Article Text

Abstract
Objective: Systemic sclerosis (SSc) is a generalised autoimmune disease, causing morbidity and a reduced life expectancy, especially in patients with rapidly progressive diffuse cutaneous SSc. As no proven treatment exists, autologous haematopoietic stem cell transplantation (HSCT) is employed as a new therapeutic strategy in patients with a poor prognosis. This study reports the effects on survival, skin and major organ function of HSCT in patients with severe diffuse cutaneous SSc.
Patients and methods: A total of 26 patients were evaluated. Peripheral blood stem cells were collected using cyclophosphamide (4 g/m2) and rHu G-CSF (5 to 10 μg/kg/day) and were reinfused after positive CD34+ selection. For conditioning, cyclophosphamide 200 mg/kg was used.
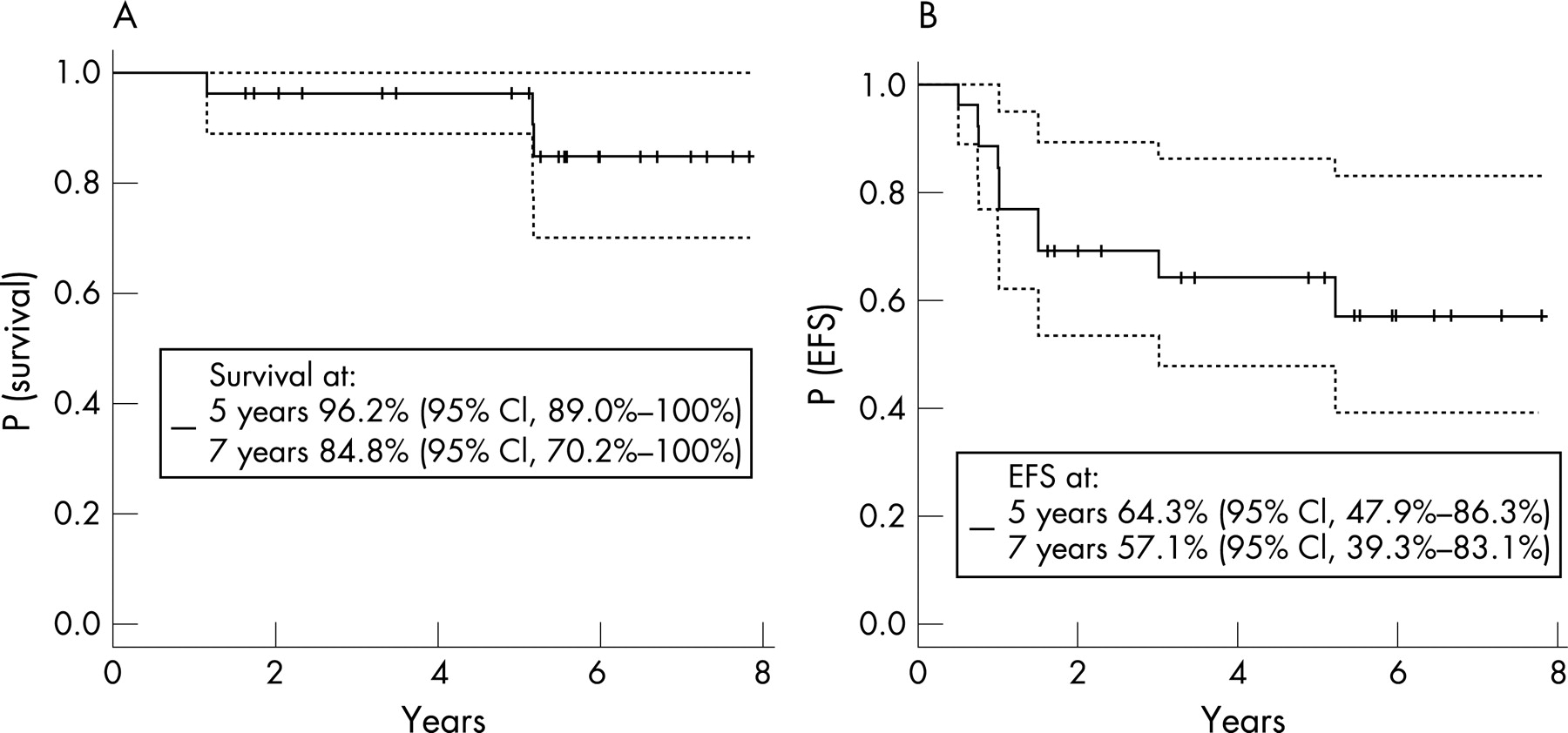
Results: After a median follow-up of 5.3 (1–7.5) years, 81% (n = 21/26) of the patients demonstrated a clinically beneficial response. The Kaplan–Meier estimated survival at 5 years was 96.2% (95% CI 89–100%) and at 7 years 84.8% (95% CI 70.2–100%) and event-free survival, defined as survival without mortality, relapse or progression of SSc, resulting in major organ dysfunction was 64.3% (95% CI 47.9–86%) at 5 years and 57.1% (95% CI 39.3–83%) at 7 years.
