Article Text

Abstract
Objective To compare the effectiveness, safety and costs of standard versus individually tailored reduced doses of anti-tumour necrosis factor (TNF) drugs in patients with ankylosing spondylitis (AS) after achieving low-disease activity.
Methods This was a single-centre prospective observational study performed within the ATTRA registry. The anti-TNF dose tapering strategy was chosen by treating physicians, without prespecified protocol. We used propensity score (PS) methodology to identify two cohorts of patients matched for relevant baseline characteristics who were treated with either reduced (n=53) or standard (n=83) doses of TNF inhibitors. One-year outcomes and costs of anti-TNF drugs were compared between both PS-matched cohorts.
Results In the reduced dosing group, the median dose of TNF inhibitor corresponded to 0.67 and 0.5 of the standard dose initially and at 12 months respectively, and 21% of patients required return to standard dosing regimen. The mean change per year in Bath Ankylosing Spondylitis Activity Index, C-reactive protein , Health Assessment Questionnaire Disability Index and Bath AS functional index, as well as quality-adjusted life-year area under the curve were no different between both groups. The HR (95% CI) of reduced versus standard dosing group for relapse and any adverse event was 1.46 (0.66 to 3.19) and 0.56 (0.22 to 1.44), respectively. Mean difference (95% CI) in cost of anti-TNF drugs was €−4214 (−4707 to −3701) per year of treatment in favour of reduced dosing strategy.
Conclusions In patients with AS after reaching low-disease activity, a tailored approach to reduce doses of anti-TNF drugs produced similar clinical outcomes at 1 year, but was substantially less costly.
- Anti-TNF
- Ankylosing Spondylitis
- Treatment
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) is a chronic, immune-mediated disorder characterised by inflammatory back pain, sacroiliitis, spinal inflammation and progressive spinal fusion that may lead to significant disability and reduced quality of life.1–3 In patients with AS, anti-tumour necrosis factor (TNF) therapy has been shown to reduce disease activity, improve physical function and quality of life,4–6 but not to prevent progression of the structural damage.7–10 Treatment with TNF-blockers may be required for long periods of time since attempts to withdraw therapy completely usually lead to clinical relapse of AS after several weeks to months.11 ,12 However, several case series and clinical experience suggest that reduced doses of anti-TNF drugs may be equally effective as standard doses after achieving good control of the disease activity.13 ,14 These reports along with funding restrictions imposed by third-party payers have led many physicians in our centre to individually tailor dose and frequency of anti-TNF drug administration in patients with low-disease activity (LDA). In order to critically assess this empirical strategy, we have conducted an analysis to compare efficacy, safety and direct costs of standard versus individually tailored reduced doses of anti-TNF drugs in patients with AS after achieving LDA.
Methods
Patient population
This is a single-centre study performed within the Czech biologics registry ATTRA analysing data of patients with AS treated between 2007 and 2013 at the Institute of Rheumatology, Prague. The ATTRA registry is a national prospective cohort study with mandatory registration for all patients with AS who start treatment with biologics. The ATTRA study was approved by the Czech Multicentre Research Ethics Committee, and all subjects provided a written consent prior to participation.
Data collection
All patients with active AS, who were starting treatment with anti-TNF therapy, were enrolled for observational follow-up. There were two sources of data collection during the follow-up: physician questionnaires and patient questionnaires. Baseline information was collected regarding demographics, disease severity, concomitant medication and comorbidity. Prospectively collected data included disease activity assessed by Bath Ankylosing Spondylitis Activity Index (BASDAI), physical function assessed by Bath AS functional index (BASFI) and Health Assessment Questionnaire Disability Index (HAQ) and C-reactive protein (CRP) in milligrams per litre (mg/L), dose and administration interval of the anti-TNF drug, concomitant medication and adverse events. The follow-up visits were performed every 3 months.
Treatments
In the Czech Republic, anti-TNF therapy is reimbursed for patients with AS who failed treatment with non-steroidal antirheumatic drugs with BASDAI>4 and CRP≥10 mg/L. Access to biological therapy is limited to 20–30 authorised centres. In 2009, third-party payers had changed their policy allowing centres to treat any number of eligible patients within a prespecified financial budget. Based on previous positive experience, some physicians in our institution reached the consensus to consider careful dose reduction in patients with inactive disease (>6 months). This approach was felt to be clinically safe and ethically justifiable because potential savings transformed the possibility to treat more new active patients. The decision of whether and how to taper (or increase in case of flare) anti-TNF therapy was left solely to the discretion of the treating physician without any prespecified protocol.
