Article Text

Abstract
Background: Steroid hormone receptors such as glucocorticoid receptors, androgen receptors, and oestrogen receptors α (ERα) and β (ERβ) have been identified in synovial cells of patients with rheumatoid arthritis and osteoarthritis.
Objectives: To find a quantitative relationship between the number of receptor positive cells and markers of inflammation, and to compare the two groups of patients with rheumatoid arthritis and osteoarthritis.
Methods: A total of 36 patients with rheumatoid arthritis (n = 17) and osteoarthritis (n = 19) were included, and receptor positive cells and cellular markers of synovial inflammation were quantified by immunohistochemistry and ELISA (interleukin 6 (IL6) and IL8).
Results: Patients with rheumatoid arthritis showed a higher degree of histologically determined inflammation compared with those with osteoarthritis. However, synovial density of gluco-corticoid receptor positive (GR+), androgen receptor positive (AR+), ERα+ and ERβ+ cells were not different among patients with rheumatoid arthritis and osteoarthritis. In patients with osteoarthritis, the density of GR+ cells positively correlated with the density of AR+, ERα+ and ERβ+ cells (p = 0.007), which was not observed in patients with rheumatoid arthritis. This indicates positively coupled steroid hormone receptor expression in patients with osteoarthritis but not in those with rheumatoid arthritis. In patients with rheumatoid arthritis, secretion of synovial IL6 and IL8 positively correlated with the density of ERα+ and ERβ+ cells (not with gluco-corticoid receptor and androgen receptor), which was not found in the synovium of patients with osteoarthritis. This indicates that inflammatory factors might up regulate the expression of oestrogen receptors in patients with rheumatoid arthritis, or vice versa.
Conclusions: In patients with osteoarthritis, expression of different steroid receptors is positively coupled, which was not observed in the synovium of patients with rheumatoid arthritis. This uncoupling phenomenon in rheumatoid arthritis might lead to an imbalance of the normal synovial homeostasis.
- AR+, androgen receptor positive
- ERα+, oestrogen receptor α positive
- ERβ+, oestrogen receptor β positive
- GR+, gluco-corticoid receptor positive
Statistics from Altmetric.com
- AR+, androgen receptor positive
- ERα+, oestrogen receptor α positive
- ERβ+, oestrogen receptor β positive
- GR+, gluco-corticoid receptor positive
Steroid hormones such as glucocorticoids, androgens and oestrogens modulate the inflammatory process in patients with rheumatoid arthritis and osteoarthritis.1,2 Androgens and glucocorticoids exert anti-inflammatory effects in chronic inflammatory diseases, whereas the role of oestrogens is still a matter of debate.1,3,4 With respect to the role of oestrogens, the concentration (low, pro-inflammatory; high (as in pregnancy), anti-inflammatory) and the availability of pro-inflammatory and anti-inflammatory downstream oestrogenic metabolites may explain their heterogeneous role,5 which is currently an area of investigation. In addition, clinical studies clearly show the ameliorating effect of therapeutically administered glucocorticoids and testosterone in patients with rheumatoid arthritis.6,7,8,9,10,11,12,13
In addition, the presence of cells with steroid hormone receptors might also influence the inflammatory process. Receptors of these steroid hormones have been identified in synovial cells in patients with inflammatory joint diseases.14–18 Particularly, the macrophage type of synoviocyte, and also lymphocytes and fibroblasts, express these steroid hormone receptors.14–18 However, no data exist to date to show the relative number of steroid hormone receptor-positive cells in patients with rheumatoid arthritis and osteoarthritis. As a relative decrease in glucocorticoid receptor-positive (GR+) cells and androgen receptor-positive (AR+) cells in relation to oestrogen receptor α-positive or β-positive (ERα+ and ERβ+) cells might indicate a more pro-inflammatory situation, investigation of steroid receptor-positive cells might shed new light on this subject.
