Article Text

Abstract
Patients with idiopathic inflammatory myopathies (IIMs) suffer an increased burden of comorbidities, but data on mortality in recently diagnosed IIM are conflicting. Also, little is known when, if ever, in relation to IIM diagnosis, mortality is increased.
Methods A population-based IIM cohort of patients diagnosed between 2002 and 2011 and general population comparators were identified using healthcare registers. They were linked to the cause of death register for follow-up.
Results 224 (31%) of the 716 patients with IIM and 870 (12%) of the 7100 general population died during follow-up. This corresponded to a mortality rate of 60/1000 person-years in IIM and 20/1000 person-years in the general population. The cumulative mortality at 1 year after diagnosis was 9% in IIM and 1% in the general population, and increased in both IIM and the general population with time. The overall hazard ratio (HR) 95%CI of death comparing IIM with the general population was 3.7 (3.2 to 4.4). When we stratified on time since diagnosis, we noted an increase in mortality already within the first year of diagnosis compared with the general population, HR 9.6 (95% CI 6.9 to 13.5). This HR then plateaued around 2 after >10 years with the disease, although the estimates were not statistically significant. Malignancies, diseases of the circulatory and respiratory system were common causes of death.
Conclusion Mortality is increased in patients with contemporary IIM. The increased mortality was noted within a year of diagnosis, which calls for extra vigilance during the first year of IIM diagnosis.
- dermatomyositis
- polymyositis
- epidemiology
Statistics from Altmetric.com
Introduction
The idiopathic inflammatory myopathies (IIMs) are a heterogeneous group of chronic, systemic disorders, defined by weakness of striated muscle.1 Other organs such as lungs, joints, heart and skin are frequently involved, suggesting that these are systemic inflammatory diseases, but the exact aetiology is unknown. On the basis of clinical, histopathological and immunological features, these disorders are often differentiated into three distinct and major subsets: polymyositis (PM), dermatomyositis (DM) and sporadic inclusion body myositis (sIBM).2 3 IIMs are regarded as treatable disorders, but many patients respond poorly to immunosuppressive treatment, and persisting muscle impairment, as well damage of other organs, such as the lung, is a frequent problem. To date, IIM is considered to be associated with increased severe comorbidity, primarily related to muscle weakness and visceral involvement, as well as increased mortality.4 5
However, population-based valid mortality assessments in IIM have been limited due to the rarity of the disease, variation in the use of classification and diagnostic methods, a heterogeneous study population and the subsequent risk of selection bias.6 7 Hospital-based studies from the 1970s have indicated increased mortality,8–12 and later work has further supported this notion.13 Studies presented have shown large variations in mortality estimates; 10-year survival proportions vary between 18% and 90%,3 4 13–24 variations probably due to differences in study design, patient selection, and large proportions of patients lost to follow-up. One of the latest studies, which is the largest population-based IIM mortality study to date, compared death rates in 326 Norwegian patients with IIM diagnosed between 2003 and 2012 in southern parts of Norway, with death rates in the general population. In that study, a standardised mortality ratio of 2.4/2.6/1.7 in PM/DM/sIBM was reported.20 Unfortunately, incidence rates of death and timing of death risk in relation to IIM diagnosis was not assessed. A later study from the USA, following patients diagnosed 2005–2014, reported 1-year, 5-year and 10-year mortality proportions that are considerably lower than earlier studies,23 which could indicate that we today are better at identifying and treating high-risk patients, thus removing some of the excess risk.
In clinical decision making pertaining to surveillance of patients with IIM, it is crucial to know if there is an increased mortality even in patients diagnosed with IIM today, and if so, when in relation to IIM diagnosis, the risk is elevated and which are the major causes of death.
We therefore performed the first nationwide population-based cohort study of mortality in adult IIM compared with a randomly selected general population comparator cohort with focus on absolute and relative risks and how the risks develop in relation to IIM diagnosis.
Methods
Study design
This study is a population-based nationwide cohort study comparing patients with IIM (exposed) to the general population (unexposed) with respect to risk of death.