Data analysis
The primary aim of this analysis was to compare changes of BASDAI, BASFI and HAQ scores over the first 12 months of treatment with reduced doses of anti-TNF drugs with a group of patients on standard dosing. Secondary outcomes were incidence of specified events (relapses defined by various BASDAI cut-offs, adverse events and switches between anti-TNF drugs), cost of anti-TNF therapy over 1 year and quality of life measured by the Euroqol-5D instrument. In order to allow comparison between standard dosing and individual dose-reducing approaches, we have decided to use the term ‘dose quotient’ (DQ) to describe the proportion of reduced versus standard dose with an assumption that reduced doses in standard administration intervals and standard doses in prolonged administration intervals are roughly interchangeable interventions with regards to the efficacy of anti-TNF drugs. DQ was calculated as (actual dose/standard dose)×(standard dosing interval/actual dosing interval). For example, in a patient receiving 25 mg of etanercept every 14 days instead of the standard 50 mg weekly, DQ=25/50*7/14=0.25, or 25% of the standard dosing regimen.
We have restricted our analysis only to patients with (i) LDA (defined by BASDAI<4) after at least 6 months of treatment with adalimumab, etanercept or infliximab and (ii) at least 12 months of follow-up after dose reduction (or comparable ‘baseline visit’ in the standard dosing group) with BASDAI, BASFI and HAQ scores available.
Statistical methods
In order to obtain two groups of patients with AS with similar characteristics at ‘baseline’ visit (ie, the visit at which the first dose reduction occurred in the reduced dosing group or the most similar visit satisfying the abovementioned inclusion criteria in the standard dosing group), which would differ only by dosing strategy of anti-TNF drugs, we have applied two-level matching techniques (multivariate matching approach15 and propensity score (PS) approach16) described below. In the first step, we aimed to select one ‘baseline’ visit for each patient in the standard dosing group, which would be most comparable to baseline visits in the reduced dosing group. At this point, we selected three most important time-varying parameters reflecting patient's disease status: duration of anti-TNF treatment, BASDAI and HAQ. Baseline visits of reduced dosing group were used to create a pattern (defined by these three parameters) that was then compared with all visits of every patient in the standard dosing group. Using multivariate matching by the nearest neighbour algorithm based on Euclidean distance we were able to identify the most appropriate visit for each standard dosing group patient and such visits have been then considered to be the baseline visits of standard dosing group patients. Since the Euclidean distance depends on the scaling of covariates, these were appropriately transformed and standardised to z-scores. No patient was discarded from the analysis at this step.
In the second step, we applied a PS matching procedure to balance all relevant available demographic and clinical baseline characteristics between the reduced dosing and standard dosing group at the time point selected by the multivariate matching approach described above. The baseline covariates balanced by the PS model included patients’ age, gender, baseline activity, baseline function, disease duration, duration of anti-TNF therapy and number of previous anti-TNF drugs (all parameters used to construct the PS are shown in the online supplementary figure S1). Highly asymmetric covariates were transformed and interactions of covariates were incorporated as appropriate. At this step, we allowed calliper of 0.5 to discard poor matches. The balance of the baseline characteristics was explored in the primary and the matched dataset by computing the standardised differences and additionally by testing statistical significance of differences.17 Participants with missing data in baseline characteristics (excluding covariates of primary interest: BASDAI, HAQ, BASFI) were included in the analysis by using multiple imputations by Markov chain Monte Carlo method with 30 imputations obtained after 20 iterations.18 Variables included in imputation models were all baseline covariates (variables with missing data were imputed and used as predictors, variables with complete data were used as predictors only).