This study was initiated to investigate the presence of steroid hormone receptor-positive cells in the synovial membrane of patients with rheumatoid arthritis and osteoarthritis using a quantitative immunohistochemistry technique. This study also aimed to compare patients with rheumatoid arthritis and osteoarthritis. A further goal was to investigate the inter-relationship between the number of steroid hormone receptor-positive cells and classic markers of inflammation.
PATIENTS AND METHODS
Patients
In all, 17 patients with rheumatoid arthritis and 19 patients with osteoarthritis who underwent knee joint replacement surgery were included without further selection. Diagnosis of rheumatoid arthritis was based on the established American College of Rheumatology criteria.19 All patients were informed about the purpose of the study and gave written consent. The study was approved by the ethics committee of the University of Regensburg, Regensburg, Germany. Table 1 gives the clinical and laboratory data for the entire group included in the study. Variables such as erythrocyte sedimentation rate, C reactive protein and blood leucocyte count were measured using standard techniques.
Basic characteristics of patients with osteoarthritis and rheumatoid arthritis
Synovial tissue preparation
Synovial tissue samples were obtained immediately after opening the knee joint capsule. The preparation of the tissue for histological examination was as described.20 About 9 cm2 of synovial tissue was dissected. Fat tissue and tissue with a large number of vessels were removed. Eight synovial tissue samples were loaded into eight superfusion chambers (for technique see later) and eight approximately 1-cm2 samples of the same synovial area were used for histological examination. The samples intended for the haematoxylin–eosin staining and immunohistochemistry were fixed for 12–24 h in phosphate-buffered saline containing 4% formaldehyde and then incubated in phosphate-buffered saline with 20% sucrose for 12–24 h. Thereafter, samples were immediately placed in protective freezing medium (Tissue-Tek, Sakura Finetek Europe, Zoeterwoude, The Netherlands) and then quick-frozen floating on liquid nitrogen. All tissue samples were stored at −80°C. Samples intended for steroid hormone receptor staining were immediately embedded in paraffin wax using standard techniques (Hypercenter XP, Shandon, Frankfurt/M, Germany).
Histological evaluation of inflammation
Histological evaluation has been described in an earlier study.20 Briefly, the frozen tissue samples were cut into 6–8 μm thick sections, and cell density and lining layer thickness were evaluated using a standard haematoxylin–eosin staining of approximately 45 sections. At a magnification of 400×, the extent of the lining layer thickness was determined by averaging the number of cells in a lining layer cross section at nine different locations. The cell density in the synovial tissue was determined by counting all stained cells in 17 randomly selected high-power fields (400×) and expressed per mm2. To determine the number of T cells (CD3, Dako, Hamburg, Germany), macrophages (CD163, Dako) and capillary vessels (collagen IV, Dako) in the synovial tissue of each patient, eight cryosections were investigated using alkaline phosphatase anti-alkaline phosphatase staining, and the number of identified structures was averaged from 17 randomly selected high-power fields (400×) and expressed per mm2.
Immunohistochemistry of steroid hormone receptors
In parallel with the histological evaluation of inflammation, 5–8 μm sections from the same patient were cut from the paraffin-wax-embedded blocks. For immunostaining, the sections were deparaffinised in xylene and rehydrated in a descending ethanol series. The slides were placed in a 0.1 mol/l citrate buffer (pH 6.0) and boiled for 40 min in a water bath (90°C). Slides were then washed in TRIS buffer (pH 7.6), trypsin-digested for 20 min (37°C) and washed again in TRIS buffer. Slides were incubated for 1 h in blocking solution consisting of 10% bovine serum albumin (PAA, Pasching, Austria), 10% foetal calf serum (PAA) and 10% goat serum (Sigma, Steinheim, Germany). Slides were again washed in TRIS buffer (pH 7.6). Antibodies to gluco-corticoid receptor α (GRα) (#NCL-GCR, Novocastra, Newcastle, UK), androgen receptor (#09477, Dianova, Hamburg, Germany), ERα (#MA1-310, ABR via Dianova), and ERβ (#06-629, Upstate, Hamburg, Germany) were applied at pretested dilutions overnight at room temperature. As a negative control, sections were incubated without the primary antibody. After washing in TRIS buffer (pH 7.6), the secondary antibody for staining of growth receptor, androgen receptor and ERα (#D0486, Dako) and for staining of ERβ (#D0487, Dako) was applied for 45 min at room temperature. After washing in TRIS, these slides were incubated with BCIP (5-bromo-4-chloro-3-indoyl phosphate)/NBT (nitroblue tetrazolium) and levamisole to block the alkaline phosphatase (both from Dako). The number of steroid hormone receptor-positive cells was averaged from 17 randomly selected high-power fields (400×) and expressed per mm2. The investigators were blinded to the diagnosis and the inflammatory status.
