Article Text

Abstract
Changes in cellular infiltrate and expression of cytokines, chemokines, and cell adhesion molecules as a result of therapeutic interventions in rheumatoid arthritis can be demonstrated in the synovial membrane. However, before synovial tissue analysis can be used as an outcome measure in such studies, standardisation of the site and method of synovial tissue acquisition, methods of tissue processing, and appropriate methods of detection and measurement of cell lineage specific markers and relevant biological proteins is needed.
- CP-J, cartilage-pannus junction
- DIA, digital image analysis
- DMARD, disease modifying antirheumatic drug
- IL, interleukin
- MC, manual counting
- MCP, metacarpophalangeal
- OA, osteoarthritis
- OMERACT, Outcome Measures in Rheumatoid Arthritis Clinical Trial
- RA, rheumatoid arthritis
- RCT, randomised controlled trial
- SM, synovial membrane
- SQA, semiquantitative analysis
- immunohistochemistry
- inflammatory arthritis
- standardisation
- synovial tissue
Statistics from Altmetric.com
- CP-J, cartilage-pannus junction
- DIA, digital image analysis
- DMARD, disease modifying antirheumatic drug
- IL, interleukin
- MC, manual counting
- MCP, metacarpophalangeal
- OA, osteoarthritis
- OMERACT, Outcome Measures in Rheumatoid Arthritis Clinical Trial
- RA, rheumatoid arthritis
- RCT, randomised controlled trial
- SM, synovial membrane
- SQA, semiquantitative analysis
Increasing interest has been shown in the use of synovial membrane (SM) tissue analysis as an outcome measure in phase Ib/phase II treatment intervention trials in rheumatoid arthritis (RA), as a “proof of concept” relating to the efficacy of new therapeutic agents.1 The advantage of using SM analysis as an outcome measure is the ability to reduce significantly the number of patients needed in studies undertaken early in the development of a new therapeutic agent when an accurate decision about whether to proceed with drug development to larger phase III and IV studies is required. Studies have already been published which have demonstrated the ability of sequentially acquired SM before and after treatment of patients with RA to reflect change in clinical disease activity.2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21 In addition, several studies have shown a lack of changes in relevant synovial biomarkers when ineffective treatment or placebo treatment is used.21–,24
However, before SM analysis can be used as an outcome measure in randomised clinical trials (RCTs), a number of factors need to be examined: (a) standardisation and validation of the methods of acquisition; (b) how representative these samples are of the generalised disease process; (c) the measurement methods used to determine a number of variables within these SM samples, including correlation with changes in clinical disease activity. This paper will examine each of these issues and also evaluate the quality of the evidence by applying the Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) filter of truth, reliability, and feasibility.25 Although most of the published studies have been performed on synovial tissue obtained from patients with RA, limited studies have looked at osteoarthritis (OA), psoriatic arthritis, and other spondyloarthropathies and these will be referred to later in this paper.
METHODS OF ACQUISITION OF SYNOVIAL MEMBRANE TISSUE
Currently, three methods of acquiring SM tissue from patients undergoing drug treatment for RA are available: blind needle biopsy, arthroscopic directed biopsy, and biopsy under imaging (usually ultrasound) guidance. The imaging techniques are relatively new and there is little published information on the reliability of this technique so it will not be discussed further in this paper. However, considerable data are available on the use of the other two techniques—the advantages and disadvantages of each will be discussed.
Blind needle biopsy has been used to sample SM for several decades and clearly has an established safety and feasibility record. It is not a costly procedure, requires no special facilities, and can be undertaken in most rheumatology departments. The main disadvantages of this technique relate to the inability to visualise directly the site of biopsy and the tissue being biopsied. In addition, it is usually only successful in acquiring synovial tissue from the knee joint and, in most cases, can only reliably sample synovial tissue from the suprapatellar bursa. There is also a concern about how often the blind needle biopsy technique may fail to obtain satisfactory SM samples, particularly if treatment results in a clinically quiescent joint, from which it is more difficult to take samples using blind needle biopsy techniques. In one series with more than 800 Parker Pearson biopsy procedures, sufficient synovial tissue for histological examination was obtained in about 85% of the patients with various forms of arthritis.26 The procedure failed especially in joints which were not swollen. Within the context of a “proof of concept” phase IB or II RCT, such a failure rate to acquire adequate synovial tissue samples would not be acceptable.