Conclusion: This study confirms that autologous HSCT in selected patients with severe diffuse cutaneous SSc results in sustained improvement of skin thickening and stabilisation of organ function up to 7 years after transplantation.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is a generalised connective tissue disorder characterised by vascular lesions, resulting in thickening of the skin, fibrotic degenerative changes in muscles, joints and viscera, mainly the intestinal tract, the heart, the lungs and the kidneys.1 2 Although its exact pathogenesis remains unknown, this autoimmune disease is characterised by predominant T-cell activation, the production of specific auto antibodies, and cytokine release.3 4 Two main clinical subsets, namely limited and diffuse cutaneous forms, can be distinguished by the extent of skin involvement, their autoantibody profile and the pattern of organ involvement. The mortality of SSc is high, with a 5-year mortality rate of at least 30%.5 6 In rapidly progressive diffuse cutaneous SSc the 5-year mortality is estimated to be 40–50%.5–9 In these patients, the cause of death is secondary to pulmonary, cardiac and renal involvement.5 6 10 To date, no treatment has been shown to prevent disease progression and reverse fibrosis, but immunosuppressive therapy, given at an early stage of the disease, could result in disease improvement. Reduction of the skin score and stabilisation or improved global response was suggested by one small placebo controlled study with methotrexate.11 This was later confirmed in a second, larger placebo-controlled randomised study.12 More recently, a large, double-blind placebo controlled trial with oral cyclophosphamide in SSc patients with interstitial lung disease showed a statistically significant, although clinically modest, effect, namely a reduction of decline of forced vital capacity (FVC).13 A similar study with monthly intravenous bolus of cyclophosphamide and prednisolone 20 mg every other day for 6 months, followed by oral azathioprine (2.5 mg/kg/day) for 6 months showed positive effects on the FVC, but not on carbon dioxide diffusion lung capacity (DLCO) or abnormalities on high-resolution CT-scan.14
Since 1996, autologous peripheral blood stem cell (PBSC) transplantation has been employed worldwide with a low early mortality of <5%.15–18 Based on these data, we have used intensive myelo- and immunosuppression followed by autologous haematopoietic stem cell transplantation (HSCT) to treat severe SSc.15 17 19 Since 1996, approximately 1000 PBSC transplantations for autoimmune diseases have been reported20 21 with 140 SSc patients in the EBMT (European Group for Blood and Marrow Transplantation) and EULAR (European League Against Rheumatism) database as to March 2007. The early results from the phase I/II clinical trials showed that HSCT is feasible in carefully selected patients with diffuse SSc.16 19 22 23 In 2004, a follow-up report from the EBMT-EULAR database, consisting of different centres and treatment schemes, showed positive responses at 3 years in two thirds of 57 patients with an early treatment related mortality of 8.7%.15 We describe here the long-term follow-up results of all the Dutch and French patients included in two similar phase I/II trials, using uniform eligibility criteria and a single transplantation protocol.24 The specific aims of this study were to evaluate the survival and the durability of responses up to 7 years of follow-up in SSc patients treated by autologous HSCT.