Non-parametric Mann–Whitney U test and unconditional z-pooled test were used when comparing continuous and categorical variables, respectively. Change in the disease activity during 1 year was modelled using linear mixed effects regression model. Survival analysis of time to relapse and time without adverse event was performed by Kaplan–Meier method and HRs were estimated using Cox proportional hazards model. Kaplan–Meier estimator was applied in multistate model of aliquot change of reduced dosing group. All computations except the matching procedures were performed using IBM SPSS Statistics V.21. The matching procedures were performed in software R (V.2.14.2) with package ‘MatchIt’.19
Annual costs of anti-TNF therapy and costs of anti-TNF therapy per quality-adjusted life-years (QALYs)
To estimate the annual costs of anti-TNF therapy, cumulative DQ in patients from the reduced dosing group was multiplied by the average cost of 1-year full-dose anti-TNF therapy in the Czech Republic of €12 000. We have also performed a simplified cost utility analysis of both anti-TNF dosing approaches assuming that other direct and indirect costs were equal in both groups. Since the directly collected EQ-5D data after baseline visit suffered from a large number of missing values, life-years were transformed into utility using a published relationship (utility=0.923–0.004* BASFI–0.004*BASDAI) derived from the BASDAI, BASFI and EQ-5D data collected during a randomised control trial with etanercept.20 ,21 QALYs were calculated assuming linear interpolation between measurement points and calculating the area under the curve to give a QALY score per patient over the 1-year horizon.22 Additionally, we derived another