Although arthroscopic directed synovial biopsy, in comparison with the needle biopsy technique, does not have any of these potential deficiencies, it is more costly with restricted feasibility due to a requirement for skill acquisition (there is a significant “learning curve”) and the requirement for a specialised sterile area in which to undertake the procedure. Only a few studies have directly compared the two synovial membrane biopsy techniques. Two studies included SM obtained by both techniques and concluded that there is generally good correlation between the analysis of synovial tissue taken by these two techniques.27,28 However, it should be noted that these studies did not deal with the ability of the needle biopsy technique to sequentially acquire synovial tissue before and after drug treatment. In addition, the SM variables analysed were limited to macrophage and T cell surface markers, lining layer thickness, and vascularity, so it is unclear whether these results can be generalised to other SM measures of interest. Taken together, the available data indicate that blind needle techniques can be used to examine some major cell populations in cross sectional studies, but arthroscopic sampling is preferable for serial biopsy in proof of concept clinical trials.
HOW REPRESENTATIVE ARE THE SM TISSUE SAMPLES OF THE DISEASE PROCESS?
How representative SM samples are may relate to a number of factors: (a) does the SM in one joint (for example, knee, wrist, metacarpophalangeal (MCP) joint, etc) reflect that seen in other joints in inflammatory arthritis and (b) is there variability within an individual joint (for example, non-cartilage-pannus junction (non-CP-J) versus CP-J regions)? These questions have direct relevance to the source of synovial tissue for SM analysis in RCTs and whether it is reliable to restrict the number of microscopic fields analysed by SM measurement.
Only one study has been published which examined the representativeness of SM from different joints. This study compared SM from the knee joints with SM from wrist or MCP joints in patients with RA.29 The authors examined the SM tissue from nine patients who had undergone arthroscopic biopsy of an inflamed knee and small joint on the same day. Although patient numbers were small, numerous biopsy samples were analysed for markers of macrophages, T cells, and the cytokine interleukin (IL) 6, and the study suggested that there are good correlations for cell infiltration in the synovial sublining, the region where most inflammatory cells are found, between large (knee) and small (wrist or MCP) joints.
“Does the SM in one joint reflect that in other joints and does the SM vary within a single joint?”
Various studies have compared the differences in SM obtained from regions adjacent to the CP-J with SM from non-CP-J areas within the same knee joint. The first study compared biopsy specimens obtained by direct visualisation at arthroscopy and by blind needle biopsies, and therefore did not directly compare CP-J and non-CP-J tissue. The SM analysis was limited to staining for T lymphocytes and activated macrophages.28 When the arthroscopic SM biopsy specimens were used the number of macrophages was greater in the CP-J SM specimens than in non-CP-J specimens; this difference did not reach statistical significance. A second study looked at a wider range of SM variables in a larger number of patients with RA comparing CP-J with non CP-J regions and showed little difference between synovial tissue obtained from these two regions.30 A third study, with small numbers8 of patients with RA, obtained synovial tissue at the time of joint replacement surgery (four patients) or at knee arthroscopy (four patients) and concluded that macrophage infiltration was greater at the CP-J and that expression of myeloid related proteins was seen predominantly at the CP-J.31 Other studies have confirmed that there is, on average, no clear cut difference in the features of synovial inflammation or the expression of mediators of inflammation and destruction between the CP-J and non-CP-J regions.32,33
Several studies have examined the variability of SM measures within and between multiple biopsy specimens taken from within a single joint. One study analysed 154 synovial specimens from 29 patients with RA for lining layer hyperplasia, fibrosis, proliferating blood vessels, perivascular lymphocyte infiltrates, focal aggregates, and diffuse infiltrates of lymphocytes.34 The authors reported considerable homogeneity for these SM variables within a single joint. Two studies have examined the variability within and between synovial tissue biopsy specimens with interpatient variability looking at different immunohistochemical measures. One study suggested that variability within and between synovial biopsy specimens for cytokines and cell adhesion molecules was limited, and less than the variability seen in SM from different patients.35 Another study examined markers for bone erosion (RANKL and osteoprotegerin), which are very relevant to RA. This study suggested marked inter- and intra-biopsy variability for RANKL expression, probably due to the variability in T cell infiltration, whereas osteoprotegerin expression was more consistent within and between synovial biopsies.36 While this variability within SM probably accurately reflects the biological variability of expression, it does suggest that restricting the number of samples examined histologically may sacrifice reliability to improve feasibility, at least in the measurement of focally expressed SM variables.