Superfusion technique for synovial tissue and cytokine analysis in the superfusate
As described earlier,20 we used a microsuperfusion chamber apparatus to superfuse pieces of synovial tissue with culture medium (RPMI 1640, 25 mM HEPES, without foetal calf serum, 1% Pen/strep, 30 μM mercaptoethanol, 0.57 mM ascorbic acid and 1.3 mM calcium, all additions from Sigma). These superfusion chambers had a volume of approximately 80 μl. Superfusion was performed for 2 h at a temperature of 37°C and a flow rate of 66 μl/min (one sample per chamber, eight chambers in parallel). Synovial tissue samples had a standard size of 5 μm in diameter, obtained using a precision biopsy punch (Stiefel, Offenbach, Germany). After 120 min, the superfusate was collected to measure cytokine concentrations in a fraction of approximately 1 ml (collected over 15 min). Human interleukin (IL) 6 and IL8 were determined by enzyme immunometric assay (detection limit in the two assays: <2 pg/ml; Endogen via Perbio, Cologne, Germany). The interassay and intraassay coefficient of variation was <10% for both cytokines.
Presentation of the data and statistical analysis
All data are given as mean (standard error of the mean (SEM)). Correlations were calculated by Spearman’s rank correlation analysis (SPSS/PC, Advanced Statistics, V.12). Group medians were compared by the non-parametric Mann–Whitney U test (SPSS); p<0.05 was the significance level.
RESULTS
Histological inflammation in synovial tissue
Lining layer thickness and CD163 macrophage density were significantly higher in patients with rheumatoid arthritis than in those with osteoarthritis (table 2). With respect to overall cellularity, this parameter of inflammation tended to be higher in patients with rheumatoid arthritis than in those with osteoarthritis (table 2). No significant difference was observed for synovial T cell density and vascularity (table 2). All together, this indicates that patients with rheumatoid arthritis had more histological signs of inflammation compared with those with osteoarthritis.
Histological markers of inflammation of patients with osteoarthritis and rheumatoid arthritis
Density of steroid hormone receptor-positive cells in synovial tissue
Tissue density of steroid hormone receptor-positive cells was not different in patients with rheumatoid arthritis as compared with those with osteoarthritis (fig 1). Densities of ERβ+ cells and AR+ cells were higher than densities of ERα+ cells and GR+ cells; however, this direct comparison is not valid owing to the different antibodies used. As no significant difference was found between patients with rheumatoid arthritis and osteoarthritis, we compared all female patients (n = 27) with all male patients (n = 9). Mean (SEM) density of steroid hormone receptor-positive cells did not differ between female and male patients (ERα 271 (36) v 296 (58); ERβ 499 (36) v 412 (44); androgen receptor 415 (44) v 439 (49); gluco-corticoid receptor 367 (52) v 321 (94) cells/mm2).