Setting
In Sweden, adult patients with IIM are treated by rheumatologists, neurologists, dermatologists or by internists. Virtually. all healthcare, including inpatient care, is universally accessed by all residents, and 95% of all rheumatologists and neurologists are hospital based and work in publicly funded healthcare. Using the unique personal identification number issued to all Swedish residents, data from national and virtually complete administrative or clinical registers on demographics, morbidity and mortality can be linked together. These registers also allow for unbiased identification of general population comparators and enable prospective assessments of morbidity and mortality, independently of IIM status.
Study population
The IIM cohort
Using the Swedish National Patient Register, a nationwide register with full coverage of inpatient care since 1987 and for specialised outpatient care since 2001, we identified a cohort of individuals with IIM. To be included in the incident/newly diagnosed IIM cohort, each individual had to be ≥18 years, have a first-ever visit 2002–2011 plus a follow-up visit within 1–12 months listing International Classification of Disease (ICD) 10 codes indicating IIM (please be referred to the appendix for ICD-10 codes used). The validity of the ICD codes used for IIM has been tested in the same underlying study population as included in the current study, and it indicates high validity of the ICD codes used to identify IIM (positive predictive value of >85 and sensitivity of >85% for all ICD codes except those indicating sIBM).25 In addition, there are two previously published papers: one Swedish,26 partly using the same study population as presented here, and one Canadian,27 also using administrative data, where using ICD codes to identify IIM was found to have a sensitivity of 88%, specificity of 96%27 and a positive predictive value of 85%.26 In the present study, only visits at IIM specialist clinics (rheumatology, internal medicine, dermatology and neurology) were included in the identification algorithm (which is presented in Svensson et al 25). Based on this algorithm, that we believe is somewhat stricter than in the examples presented above, we were able to identify DM as a subgroup of IIM, but due to the overlap in ICD codes for PM and sIBM, the rest of the patients with IIM were analysed together (referred to as other inflammatory myopathies). The latest of the two IIM defining visits was used as index date.
The general population
For each patient classified as a patient with IIM, we randomly selected 10 individuals from the Swedish Population Register (which includes all Swedish residents). Matching variables were sex, year of birth, year when the patient with IIM was first found with an ICD code indicating IIM, and county of residence. Each population-based general population comparator was required to be alive at the index date of its corresponding patient with IIM.
Data sources used to detect outcomes during follow-up
We linked the patients with IIM and their general population comparators to the following data sources: i) The Swedish Population Register, which includes information on births, deaths, emigration and immigration for the entire Swedish population.28 Follow-up data from this register were available until 31 December 2013. ii) The cause of death register, which includes information on death date and underlying cause of death.
By linking the patients with IIM and their matched general population comparators to these registers, we identified all deaths including their causes and all emigrations from Sweden during follow-up, enabling us to perform a cohort analysis with high internal and external validity and virtually no loss of follow-up.
Definition of outcome
Primary outcome for this study was overall death. The secondary outcomes were cause-specific deaths: certain infections and parasitic diseases, malignant neoplasms, diseases of the respiratory system and diseases of the circulatory system (for ICD-10 codes used to identify deaths from the above diagnoses, please be referred to online supplementary table 1). To add information on morbidity around the time of death, we have also investigated the main reasons for hospitalisation the month prior to death.
Supplementary file 1
Follow-up
Follow-up started at index date, which was the date of the second visit in the IIM cohort. Follow-up ended at death, first emigration or 31 December 2013, whichever came first. Once an individual is censored, he or she is no longer followed and stops contributing person-time. Two (0.3%) of the patients with IIM and 61 (0.9%) of the general population emigrated during follow-up.