“Restricting the number of samples may sacrifice reliability to improve feasibility”
For T cell infiltration and expression of activation antigens in RA synovium, a variance of <10% can be reached when at least six biopsy specimens are examined,37 suggesting that representative data can be obtained when a limited number of biopsy samples from different areas within one joint are investigated. Consistent with these data it has been demonstrated that using about six tissue samples allows for the detection of twofold differences in gene expression by quantitative polymerase chain reaction.38 Therefore, we recommend obtaining at least six biopsy specimens for each technique used in research.
QUANTIFICATION METHODS IN SM ANALYSIS
Three methods are commonly used in published studies to quantify immunohistochemical labelling of synovial tissues, looking at a variety of markers, including cellular infiltrate (including phenotyping of cells), cytokine and chemokine expression, receptor expression on cell surfaces, and cellular adhesion molecule expression (table 1⇓).
Application of the OMERACT filter to the three methods of measurement of synovial membrane immunohistochemical labelling currently in use
Manual counting (MC)
Manual cell counting is the time-honoured “gold standard”, although the intra- and inter-biopsy variability or responsiveness to change in disease activity of this technique has not been standardised (fig 1⇓). The results are usually recorded as the percentage of all cells counted in a high power field that are positive by immunohistochemical labelling for a particular variable, corrected for the area of tissue examined. Modifications of this technique can include restricting the region (for example, lymphocyte aggregates) or cell type (for example, T lymphocytes characterised by immunohistological staining) that is examined in each high power field. This technique is very time consuming but has face validity. It is subject to observer bias and field selection bias, unless all fields are analysed. Although it is possible to restrict the number of fields analysed by MC without affecting the reliability of the measurement, this has only been demonstrated for a limited number of SM variables.27 This technique is not well suited to, and has not been validated for, measurement of variables which are not always cell associated (for example, cytokines).

Manual counting of a synovial membrane section with a graticule.
Semiquantitative scoring (SQA)
SQA is the fastest of the quantification techniques and represents a grading of biopsy staining at low to medium power magnification (fig 2⇓). It does eliminate field selection bias but has some observer error, which may be minimised by observer training and standardisation and by using two observers, with the final score being a consensus score. Although variations of this scoring method have used single scorers, with limited training or standardisation as well as variations in scoring and averaging of high power fields, none of these variations have been validated.