relationship from the whole ATTRA registry using generalised estimating equations (N=1679 patients with AS; utility=0.952—0.055*BASDAI—0.206*HAQ) for the sake of sensitivity analysis. Incremental cost (C) and effectiveness (E) of reduced dosing strategy were calculated as a difference from standard dosing strategy in mean cost and mean QALY score obtained after 10 000 iterations of bootstrap resampling. Incremental cost-effectiveness ratio (ICER) was then calculated as C/E. Net monetary benefit (NMB) was calculated as (E * WTP)–C. Willingness to pay (WTP) in the Czech Republic was estimated according to the WHO recommendation as three times the gross domestic product per capita (€43 250).
Results
Study population
As of January 2013, there were 386 patients with AS treated by anti-TNF therapy in our centre. In total, 82 patients with attempted dose reduction and 162 patients with standard dosing satisfied the entry criteria for this analysis (unbalanced dataset). By the above-described two-step multivariate matching method, we have identified 53 patients with attempted dose reduction and 83 patients with standard dosing, who had comparable demographic and clinical parameters at baseline visit (balanced dataset). The baseline parameters of both treatment groups in the balanced dataset are shown in table 1. The comparison between balanced and unbalanced datasets is demonstrated in the online supplementary figure S1 and table S2.
Baseline characteristics
Changes in the dosing during the 12 months of observation in the reduced dosing group