Statistical analyses
Crude rates were calculated by dividing the number of events during follow-up by the corresponding person-time at risk. All rates are presented as number of events per 1000 person-years. The absolute risks were calculated in men and women separately as well as based on subgroups of IIM, age group at diagnosis and, since mortality is increased in individuals with low income and low socioeconomic status,29 educational level (highest achieved educational level <10 years, 10–12 years and >12 years). To compare the mortality in patients with IIM and the general population, Cox proportional hazards models were constructed to estimate HRs. All models were adjusted for age at index date as a continuous variable, birth year, sex and residential area (with Stockholm as the reference category). The HR of death overall and death from diseases of the circulatory and respiratory systems, from malignant neoplasms, and from certain infections and parasitis diseases were estimated. We also made subgroup analysis based on sex, IIM diagnosis (DM and PM/sIBM), age group and educational level. We used Cox proportional hazards models with time since diagnosis as time varying covariates to estimate the HR of death in four different disease duration windows (<1 year, 1–≤5 years, 5–10 years and >10 years) in order to assess when in the disease course patients with IIM are at highest risk of death. All HRs were also adjusted for educational level. Kaplan-Meier survival curves were plotted to assess time to event and the cumulated mortality at 1, 5 and 10 years after start of follow-up. Since there was no major difference in the results from DM and other inflammatory myopathies, results based on IIM overall are presented.
All analyses were performed using The SAS software package, V.9.4 and STATA IC V.11.2.
Results
Baseline characteristics of the study population
In total, 716 individuals were included in the IIM cohort; 55.2% were women, mean (SD) age at start of follow-up was 61.4 (14.5) years (table 1). In the general population, the proportion women and the mean age at start of follow-up was the same as in the IIM cohort. The educational level in the IIM cohort was similar to the educational level in the general population; 26% had an education extending 12 years. Information on treatment during the first year after start of follow-up was available on a subgroup of the study population. It can be found in online supplementary table 2.
Characteristics of patients with idiopathic inflammatory myopathies (IIMs) identified from the National Patient Register 2002–2011 and their general population comparator cohort
Follow-up
The total time of follow-up in the IIM cohort and in the general population was 49 740 person-years (3740 in patients with IIM, 43 963 in the general population). Median (IQR) follow-up in the IIM cohort was 4.6 (5.4) and 6.0 (5.5) years in the general population.
Absolute mortality and the causes of death
Two hundred twenty-four (31%) of the IIM cohort and 870 (12%) in the general population died during follow-up. This corresponded to a crude incidence rate (95% CI) of 59.9 (42.0 to 77.8) deaths/1000 person-years in IIM and 19.8 (16.5 to 23.1) deaths/1000 person-years in the general population. The mortality rate was similar in men and in women in the IIM cohort but, in the general population, the mortality rate was higher in men than in women (figure 1).

Number of events (N), person years at risk (PYR) and incidence rates (IRs) of death in patients with IIM identified in the National Patient Register between 2002 and 2011 and in an individually matched general population comparator. HR and 95% CI with the matching factors (sex, residential area and year of diagnosis) were taken into account and adjusted for age. Overall and stratified by sex, age group, educational level and IIM subgroup.
The mortality rate also increased with age in both IIM and general population and decreased with increasing educational level.
At time of death, patients with IIM were younger than the general population (mean (SD) age 73 (11) in IIM and 79 (10) in the general population, median (IQR) 75 (15) in IIM and 81 (12) in the general population). Of those who died, more were women in IIM than in the general population (56% vs 47%). Main causes of death in patients with IIM were, besides musculoskeletal and connective tissue disease, malignancies, diseases of the circulatory system and diseases of the respiratory system. The general population also mainly died from these three disease groups (table 2). When we looked at the causes for hospitalisations during the month prior to death, we noted that it was more common for patients with IIM than the general population to be hospitalised overall (45% vs 36%). Patients with IIM were more often hospitalised due to diseases of the respiratory system and diseases of the musculoskeletal system and connective tissue. In the general population, the most common reasons for hospitalisation were diseases of the circulatory system and malignancies (table 2). Among those patients with IIM who died from diseases of the respiratory system (n=21), 20 patients had been hospitalised the month prior to death. The most common reasons for hospitalisation was pneumonia and interstitial lung disease (online supplementary table 3). There was also one hospitalisation for pulmonary arterial hypertension the month prior to death in this group. Among those who died from diseases of the circulatory system (n=63), 26 were hospitalised the month prior to death. Among those, the most common cause for hospitalisation was non-ischaemic heart disease (online supplementary table 4). More information on hospitalisations a month prior to death and more details on the causes of death are found in online supplementary tables 3–7.