PATIENTS AND METHODS
We report results from patients with SSc, treated by HSCT at the Radboud University Nijmegen Medical Centre and the Leiden University Medical Centre in The Netherlands and at the Hôpital Saint-Louis in Paris, France, with at least 6 months follow-up after HSCT. All patients fulfilled the ACR preliminary criteria for SSc and had the diffuse cutaneous form.3 Patients were eligible if they had the following characteristics: (a) age <66 years and (b) rapidly progressive disease ⩽2 years duration with a modified Rodnan skin score (mRSS) above 20, plus ESR >25 mm/first h and/or Hb <11 g/dL, not explained by other causes than active SSc or (c) a disease duration >2 years plus a progression of the mRSS (>20%) plus major organ involvement related to SSc as defined by either: (1) lung involvement: with a vital capacity (VC) or DLCO below 70% predicted, or a mean pulmonary artery pressure (PAP) above 40 mmHg (measured by echocardiography); (2) digestive tract involvement: with serum albumin <25 g/L or weight loss exceeding 10% body weight in the preceding year; (3) kidney involvement: with 24-h urinary protein above 0.5 g or serum creatinine above 120 μmol/L. The exclusion criteria were: uncontrolled arrhythmia, echocardiographic left ventricular ejection fraction (LVEF) <50% or mean PAP >50 mmHg, DLCO <45% of predicted, creatinine clearance <20 ml/min, platelets <80 000/mm3, haemorrhagic cystitis, HIV or HTLV1 seropositivity, malignancy, pregnancy, a cardiac or vascular prosthesis, and no vascular access.19 These studies were approved by the local ethics committees.19 After obtaining written informed consent, eligible patients were included in the protocol.
Pre-treatment evaluation
Pre-transplant evaluation included: (1) disease characteristics such as the disease duration (in years from the first non-Raynaud symptom), autoantibody profile, previous disease specific treatment and determination of WHO performance status, grade 0–5; grade 0 being a patient who is fully active without restriction; grade 1 being a patient who is restricted in physically strenuous activity, but ambulatory and able to carry out work; grade 2 representing a patient who is ambulatory and capable of all self-care but unable to carry out any work, up and about >50% of the waking hours; grade 3 being a patient who is capable of only limited self-care, confined to bed or chair >50% of waking hours; grade 4 representing a patient who is completely disabled and cannot carry out any self-care, who is totally confined to bed and chair; and grade 5 a deceased patient;25 (2) organ involvement according to: (a) the extent of skin sclerosis using the mRSS;10 (b) chest x ray or high-resolution CT-scan, pulmonary function tests with total lung capacity (TLC), VC, forced expiratory volume in first second (FEV1), and DLCO, all in % of predicted; (c) echocardiography to measure LVEF (%) and mean PAP (mmHg); (d) estimation of the creatinine clearance according to the method of Cockcroft and Gault.26
Stem cell mobilisation, collection and selection: transplantation procedure
The transplantation procedure was performed as previously reported.19 In short, the mobilisation and collection of PBSC was performed with 4 g/m2 cyclophosphamide followed 4–5 days later by rHu G-CSF (Lenograstim®, Aventis and Chugai Pharma France or Filgrastim®, Amgen, Thousand Oaks, California, USA) 5 or 10 μg/kg/day until the last apheresis. Autologous PBSC were collected when CD34+ cells were above 20/μl in peripheral blood. At least 9.5×106 CD34+/kg had to be collected by successive daily apheresis to obtain 7×106 CD34+/kg for positive selection (using Nexel Isolex®300i Stem Cell Collection System at St Louis Hospital and Clinimacs® of Miltenyi in Nijmegen and Leiden) and 2.5×106 CD34+/kg for haematopoietic rescue.27 The graft was 4–5 log T-cell depleted. Conditioning was performed at least 4 weeks later using cyclophosphamide at 50/mg/kg/day from day –5 to day –2 prior to PBSC reinjection.