Participating physicians opted to prolong the administration interval (most often with etanercept) in 80.7%, reduce the dose (most often with infliximab) in 14.0% or used both approaches in 5.3% patients. DQ ≤0.5 was reached in 61.5% patients treated with etanercept, 0.0% with adalimumab and 23.5% with infliximab. As shown in figure 1, at baseline visit the median DQ was 0.67 and 0.50 at 12 months. In 21% of patients, the DQ was further decreased during 1 year of observation, while the same proportion of patients required a return to standard dosing regimen.
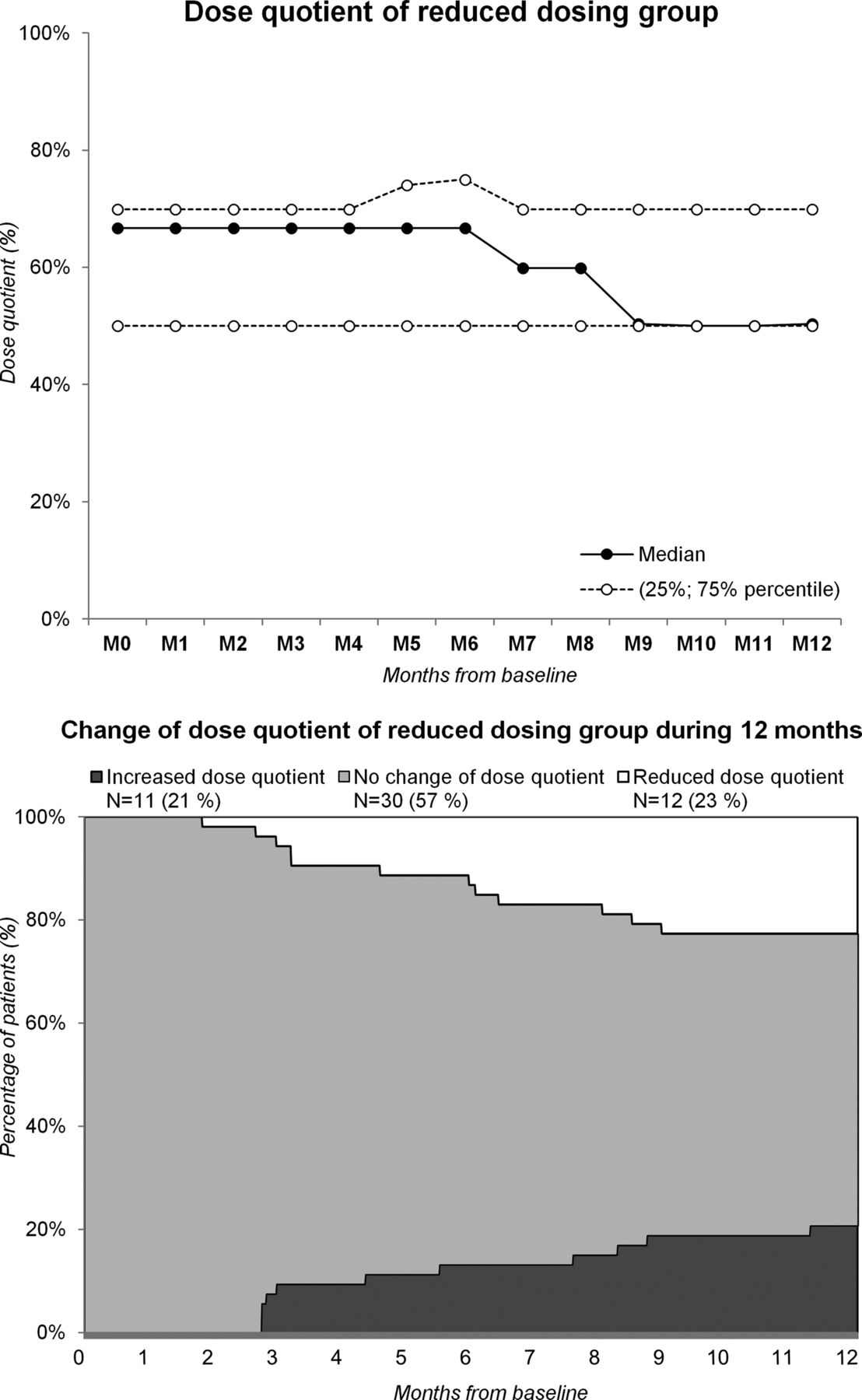
Dose quotient of reduced dosing group.
Relapses, complications and switches between anti-TNF drugs
The incidence of relapses, reported adverse events, severe adverse events, infections, infusion reactions and switches between anti-TNF drugs did not significantly differ between both treatment groups (table 2, figure 2).
Incidence of relapses (defined by different BASDAI cut-offs), switches of anti-TNF drugs and adverse events
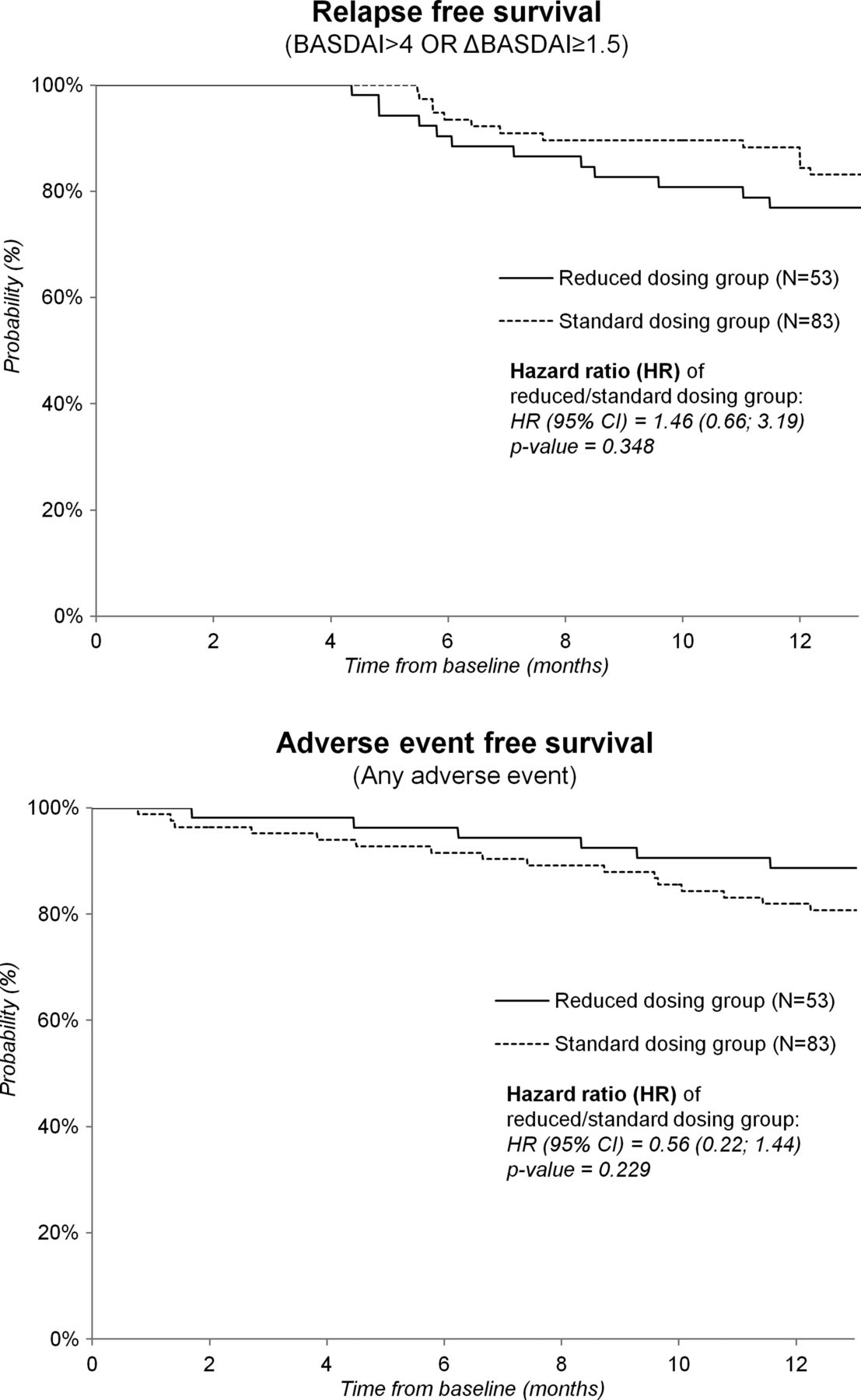
Relapses and adverse events. BASDAI, Bath Ankylosing Spondylitis Activity Index.
Change in BASDAI, HAQ and BASFI scores and CRP during the 12 months of observation
As shown in table 3, all parameters of activity (CRP, BASDAI) and function (HAQ, BASFI), as well as their mean change, were similar between both treatment groups at baseline and at 12 months of observation. A sensitivity analysis comparing proportions of patients in both groups with improvement or deterioration in BASDAI, BASFI or HAQ scores by more than a published threshold of the minimally clinically important difference23 ,24 yielded similar results (see online supplementary table S3).
Measures of activity/function, quality of life and costs of anti-TNF therapy over one year of observation
Quality of life and costs
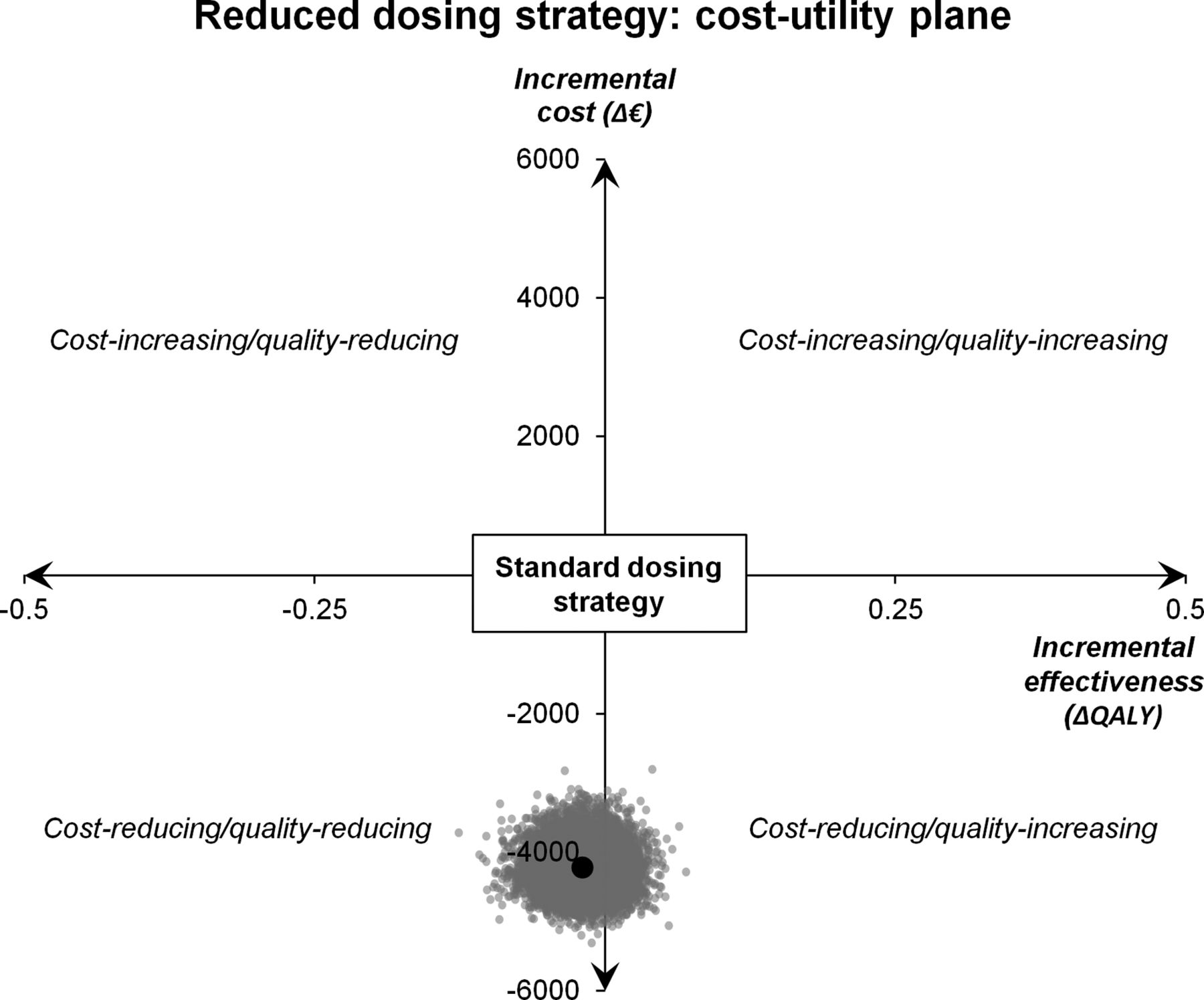
