development of structure modifying treatments challenging. Further research on prognostic factors in hand OA is needed to confirm and extend our findings as well as research on the relationship between change in symptoms and structural abnormalities.
Acknowledgments
We would like to acknowledge support of the cooperating hospitals and staff (Bronovo Hospital, The Hague: Dr ML Westedt; Jan van Breemen Instituut, Amsterdam: Dr D van Schaardenburg; Leyenburg Hospital, The Hague: Dr HK Ronday and Dr LN Coene; Reinier de Graaf Gasthuis, Delft: Dr AJ Peeters; Rijnland Hospital, Leiderdorp: Dr EJ van Langelaan) and referring rheumatologists, orthopaedic surgeons and general practitioners.
References
Footnotes
-
Funding The GARP study was financially supported by the Dutch Arthritis Association (project number 06-1-304) and Pfizer (Groton, Connecticut, USA). The sponsors did not contribute to study design, data collection, data analysis and writing of the manuscript. Publication was not contingent on the approval of the sponsors.
-
Ethics approval This study was conducted with the approval of the Leiden University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.