Causes of death of all who died during follow-up and the main diagnosis for hospitalisation up to 1 month prior to death in patients with idiopathic inflammatory myopathy (IIM) identified from the National Patient Register 2002–2011 as well as the general population cohort
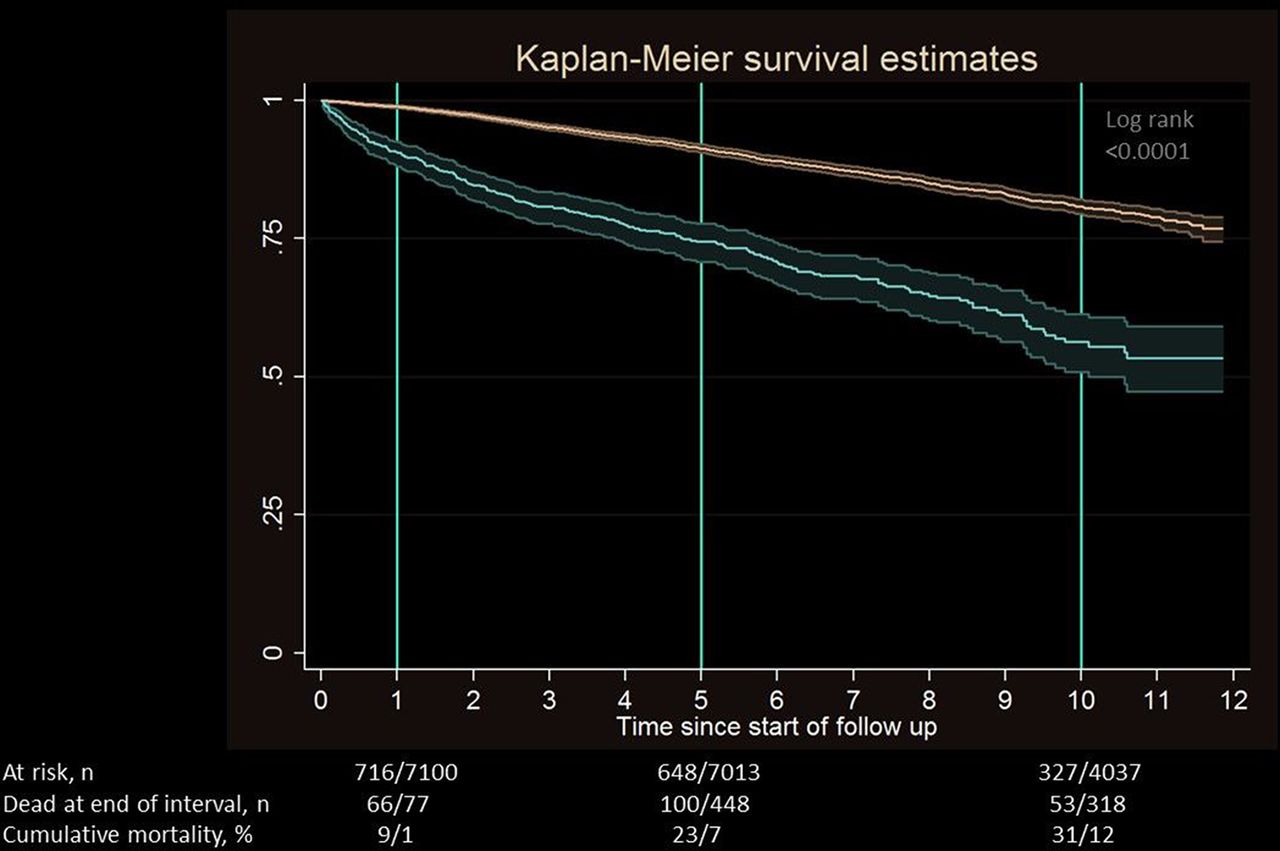
The cumulative mortality at 1 year after diagnosis was 9% in IIM and 1% in the general population, at 5 years it was 23% in IIM and 8% in general population and at 10 years, the proportion was 31% and 12% (figure 2).