Clinical follow-up
To assess the survival and disease response to treatment, clinical evaluation was conducted at least every 6 months, consisting of the same investigations that were used in the pre-transplantation evaluation. Event-free survival (EFS) was defined as survival without mortality, relapse or progression of SSc, resulting in heart, lung or kidney dysfunction. Organ dysfunction was defined as follows: heart: an echocardiographic LVEF<40% or mean PAP >50 mmHg; pulmonary: respiratory failure with a paO2 <8 kPa/60 mmHg; kidney failure necessitating dialysis. Response to therapy was assessed segregating major (MR) or partial (PR) responses, no response, disease progression or relapse as previously described.19 A major response was defined as: (1) performance status at 0; plus (2) decrease >50% in the mRSS and/or an increase in FEV1 >30%, plus an LVEF >45% without any pericardial effusion and serum creatinine ⩽ baseline values. A partial response was defined as: (1) performance status ⩽1; plus (2) decrease 25%–50% in mRSS and/or an increase in FEV1 15%–30%, plus an LVEF >45% with no or small pericardial effusion plus serum creatinine at baseline values or <180 μmol/L. No response was defined by stable disease compared to inclusion. Relapse was defined by the onset of progression after prior response. Disease progression was defined as an increase in mRSS >25% compared to the baseline values, a decrease in VC or DLCO >15% and/or major organ dysfunction as defined above.
Statistical analysis
Categorical variables were summarised as counts and percentage, while numerical variables were summarised as median and full range. Outcomes were reported for each follow-up year. Groups were compared using Fisher’s exact test for the categorical variables and non-parametric paired Wilcoxon rank sum test for numerical variables. The significance level of p values was set to 0.05. The survival curve was calculated by the Kaplan–Meier method. A piecewise linear mixed model was used to represent the mRSS over follow-up, with the first linear part from inclusion to the first year of follow-up, and the second part from the first up to the seventh year of follow-up.28 Random subject main effect and slope were added to the model, to account for the correlation between measurements on the same subjects. All computation analyses were performed using R (http://cran.r.project.org) version 2.1 for Windows.
RESULTS
Patients
A total of 26 patients (19 females and 7 males), median age 42 (16–65) years, with diffuse cutaneous SSc were included in the study (11 from Nijmegen, 10 from Paris and 5 from Leiden) from March 1998 to May 2004. Table 1 shows baseline patients’ clinical characteristics. Two patients included were subsequently found as having one of the exclusion criteria (one with a DLCO at 21% and one with a LVEF of 46%), which were considered as violation of the protocol but could be kept in the study according to the study committee advice. A total of 12 patients had early diffuse SSc, with a median disease duration of 1.4 (0.8–2) year, and 14 patients had progressive organ involvement with a median disease duration 3.7 (2.1–13) year. The median mRSS of 32 (9–51) and 85% (n = 22) had an mRSS ⩾20. Pulmonary involvement was present in 65% (n = 17), and 19% (n = 5) had a creatinine clearance below 70 ml/min. Significant weight loss was one of the eligibility criteria in 19% of the cases (n = 5). All but three patients had been treated with immunosuppressive agents prior to the HSCT (methotrexate, prednisolone, cyclophosphamide with a maximum of 9 gram per patient, d-penicillamine, colchicine, azathioprine, sulphasalasine, interferon α, infliximab, and anti-TGF β). These agents were discontinued at least 1 month prior to PBSC mobilisation. In five patients relevant co-morbidity, such as diabetes mellitus (n = 1), asthma (n = 2) and ischaemic heart disease (n = 2) was present.
The treatment regimen is described in table 2. In one patient, PBSC mobilisation failed, but enough bone marrow stem cells were harvested 4 weeks later and autologous bone marrow transplantation was performed with antilymphocytes globulins and cyclophosphamide.15 Another patient received PBSC transplantation without T cell depletion due to technical problems at the time of the selection procedure.