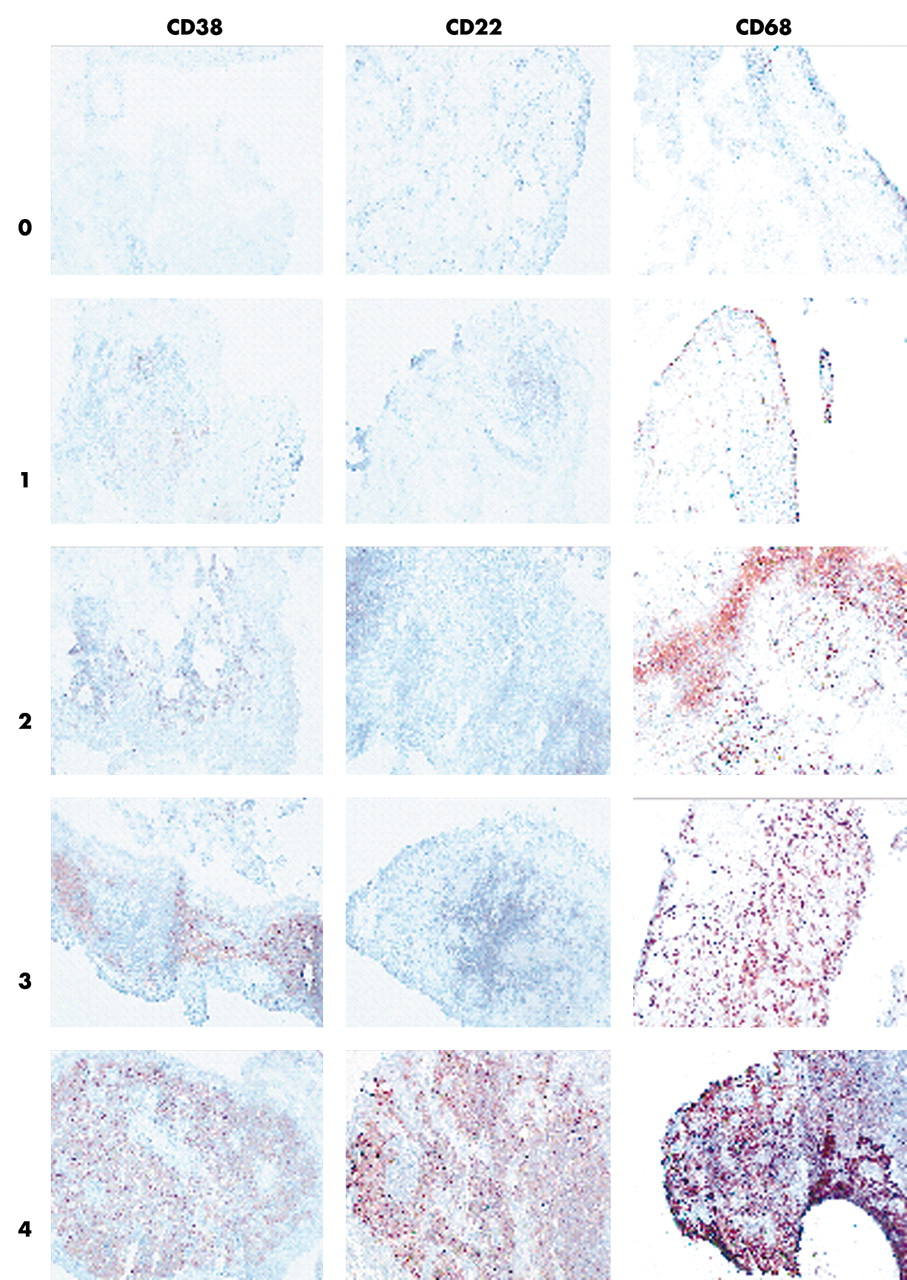
Semiquantitative scoring of synovial tissue.
Digital image analysis (DIA)
DIA is the newest of the available quantification techniques, which may be the most sensitive to change, but the equipment required is the most expensive (fig 3⇓). The results are usually expressed as the area of staining (in pixels), the density of staining (units), or as a combined measure of integrated optical density (pixel units). Several validation studies have confirmed a direct correlation between cell numbers and the area of staining as measured by DIA in various tissues. It is probably more time efficient than MC but considerable training of the observer is required. A potential for observer bias exists in the selection of thresholds and also in field selection. The former source of bias is minimised with most of the available software programs by automatic selection of the threshold when an image is scanned by the program. However, it is possible to override this automatic threshold selection process manually. Automation of the field selection using a motorised microscope stage and scanning the entire tissue section field can minimise field selection bias. As with all measurement techniques, particularly MC and DIA, the observer needs to make a decision about how intact and representative the synovial tissue being analysed is, and this can be a source of bias. This source of bias can be limited by analysing only SM samples that have an intact lining and contain sufficient subintimal tissue and by improving the quality control of SM biopsy procedures. Automation of many of the procedures can reduce the time required to use this technique, making it attractive as a quantification method for large samples.