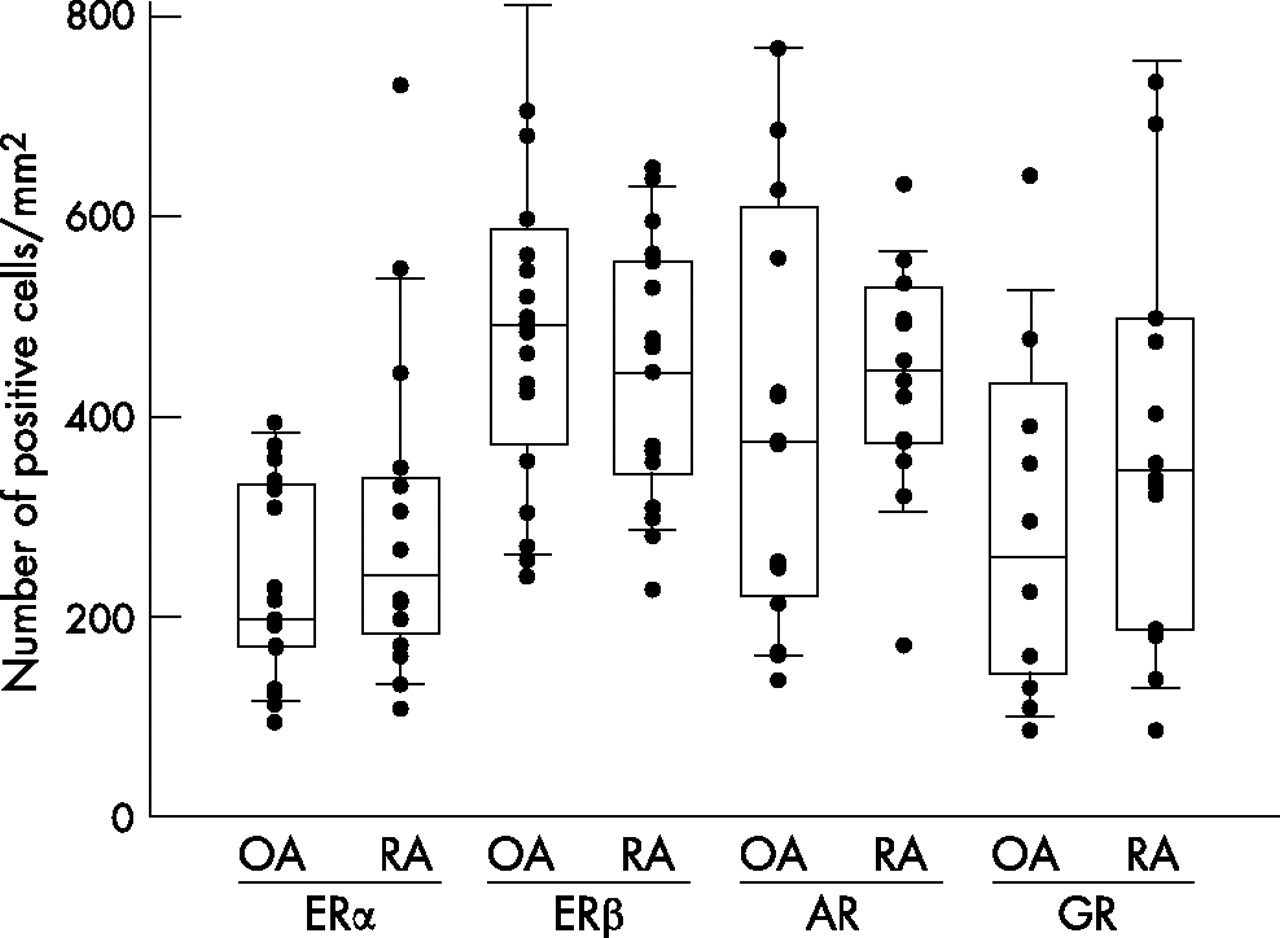
Density of steroid hormone receptor-positive cells in synovial tissue of patients with rheumatoid arthritis (RA) and osteoarthritis (OA). Individual patients are given as small black symbols. Box plots show the 10th, 25th, 50th (median within the box), 75th and 90th centiles. Owing to technical reasons, staining of receptors was not achieved in all patients. AR, androgen receptor; ERα, oestrogen receptor α; ERβ, oestrogen receptor β; GR, glucocorticoid receptor α.