Survival
The early mortality, within 6 months after HSCT, was previously reported for all patients.15 19 In short, among 28 severe SSc patients treated by HSCT 2 died within 6 months (7.1%), leaving 26 patients with at least 6 months of follow-up after HSCT. The causes of death of these two patients was considered as treatment related at 1 month for one patient and due to disease progression for another at 6 months after HSCT. As illustrated in fig 1, the probability of survival of SSc patients with at least 6 months follow-up after HSCT was 96.2% (95% CI 89–100%) at 5 years and 84.8% (95% CI 70.2–100%) at 7 years. At the time of analysis, no patients were lost to follow-up. After a median follow-up of 5.2 (1–7.5) years, death from disease progression occurred in 2 patients (8%): both from relapse at 18 months after transplantation, one after initial PR and the other after initial MR. A third patient, a heavy smoker, died from small cell lung cancer 64 months after HSCT. Among the others showed 35% (n = 9) sustained MR, 50% (n = 13) sustained PR, and 3% (n = 1) progressed after PR. All together, the event-free survival (EFS) for the patients with at least 6 months of follow-up after autologous HSCT was 64.3% (95% CI 47.9–86.3%) at 5 years and 57.1% (95% CI 39.3–83.1%) at 7 years (fig 1).
Long-term morbidity
Infectious complications occurred in 19% (n = 5) of the patients, caused by Herpes Zoster reactivation (n = 3) and atypical mycobacterium (n = 2). One patient with persistent pancytopenia after HSCT received 16 units of red blood cells and recovered suboptimal blood counts after discontinuing simultaneous treatment with co-trimoxazole. One patient developed a basal carcinoma of the facial skin at 4 years after transplantation, which was surgically removed.
Clinical evolution
The WHO performance status improved throughout the follow-up, from baseline values at median 2.12 (0–4, n = 26) to 0.60 (0–2, n = 15 p<0.05) after 5 years of follow-up (fig 2).

A significant fall in mRSS was observed up to 7 years after HSCT with faster regression within the first year and sustained fall thereafter. The representation of the mRSS by a linear mixed model resulted in a median mRSS decrease of 11.57 units in the first year (p<0.001) and of 2.57 units per year after that (p<0.001) (tables 3 and 4 and fig 3). A significant decrease (>25%) in mRSS was achieved in 73% (n = 19/26) of the patients after 1 year and in 94% (15/16) after 5 years.

Repeated assessments of pulmonary function parameters were obtained in all patients every 6 months with 15 patients completing 5 years of follow-up. The median VC (% predicted) was 76% (37–143%) at inclusion and 73% (33–114%) after 5 years of follow-up. In comparison with baseline values for all patients, there was no significant change in FEV1 or DLCO during follow-up. Cardiac and renal function remained stable during follow-up (tables 3 and 4).
After autologous HSCT 81% (n = 21/26) of the patients with at least 6 months follow-up demonstrated a positive response at one year with either major (n = 5) or partial (n = 16) response, whereas 5 patients had no response (fig 4).19 Longer follow-up showed that after 5 years 82% (n = 14/17) had a response to the transplantation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relapses occurred in 28% (n = 6) of the initial major (n = 2) or partial (n = 4) responders within 2.7 (range 2–4) years after transplantation. Treatment of the relapses consisted of either corticosteroids (n = 3), corticosteroids plus mycophenolate-mophetil (n = 1), or corticosteroids plus mycophenolate-mophetil plus cyclosporine A (n = 2). After a median follow-up of 5.3 (1–7.5) years, 88% (n = 23/26) of the patients with at least 6 months follow-up after HSCT were alive: 35% (n = 9) with MR, 50% (n = 13) with PR, and 3% (n = 1) with progression after PR.
DISCUSSION
The data presented here were obtained from the combined Dutch–French database of patients with SSc treated by HSCT in a phase I/II study. The primary objectives of this study were to assess the long-term survival. The secondary objectives were to evaluate the disease response after HSCT, using previously published criteria,19 to assess the evolution of the functional status, the skin involvement as well as organ involvement.
The cohort of patients studied represented a group with SSc and poor prognosis, as assessed by their initial high mRSS, the number of patients with lung disease and the presence of anti-topoisomerase auto antibodies.6–9 29–39 The treatment regimen, as well as clinical follow-up after transplantation employed in the three hospitals were similar. To our knowledge, this is the largest cohort of severe SSc patients studied, with a median follow-up period of 5.3 years after autologous HSCT, providing valuable information on long-term outcome.