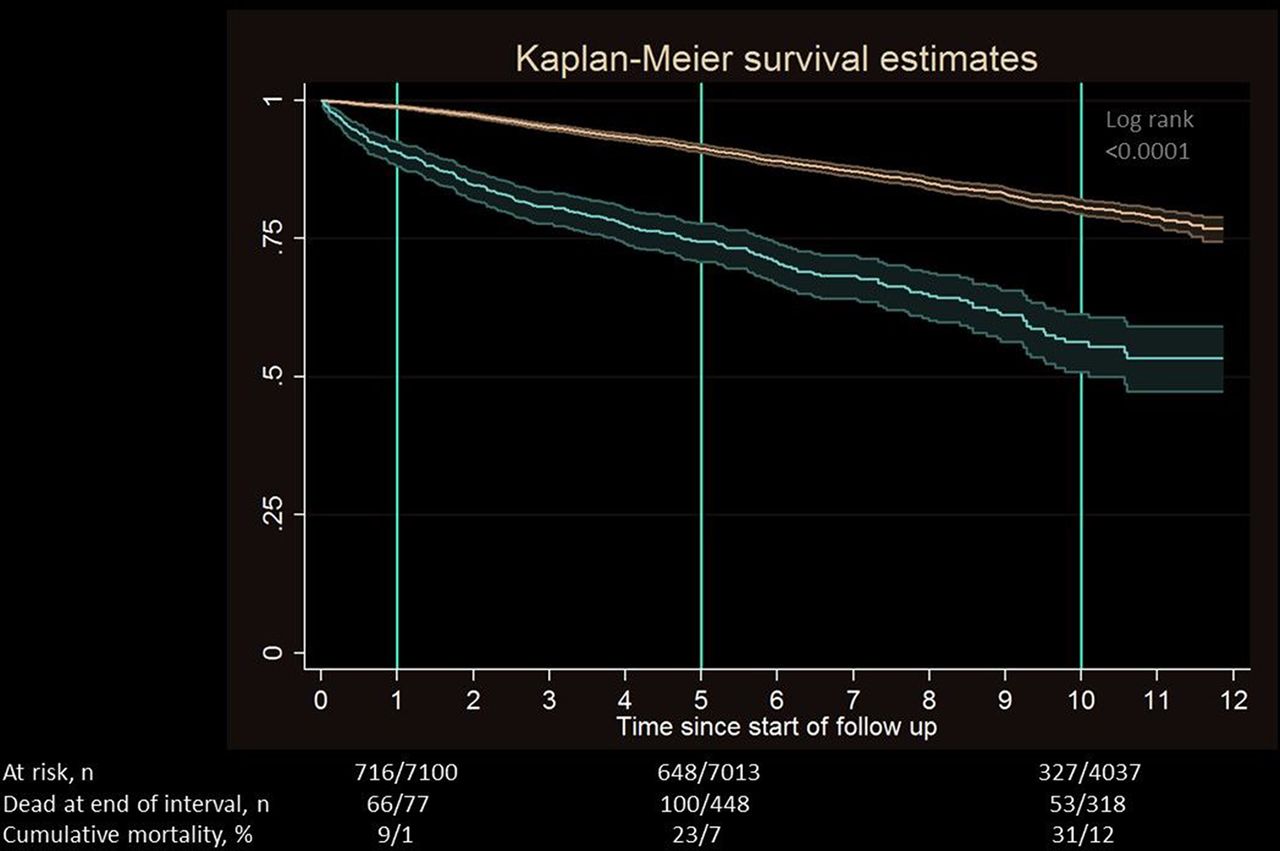
Kaplan-Meier curves of death in idiopathic inflammatory myopathy (red line) and general population (blue line).