{kind=link}
{kind=link}
{kind=link}
Digital image analysis of synovial tissue: DIA equipment (A), RA synovial tissue stained for CD3 using the immunoperoxidase method with 3-amino-9-ethylcarbazole (red) as chromogen ×200 (B) and ×400 (C). Image shown in (B) captured by DIA software and processed for nuclear staining with red mask applied (D), CD3 staining with red mask applied (E) and both nuclear staining (outlined) and CD3 staining (red mask) (F). Software will automatically detect nuclear staining and immunoperoxidase staining and calculate areas of each, but the observer can override the program if necessary.
Comparison of the quantification methods
Three studies have compared at least two of these measurement methods using the same series of synovial tissue biopsy specimens. One study used MC and SQA to measure T cell and macrophage content in sequential synovial specimens taken during treatment studies using methotrexate, IL10, and placebo.39 Both methods correlated well for lining and sublining macrophages and T cell infiltration, with a suggestion that MC was more sensitive to change in disease activity in a subgroup of nine patients with baseline and post-treatment synovial biopsy specimens.
Another study compared DIA with MC for intimal layer thickness, vascularity, CD3, and CD8 positive T cells in 78 synovial tissue sections.40 A good correlation was found between the two methods for intimal layer thickness and CD8+ cell infiltration, while the two methods correlated less well for CD3+ cell infiltration and correlated poorly for vascularity.
Another study compared DIA and SQA for the measurement of one cytokine (IL1β) and one vascular cell adhesion molecule (VCAM-1) in a series of synovial biopsy specimens from 10 patients with RA achieving an American College of Rheumatology remission with standard disease modifying agent (DMARD) treatment.41 This study showed good correlation between SQA and DIA, although when the number of high power fields assessed was reduced from 20 to 6, some increase in variability was found. This study also suggested that DIA was more sensitive to change than SQA.
Another study compared all three methods of measurement in a series of synovial biopsy specimens taken from an affected and a non-affected knee joint from nine patients with active RA.42 The variables assessed were limited to T cell (CD3+) and macrophage (CD68+) infiltrates. All three methods correlated well for both T cells and macrophages and all three methods could distinguish between the inactive and active knee SM biopsy specimens and the normal synovial tissue used as a control group in this study, although DIA and MC were more discriminatory than SQA. SQA was quicker to perform than DIA or MC, with MC being significantly slower to perform than either DIA or SQA (table 2⇓).
Comparison of the advantages/disadvantages of manual counting, semiquantitative, and digital image analysis techniques
RESPONSIVENESS OF SYNOVIAL TISSUE ANALYSIS TO TREATMENT-INDUCED CHANGES IN RA DISEASE ACTIVITY
Several studies, using a range of measurement methods, have demonstrated the responsiveness of SM analysis to changes in RA disease activity induced by treatment (table 3⇓) with conventional DMARDs2–9,14,15 or biological agents.10–13,17,18 A recent study was designed to identify the optimal synovial biomarker associated with clinical efficacy after a short treatment duration.20 This study demonstrated the status of sublining macrophages as an optimal biomarker associated with clinical response. Next this biomarker was tested across a range of discrete interventions and kinetics.21 Patients who participated in various randomised clinical trials were evaluated in the same centre, using standardised techniques. The treatments evaluated included methotrexate, leflunomide, prednisolone, infliximab, a specific CCR1 antagonist, and placebo. A significant correlation between the change in the number of sublining macrophages and the change in 28 joint count Disease Activity Score (DAS28) was found. The sensitivity to change of the biomarker was high in patients receiving active treatment, but no significant changes were detected in placebo treated patients.
Published studies on the effect of treatment on the cellular infiltrate and other biological variables in the synovial membrane
CONCLUSIONS
SM tissue acquisition is reasonably well standardised across rheumatology centres, with preference for arthroscopic directed synovial biopsy techniques. Arthroscopic biopsy is more reliable than blind needle biopsy in accessing evaluable serial synovial tissue samples as well as accessing SM from small joints other than the knee joint. It can also allow SM biopsies from all regions within a joint under direct vision. It seems that SM acquired from actively inflamed large and small joints in patients with RA is not significantly different. All three measurement methods are well validated and standardised (table 1⇑). However, methods which are both time efficient and sensitive to change in disease activity are probably more feasible, which favours DIA over SQA and MC methods of quantitative analysis. SM analysis reflects changes in RA disease activity in response to various treatments, including traditional DMARDs and biological treatments. The lack of change in SM variables in patients who fail to show a clinical response is further evidence of the reliability of SM analysis and suggests that it is an appropriate outcome measure for RCTs in RA.