Benefits and mortality
This study illustrates the benefits that can be observed after HSCT in severe SSc patients. The adequate selection of patients with a poor prognosis, but without irreversible organ damage, is important to reduce the treatment risks and to improve the treatment success.22 29 After a median follow-up of 5.3 (1–7.5) years, death from disease progression occurred in 8% of our SSc patients. This rate is strikingly lower compared to the 5-year mortality rate estimated at 40% in such severe SSc patients, according to a recently published meta-analysis.6 The positive effect of HSCT on survival rate needs to be interpreted with care, due to a wide range in the duration of patients’ follow-up and the uncontrolled nature of this study, but the results are encouraging.
Autologous HSCT induced a rapid skin score decline. To our knowledge, no other therapeutic intervention in diffuse SSc has ever shown such a rapid and sustained improvement in skin condition. In our cohort, a significant decrease in mRSS was achieved in 73% after 1 year and in 94% (15/16) after 5 years. The skin thickness in patients with early SSc may improve spontaneously. However, the time span of such changes has always appeared much slower than observed within the first year after autologous HSCT.40 Further studies will help to clarify the pathological mechanisms associated with regression of skin sclerosis as recently shown after autologous HSCT in SSc.41
Interstitial pulmonary disease accounts for a large part of mortality in SSc patients. The effects of current treatment protocols of interstitial pulmonary disease in SSc is not very successful.13 In our study 65% of the patients with severe SSc had significant lung involvement at inclusion. All pulmonary function parameters remained stable after 5 and 7 years of follow-up.
The strongest effect of treatment by HSCT was observed on functional status, as assessed by the WHO performance status, possibly due to improvement of the skin condition. Five years after transplantation, the percentage of patients with a WHO performance status of zero had increased to 56% compared to 4% at baseline. Therefore, HSCT treatment showed a sustained positive effect on the combination of functional status, skin, lung, heart and kidney involvement.19
Our study has several limitations. First, this uncontrolled study and the promising results obtained in a relatively small number of patients will have to be confirmed in larger numbers as aimed in the two ongoing phase III randomised trials comparing autologous HSCT to monthly cyclophosphamide intravenously, the European ASTIS trial and the North American SCOT study. Nonetheless, to our knowledge this is the largest cohort of SSc patients studied after autologous HSCT, providing a rather good estimation of the long-term outcome and treatment effects at 5 years. Secondly, the natural history of SSc in some patients may lead to a more indolent disease after a period of active disease, resulting in stabilisation of organ functions and reduction of the mRSS. However, no study has yet found the predictive factors to distinguish such patients. Furthermore, large cohorts of SSc patients prospectively studied by Steen37 and Scuzel42 have shown the very severe spontaneous evolution of SSc in some cases.
In conclusion, for the first time this extended report shows the long-term follow-up results of HSCT in patients with severe SSc. It is confirmed that this treatment is feasible with acceptable toxicity.15 19 22–24 Clinical significant and sustained improvement was found on the skin condition and functional status with pulmonary cardiac and renal function stabilisation. Combined results allowed us to show that the majority of the patients experienced a sustained complete or partial remission of SSc.
Acknowledgments
We thank the nursing, medical and supporting staffs of our institutions for their careful and dedicated care for the patients. We thank Dr A Voskuyl for providing the latest follow-up of one of the described patients and Mrs A I Smetsers and Mrs S Parlier for their technical support.
REFERENCES
Footnotes
-
Funding: Supported by grants from: Délégation Régionale è la Recherche Clinique (DRRC), Assistance Publique- Hôpitaux de Paris (AP-HP); the French Ministry of Health (Programme Hospitalier de Recherche Clinique: PHRC 1997 AOM 97-030); the Etablissement Français des Greffes (2003); the Groupe Français de Recherche sur la Sclérodermie (GFRS); the Association Française contre la Sclérodermie; and the Dutch Arthritis Foundation, Amsterdam, The Netherlands.
-
Competing interests: None declared
Linked Articles
- Correction