Mortality in IIM compared with the general population
After adjusting for age, sex, residential area, birth year and year of diagnosis, the overall HR (95% CI) of death comparing the IIM cohort and the general population, was 3.73 (3.19 to 4.37). The increased risks could be seen in patients with DM as well as the other inflammatory myopathies, in all age groups, and in both women and men with IIM compared with the general population (figure 1). The relative risk of death in IIM versus the general population was highest in the youngest age group (HR <53 years at diagnosis 7.14, 95% CI 4.06 to 12.54) and decreased with age (HR ≥72 years at diagnosis 2.83, 95% CI 2.27 to 3.53) (figure 1). When restricting the outcome to certain infections and parasitic diseases, diseases of the circulatory systems, diseases of the respiratory system, malignant neoplasms and other causes of death, we noted increased risks in all outcomes in IIM overall compared with the risk in the general population (figure 3), although the elevated relative risk for death from certain infections and parasitic diseases was not statistically significant. Adjusting the HRs for educational level did not alter the interpretation of our findings (please be referred to online supplementary tables 8 and 9 for estimates).
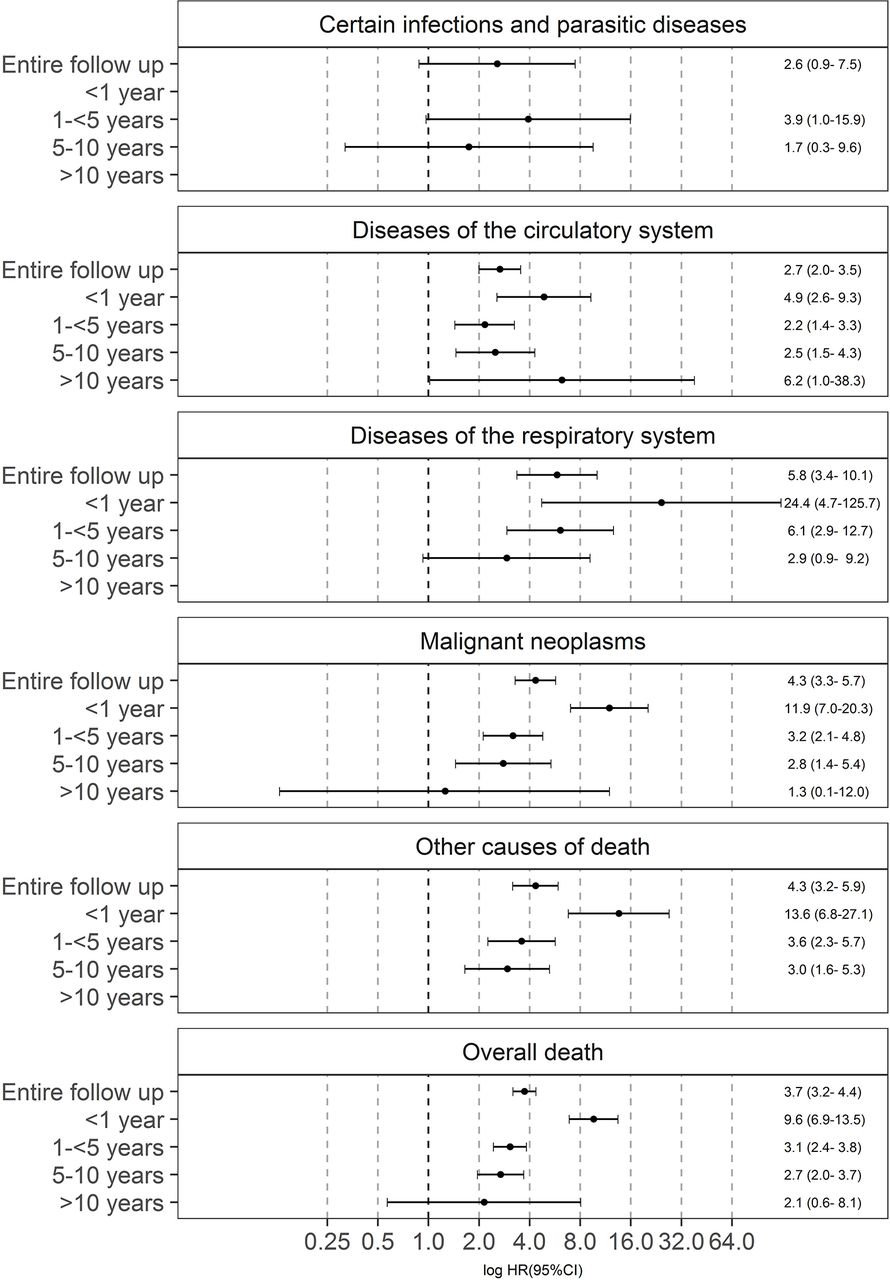
HR and 95% CI comparing the risk of death in patients with idiopathic inflammatory myopathy (IIM) identified in the National Patient Register between 2002 and 2011 and in an individually matched general population comparator. Adjusted for matching factors (sex, residential area and year of diagnosis) and age. Overall and stratified by underlying cause of death and time since IIM diagnosis.