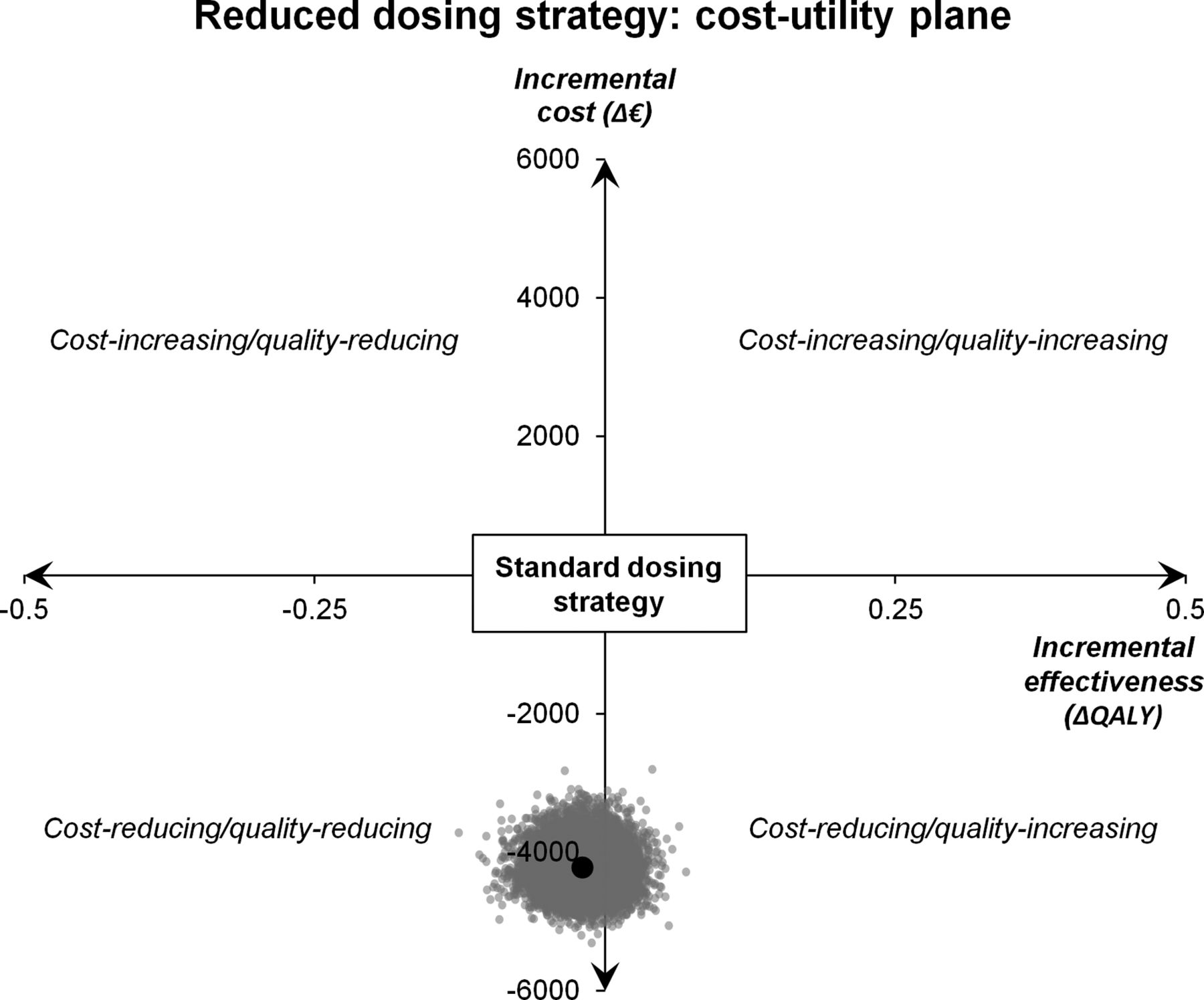
While the quality of life (assessed by EQ-5D, derived from BASFI/BASDAI) did not differ between both groups, the annual costs of treatment with anti-TNF drugs were, as expected, significantly different (table 3 and figure 3); the average annual cost of anti-TNF therapy in the reduced dosing group was approximately two-third of standard dosing group. Consequently, ICER (€211 426) and NMB (€−3354) of standard versus reduced dosing strategy was high and negative, respectively.
{kind=link}
{kind=link}
{kind=link}
Cost utility plane: reduced versus standard dosing strategy. QALY, quality-adjusted life-year.
Sensitivity analyses
The proportion of missing baseline data was low, but about 33% of EQ-5D utilities (mainly from the follow-up period) were missing. We conducted sensitivity analyses (i) restricted to patients with no missing baseline data, (ii) restricted to patients exposed only to one anti-TNF drug and (iii) based on utilities calculated with the ATTRA registry derived equation, none of which did alter the results (see online supplementary file S4).
Discussion
To our knowledge, this is the first study comparing the outcomes of patients with AS with anti-TNF dose down-titration and standard dosage. We have found that patients with AS treated by individually tailored doses of anti-TNF drugs had similar clinical outcomes as matched controls over 1 year of observation. However, the annual cost of anti-TNF therapy was substantially lower in the group with attempted dose reduction.