A further analysis of patients with osteoarthritis showed that density of GR+ cells positively correlated with density of ERα+ cells, ERβ+ cells and AR+ cells (fig 2). This was not significant in patients with rheumatoid arthritis (fig 2). In addition, in patients with osteoarthritis, the density of AR+ cells positively correlated with density of ERα+ cells (RRank = 0.617, p = 0.014) and ERβ+ cells (RRank = 0.743, p = 0.002), which again was not significant in patients with rheumatoid arthritis (ERα: RRank = −0.258, NS; ERβ: RRank = 0.512, NS). Density of ERα+ cells and ERβ+ cells did not correlate in patients with either osteoarthritis or rheumatoid arthritis (data not shown).

Inter-relationship of density of gluco-corticoid receptor positive (GR+) cells and density of androgen receptor positive (AR+), oestrogen receptor α positive (ERα+) and oestrogen receptor β positive (ERβ+) cells in patients with rheumatoid arthritis and osteoarthritis. The panels show the linear regression line, the Spearman’s rank correlation coefficient and its p value. Due to technical reasons, staining of receptors was not achieved in all patients.
As glucocorticoids via growth receptors and androgens via androgen receptors confer anti-inflammatory effects, and oestrogen receptors, at low concentrations, confer pro-inflammatory effects, the ratios of density of steroid receptor-positive cells might better show a preponderance of an anti-inflammatory versus a pro-inflammatory pathway. However, the ratios of GR+ cells:ERα+ cells, GR+ cells:ERβ+ cells, AR+ cells:ERα+ cells and AR+ cells:ERβ+ cells did not differ between patients with osteoarthritis compared with those with rheumatoid arthritis (data not shown).
In patients with rheumatoid arthritis and osteoarthritis, the density of all steroid hormone receptors was not related to disease-specific drugs (data not shown).
Inter-relationship between density of steroid hormone receptor-positive cells and markers of inflammation
Only in patients with rheumatoid arthritis, did superfusate concentrations of IL6 and IL8 positively correlate with the density of ERα+ cells (fig 3). Similarly, only in patients with rheumatoid arthritis, did IL6 and IL8 levels positively correlate with density of ERβ+ cells (IL6: RRank = 0.700, p = 0.016; IL8: RRank = 0.627, p = 0.039). A similar positive inter-relationship did not exist for density of androgen receptor positive cells and gluco-corticoid receptor positive cells with these cytokine superfusate levels (in patients with osteoarthritis and rheumatoid arthritis; data not shown). No other histological marker of inflammation (table 2) correlated with the density of steroid hormone receptor-positive cells (data not shown).

{kind=link}
{kind=link}
{kind=link}
Inter-relationship of synovial cytokine secretion and density of ERα+ cells in patients with rheumatoid arthritis and osteoarthritis. The panels show the linear regression line, Spearman’s rank correlation coefficient and its p value. Owing to technical reasons, staining of receptors was not achieved in all patients. AR, androgen receptor; ERα, oestrogen receptor α; ERβ, oestrogen receptor β; GR, glucocorticoid receptor α.
DISCUSSION
Steroid hormone receptor-positive cells were found in different types of synovial cells in patients with rheumatoid arthritis and osteoarthritis.14–18 These receptors convey effects of steroid hormones to cells involved in the inflammatory process. Glucocorticoids and androgens are thought to exert anti-inflammatory effects in different inflammatory models and in patients with inflammatory diseases, whereas the role of oestrogens is still a matter of debate.3 Clinical studies showed the positive effect of therapeutically administered glucocorticoids and testosterone in patients with rheumatoid arthritis,6,7,8,9,10,11,12,13 and we expect that most of these effects are conveyed through intracellular gluco-corticoid receptors and androgen receptors, respectively. Glucocorticoid effects may also be partially due to binding of these steroid hormones to glucocorticoid membrane receptors.21 The effect of oestrogens seems to depend on oestrogen concentration (low, pro-inflammatory; high (similar to pregnancy), anti-inflammatory) because the dual inhibiting and stimulating roles of oestrogens have been shown in several models.22 It would be interesting to know more about receptor expression in inflamed tissue of patients with rheumatoid arthritis and osteoarthritis. To our knowledge, the relationship between the presence of receptor-positive cells and markers of inflammation has not been investigated. In addition, it is not known whether different types of steroid hormone receptors are present in synovial cells at the same time (we called this phenomenon time-coupled expression of different steroid hormone receptors).