Mortality in relation to time since diagnosis
When we stratified on time since diagnosis, we noted an increased absolute and relative risk of death within the first year of diagnosis, overall and in all cause specific outcomes, except for death from certain infections and parasitic diseases where number of events were few and the CI wide (figure 3, figure 4). For diseases of the respiratory system and malignant neoplasms, the absolute risks were highest within 1 year of diagnosis in patients with IIM and decreased with disease duration. The opposite was seen in the general population regarding diseases of the respiratory system and malignant neoplasms, where the mortality increased with time (figure 4). The relative risk of death was therefore elevated already within 1 year of diagnosis and remained elevated throughout follow-up (figure 3). The risk of death from circulatory diseases was also increased in patients with IIM already within 1 year of diagnosis, point estimate 4.9, and it thereafter increased to a point estimate of 6.2 after >10 years of follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Deaths/1000 person-years (PY) by cause of death and time since start of follow-up in idiopathic inflammatory myopathies (black bars) and the general population (grey bars).
Discussion
In this first nationwide, population-based IIM mortality study, we have demonstrated that IIM indeed is associated with increased mortality. There has been some discussion regarding whether there is an increased mortality in patients diagnosed with IIM in recent years,23 but this study leaves little doubt to this question. This study also demonstrates that the mortality is highest within the first year of IIM diagnosis, and it remains more than doubled compared with the general population throughout a follow-up of over 10 years, although the increased relative risk was not statistically significant after 10 years. After adjusting for age, sex, residential area, birth year and year of diagnosis, a >3-fold mortality risk was seen in IIM compared with the general population. The increased mortality was manifest in IIM overall, and in DM, in all age groups, in all educational levels and in both women and men with IIM compared with the general population. In addition, we found that at the time of death, patients with IIM were younger and to a higher extent women compared with the general population. The cumulative mortality at 1 year and 5 years after diagnosis was 9% and 23%, respectively, in IIM and 1% and 8%, respectively, in the general population. At 10 years, the proportion was 31% and 12%. Not surprisingly, we found the same major causes of death in patients with IIM (malignancies, respiratory and circulatory diseases, as well as musculoskeletal diseases), as previously reported.4 17 30–32
The high mortality in the first year after IIM diagnosis and the thereafter decreasing risk of death was in contrast to the general population where mortality increased with time. The high mortality in the first year after IIM diagnosis refers not unexpectedly to cancer, but importantly also to pulmonary and circulatory disease, the latter which contributes largely to the mortality seen after 5 years with IIM. This emphasises the systemic nature of IIM and that a careful surveillance for cancer and also for lung and heart involvement in newly diagnosed patients with IIM is needed, and furthermore, that a careful monitoring of function of these organs at least during the first year of follow-up is important. These comorbidities are captured both by the disease activity score, myositis disease activity tool, and the disease damage score, myositis damage index, developed by the International Myositis Assessment and Clinical studies group network, and these can be used in clinical practice for surveillance and as support tools for decision making on therapies.33
Mortality studies in patients with IIM diagnosed during the last decade are scarce, and study design differences could partly explain the wide range of estimates previously presented. A majority of the studies lack general population comparators and are therefore not able to relate the risk of death in IIM to the risk of death in the general population, which explains why the data in these reports are presented as 1-year, 5-year and 10-year survival proportions. Three of the more recent publications,13 22 24 including patients partly diagnosed during the last decade, present 5-year and 10-year survival proportions similar to what we have presented in this study, but the most recent and the so far largest study published,23 which studied