Previous observational cohort studies have shown that complete discontinuation of long-term therapy with anti-TNF agents in patients with AS frequently led to a clinical relapse of the disease after several weeks to months, and is therefore not a feasible therapeutic approach in most patients.11 ,12 Another strategy for the management of patients with AS achieving an LDA state on anti-TNF therapy is dose reduction.13 ,14 Navarro-Compán et al13 used several etanercept dose reduction strategies in 16 patients with AS, all of whom maintained good disease control and did not require dose escalation after a mean follow-up of 26 months. Lee et al14 reported similarly good outcomes in 109 Korean patients with AS treated with progressively tapered doses of etanercept down to 25 mg every 12 days with a mean follow-up of 21 months. Our results support and further extend the findings of these studies, indicating that low-dose regimens may be considered as a ‘maintenance’ strategy after successful ‘induction’ treatment with standard doses of anti-TNF drugs in patients with AS. In our study, the matched design and uniform prospective collection of outcome data in a relatively large cohort of patients with AS enables a cautious attempt to compare the standard and individually tailored dosing strategies in a 1-year horizon. Within this timeframe, patients in both groups fared very similarly, as indicated by the conventional parameters of activity and function. These findings support our assumption that other direct and indirect costs (save for the cost of anti-TNF therapy) were also similar because BASDAI and BASFI are validated and established tools in AS and have been shown to correlate strongly with both disease costs and utilities.25 ,26 Calculated indices of cost-effectiveness of standard versus reduced dosing strategy appeared far beyond the conventional thresholds of societal acceptability.