Synovial tissue analysis in the spondyloarthropathies and OA
Although there have been limited studies on patients with inflammatory arthropathies other than RA, an increasing number of studies are being published looking at the synovial tissue in psoriatic arthritis44–,49 and other spondyloarthropathies.50–,55 Similar results, including the effect of standard DMARD treatment and biological treatments on the cellular infiltrate and cytokine production, are seen in these inflammatory arthropathies compared with that seen in the synovial tissue from patients with RA. Two of these studies used a modification of the SQA method45,47 that has not been validated against other measurement methods or the original SQA method, and such validation studies are required if modifications of the SQA method are to be used in future studies (see below). More recently, preliminary studies have also validated the use of synovial biopsy specimens obtained by arthroscopy for other approaches such as microarray, which proved equally sensitive to change upon treatment.52,55
Limited studies on SM analysis in OA are available, and these do not examine standardisation, which is the main focus of this paper. Although there appears to be an inflammatory component to the pathology of OA,57 it is unclear how relevant it is to the progression of the condition and at what stage in the progression of OA (preclinical, early symptoms, or late disease) SM pathology is important.58 Further studies of SM pathology in OA are clearly necessary, supported by the standardisation and validation studies which have currently been undertaken, predominantly in SM from patients with RA.
Although further studies are needed to assess specific standardisation problems, such as intra- and interjoint variability of the synovial histopathology in non-RA arthritides, these data indicate both the feasibility and the responsiveness to treatment. Because synovial histopathology reflects global disease activity in spondyloarthropathies, further exploration of synovial tissue analysis as a surrogate outcome measure in early phase clinical trials in all types of inflammatory arthritis is clearly warranted.56
FURTHER STUDIES NEEDED
Despite the fact that much work has already been done to validate and standardise SM analysis as an outcome measure, more research is required. Although not an exhaustive list, the following questions still need to be answered:
Do the published results concerning within and between biopsy variability apply to other synovial tissue variables not measured in the published studies?
Can field analysis be limited to a manageable number of high power fields without introducing excessive variability and reducing reliability and does this apply to other synovial tissue variables not measured in published studies looking at variability?
Is field selection for measures which do show regional variability (for example, T cell aggregates) appropriate or does it introduce another bias into measurement of synovial tissue analysis?
Given that there are differences between measurement methods, should more than one method of measurement be used in synovial tissue analysis and should a particular measurement method be used depending on the SM variable being measured (for example, MC for measurement of cell lineages in the inflammatory infiltrate, SQA or DIA for quantifying cytokines)?
Can modifications be made to the SQA method to restrict the number of observers and to average across measurements and does this correlate with the established method of SQA analysis?
Do all successful treatments for patients with RA produce the same effects on the synovial tissue or are some SM changes unique to specific treatments?
Are the SM changes disease-specific or can the results from RA studies be extrapolated to other inflammatory arthritides, including an asymmetric arthritis like psoriatic arthritis or a predominantly spinal condition like ankylosing spondylitis?
Most of the published studies on synovial tissue analysis have focused on cellular markers, together with protein and mRNA analysis for a limited number of proteins of interest (for example, cytokines, growth factors). With the development of more sophisticated techniques, such as microarray, laser capture of sections of interest, and new proteomic approaches, it is likely that future SM studies will use these powerful instruments to explore further the biology of synovitis.
However, before a wider application of arthroscopic synovial biopsies to clinical practice, basic research, and RCTs is possible, factors such as the availability of rheumatologists trained in arthroscopic techniques as well as the training and accreditation of rheumatological arthroscopists need to be examined. In addition, quality assurance in relation to the size of SM samples and how intact and representative these biopsies are need to be examined. These problems need to be resolved before these techniques can be widely used as surrogate outcome measures in RCTs.
REFERENCES
Footnotes
Published Online First 23 June 2005