patients actively followed at Johns Hopkins in 2006–2014 but perhaps diagnosed earlier, presented significantly improved 5-year and 10-year survival proportions (95% at 5 years and 90% at 10 years). They did follow patients from the date of diagnosis, but since patients were required to be actively followed, and therefore alive, sometime between 2006 and 2014, those who were diagnosed before 2006 and died within the first years will not have contributed with events in their follow-up, thus lowering the mortality proportion significantly. This could at least partly explain their seemingly different results. The only so far published study on recently diagnosed patients with IIM, and with a general population comparator but with a smaller study population and lacking the risks in relation to disease duration, presents results that are in line with our main results.20
The main strength of this study is the nationwide, population-based IIM cohort including newly diagnosed patients who are actively followed in contemporary time. Although we are not including patients diagnosed after 2011, we believe the estimations are true for patients diagnosed even in the last years. There are no substantial changes in work up or follow-up of these patients in the last years and could have had an impact on the relative risk. The general population cohort and our possibility to add prospectively collected and linked data on comorbidity and covariates from mandatory public registers with high coverage further increases both the internal and external validity of our finding. The risk of misclassification of the overall outcome death is low since the Swedish Population Register has high validity and coverage.34 Our algorithm to identify all individuals who were exposed (patients with IIM) has been assessed and the robustness of the definition has been tested, and the risk of differential misclassification of exposure is therefore low. A limitation of our study is the overlap of ICD codes used for IBM and PM. Due to this, we could only analyse DM separately and not other subgroups of IIMs. However, the increased mortality rate was found in both DM and in non-DM inflammatory myopathies. The absence of clinical information such as myositis specific autoantibodies and muscle biopsy features and other clinical phenotypes is another limitation of this study, and to assess mortality in relation to such information would have strengthened our results.
Over the last 20 years, the autopsy rates have decreased in Sweden.35 This could lead to a non-differential misclassification of outcome pertaining to the cause-specific assessments of death presented in this study, thus reducing the size of the true association. However, cancer, pulmonary and circulatory manifestations are well recognised comorbidities and causes of death in IIM from previous studies.
In conclusion, mortality rate is increased during the first 10 years after diagnosis of IIM. Novel information from this study is that the overall mortality in IIM is highest during the first year after IIM diagnosis and then decreases, in contrast to the general population where the reversed was seen with an increased mortality rate during a >10-year follow-up period. The major causes of death in patients with IIM are malignancies, diseases of the circulatory and respiratory system, all of them already during the first year after IIM diagnosis. This emphasises that IIM are severe disorders with frequent extramuscular manifestations and that these patients need careful monitoring of muscle strength and of heart and lung function as well as careful surveillance for malignancies.
References
Footnotes
Contributors Study concept and design: MH, IEL and GCD. Acquisition of data: MH and IEL. Statistical analysis: MH. Analysis and interpretation of data, drafting of manuscript and critical revision of manuscript and final approval given: all authors. Obtained funding: IEL and MH. Study supervision: MH.
Funding The Swedish Research Council (Vetenskapsrådet), the Research Agreement on Medical Training and Clinical Research (ALF), Karolinska Institutet, the Swedish Rheumatism Association (Reumatikerförbundet) and the Swedish Society of Medicine (Svenska läkaresällskapet).
Competing interests IEL has received research grants from Astra-Zeneca and Bristol-Myers Squibb and has consultancies from Bristol-Myers Squibb and IDERA Pharmaceuticals. All other authors have declared no competing interests.
Patient consent This is a register-based study.
Ethics approval This study was approved by the Ethical Committee in Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.