This study was not a randomised clinical trial but rather an observational study of a standard versus a broadly defined dose reduction treatment strategy in a real-world setting and therefore, does have some limitations that must be considered. Since the treatment strategies were not assigned randomly to patients, statistical models were used to account for the differences in baseline disease severity in order to minimise the selection bias. However, these models are dependent on the covariates entered into the model and therefore, we cannot exclude the effects of unmeasured confounding. Also, we cannot exclude the possibility that patients with less severe disease may have been selected to down-titration strategies on the ground of clinical parameters not captured by the measures collected in the registry database. We have also encountered a problem that there are no universally accepted standardised criteria defining remission and flare in patients with AS, which makes comparison with previously published studies difficult. Unfortunately, we were not able to use the newly proposed ASDAS tool due to the fact that not all required variables were collected in our registry. However, both BASDAI and BASFI are established and valid measures of disease activity and function in patients with AS.
The study sample was selected from a single tertiary academic centre, which may limit the possibility to extrapolate our findings to patients with AS treated elsewhere. More importantly, the observational period of 1 year, chosen for practical reasons, is inadequate to draw any firm conclusions concerning long-term outcomes and cost-effectiveness.
Our study describes outcomes of several down-titrating strategies, with different anti-TNF drugs. In fact, there may be substantial differences between individual anti-TNF drugs and dose reduction strategies, optimal starting points, as well as suitable patients. Interestingly, the lowest dosing quotients were reached in patients treated with etanercept, but the design of our study does not allow for discrimination between true pharmacological properties of the respective anti-TNF drugs or the dose reduction strategies.
Although the pool of evidence supporting the safety and efficacy of low-dosing regimen in patients with AS is growing, several theoretical concerns remain.
Theoretically, sustained low-grade inflammation in patients on reduced doses may, in the long term, lead to more severe structural damage or be associated with atherosclerosis progression. Also, lower or fluctuating blood levels of anti-TNF drugs may potentiate immunogenicity of anti-TNF drugs, thus increasing the risk of secondary failure and hindering future attempts to treat disease flares. However, over 1 year of follow-up we have not observed a difference in mean CRP levels, and all patients who required dose re-escalation reached disease activity comparable with that prior to dose reduction. Nonetheless, patients on lower than standard doses of anti-TNF drugs should be monitored closely because 21% of patients in our study required re-escalation of anti-TNF therapy (not necessarily because of overt flare). This proportion may increase with time, thus limiting the possibility to predict potential savings beyond the timeframe of our study. Our results need to be reproduced in larger studies with longer follow-up time before the reduced dosing strategy in patients with AS after reaching LDA could be universally recommended. A multicentre, double-blinded, randomised controlled trial would be probably the best way to confirm the non-inferiority and safety of this approach.
In conclusion, the results of our study indicate that over 1 year using individually tailored reduced doses of anti-TNF drug appears to be similarly effective, but substantially less costly compared with standard dosing in maintaining low level of activity and preserving physical function in patients with AS after reaching state of inactive disease. Such an approach allowed us to save more than one-third of costs over 1 year and treat more patients within a preset financial budget.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Collaborators Radim Bečvář; Dana Tegzová; Jiří Štolfa; Ladislav Šenolt; Olga Šléglová; Andrea Pavelková; Radka Svobodová; Olga Růžičková; Liliana Šedová; Lucie Goerojová; Olga Kryštůfková; Gabriela Šimková; Zuzana Urbanová; Helena Dejmková.
Contributors JZ designed the study and wrote the draft. MU performed the statistical analysis. KS, SF, KJ, HM, JV and KP substantially contributed to the acquisition and interpretation of presented data, revised and approved the final draft.
Funding This work was supported by the project (Ministry of Health, Czech Republic) for conceptual development of research organisation 00023728 (Institute of Rheumatology).
Competing interests None.
Ethics approval This study deals only with anonymised clinical data collected in the ATTRA registry. All subjects enrolled in the ATTRA registry gave their written consent for participation. The ATTRA study (and the written consent) was approved by the Czech Multicentre Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.