For the first time, this study shows that the presence of one steroid hormone receptor is highly positively correlated with the presence of other steroid hormone receptors in the same tissue in patients with osteoarthritis. In patients with osteoarthritis, this phenomenon indicates common regulatory elements which coordinate expression of investigated steroid hormone receptors in a parallel fashion. We speculate that such a coupling of steroid hormone receptor expression may provide an important homeostatic effect to protect the inflamed joint. This hypothesis emerged because the coupled expression of tested steroid hormone receptors was not observed in patients with rheumatoid arthritis.
From our studies, we cannot distinguish whether this coupling appears in the same cell or in different cells. In our study, fluorescence-activated cell sorter analysis of parallel expression of intracellular receptors was not successful, and quantitative double immunohistochemistry is extremely time consuming. An explanation for the divergence in expression of steroid hormone receptors might be the different cellular composition of the synovial tissue in patients with osteoarthritis compared with those with rheumatoid arthritis. As macrophage density was higher in patients with rheumatoid arthritis than in those with osteoarthritis, and the density of T cells tended to be increased in patients with rheumatoid arthritis compared with those with osteoarthritis, the observed uncoupling phenomenon can be a readout parameter of different macrophage and T cell infiltration of synovial tissue.
Surprisingly, the density of steroid hormone receptor-positive cells did not differ between patients with osteoarthritis and rheumatoid arthritis. We recently showed that tissue levels of androgens and oestrogens were not markedly different between patients with osteoarthritis and rheumatoid arthritis,23 whereas synovial fluid levels were markedly increased in patients with rheumatoid arthritis compared with trauma controls (which are not equal to patients with osteoarthritis).5 Thus, ligand-induced down regulation of androgen receptor, ERα and ERβ might not be relevant in these patients with osteoarthritis and rheumatoid arthritis.23 It should be noted that serum hormone levels are most probably irrelevant for the local expression of steroid hormone receptors because local hormone levels are considerably higher owing to the lipophilic nature of these compounds.5 Only local concentrations of steroid hormones can provide information on whether a receptor is ligand-dependently up regulated or down regulated. The question remains as to why patients with osteoarthritis demonstrated coupling of steroid hormone receptor expression whereas those with rheumatoid arthritis did not. Pro-inflammatory cytokines, which can modulate steroid hormone receptor expression,24,25 might be responsible for the observed uncoupling phenomenon. In this respect, it is interesting that superfusate levels of IL6 and IL8 positively correlated with density of ERα+ cells and ERβ+ cells in patients with rheumatoid arthritis, which was not observed in those with osteoarthritis. As superfusate cytokine levels are closely correlated with histological inflammation,26 the more active patients with rheumatoid arthritis showed increased densities of ERα+ and ERβ+ cells. A relative increase of only ERα+ cells and ERβ+ cells, but not of AR+ cells and GR+ cells, by pro-inflammatory factors might, thus, lead to the observed uncoupling phenomenon.
Conclusion
This study shows a similar density of steroid hormone receptor-positive cells in patients with osteoarthritis and rheumatoid arthritis. However, only in osteoarthritis tissue is the presence of one steroid hormone receptor highly positively correlated with the presence of other steroid hormone receptors in the same tissue. This coupling phenomenon in patients with osteoarthritis might lead to a favourable balance in osteoarthritis tissue, the loss of which in rheumatoid arthritis tissue might prove to be an unfavourable factor to support the erosive process.
Acknowledgments
This study was supported by the Deutsche Forschungsgemeinschaft (DFG, STR 511/15–1), AN 309/2-1.
REFERENCES
Footnotes
-
Published Online First 30 June 2006
-
Competing interests: None.