Article Text

Abstract
OBJECTIVES To develop an enzyme linked immunosorbent assay (ELISA) using as substrate a synthetic 22-aminoacid peptide, corresponding to the ribosomal P0, P1 and P2 common epitope. To study the specificity and sensitivity of the method and evaluate the frequency and clinical associations of anti-P antibodies in two groups of systemic lupus erythematosus (SLE) patients: (a) unselected SLE patients and (b) SLE patients with central nervous system (CNS) involvement.
PATIENTS AND METHODS The C-terminal 22 aminoacid peptide of the ribosomal P proteins (Lys-Lys-Glu-Glu-Lys-Lys-Glu-Glu-Lys-Ser-Glu-Glu-Glu-Asp-Glu-Asp-Met-Gly-Phe-Gly-Leu-Phe-Asp) was synthesised according to Merrifield's solid phase procedure. Purification of the peptide was performed by preparative high performance liquid chromatography and confirmed by amino acid analysis. Using this peptide, in a concentration 5 μg/ml, an ELISA was developed. The presence of anti-P antibodies was evaluated by western blot using purified ribosomal proteins from rat liver. Sera from 178 consecutive patients with SLE and 28 patients with SLE and CNS manifestations were tested. Sera from 58 patients with rheumatoid arthritis and 57 patients with primary Sjögren's syndrome were used as controls. The cut off point of the assay was defined using 124 normal sera.
RESULTS The specificity of the assay was evaluated by homologous inhibition. Pretreatment of positive sera with soluble 22mer peptide of the ribosomal P proteins resulted in 88% inhibition. The concordance between the peptide assay and western blot was found to be 83%. Thirty three of 178 (18.6%) of the unselected SLE patients had antibodies to P-protein common epitope. Their presence was associated with more active disease (European Consensus Lupus Activity Measurement, ECLAM scoring system) (p<0.001), higher levels of anti-ds DNA antibodies (p<0.05) and lower levels of the C4 component of complement (p<0.01). Eleven of 28 (39.3%) patients with SLE and active CNS involvement had antibodies to P-protein. The overall prevalence of anti-P antibodies in active CNS disease patients was statistically significantly higher, as compared with unselected SLE patients (χ2=6.04, p<0.05). These antibodies were found in a high proportion of patients without anticardiolipin antibodies (52.4%) and they were associated with diffuse CNS involvement (psychiatric disorders (71%) and epilepsy (75%)).
CONCLUSIONS A synthetic analogue of the common epitope of ribosomal P-proteins can be use as an antigen for the detection of anti-P antibodies. These antibodies are associated with active SLE and CNS involvement particularly in patients without anticardiolipin antibodies.
- systemic lupus erythematosus
- CNS involvement
- ribosomal P proteins
- anticardiolipin antibodies
Statistics from Altmetric.com
Autoantibodies to ribosomal P proteins (anti-P antibodies) were recognised several years ago as a distinct group of autoantibodies directed against the P0, P1, and P2proteins located on the larger (60 S) subunit of the eukaryotic ribosomes.1 ,2 Sera containing anti-P antibodies react preferentially with a common epitope consisting of 22 amino acid residues and located at the carboxyl-terminal end of all P proteins.3 These autoantibodies are predominantly found in sera of patients with systemic lupus erythematosus (SLE) and have been correlated with neuropsychiatric lupus in some but not all studies (reviewed The and Isenberg4). The frequency of anti-P antibodies in SLE population is generally low and can vary from 6% to 36% in different ethnic groups.5
The aim of this study was to develop an enzyme linked immunosorbent assay (ELISA) using as substrate a synthetic 22 mer peptide, corresponding to the common epitope of P proteins and to evaluate the frequency and clinical associations of anti-P antibodies in two groups of Greek SLE patients; the first consisted of consecutive patients and the second of patients with active CNS involvement.
Methods
PATIENTS
Two groups of SLE patients were studied. All Greek patients were white. The first group consisted of 178 consecutive patients followed up in the outpatient rheumatology department. There were 173 women and five men (mean (SD) age 34.6 (6.2) years; mean (SD) disease duration 4.3 (2.1) years). Seventeen of the patients presented features of secondary antiphospholipid syndrome.6 The second group consisted of 28 patients with SLE and active CNS disease who were admitted in the hospital. There was not overlap between the two groups (mean (SD) age: 29 (8.1) years). Seven patients of the second group had anticardiolipin antibodies.7 All patients fulfilled the ACR criteria for the diagnosis of SLE.8 Active CNS involvement was considered if a patient had the following manifestations no more than two weeks before evaluation: seizures and/or cranial nerve pulse and/or stroke and/or transient ischaemic episode and/or recurrent migraine not responding to conventional treatment. Psychiatric disorder, including psychosis or organic depression were each defined according to criteria established by the American Psychiatric Association.9 This group of patients was subdivided in three subgroups, according to their clinical picture: the first group (n=11) consisted of patients with diffuse CNS disease, including patients with neuropsychiatric manifestations and/or grant mal seizures. The second group (n=13) consisted of patients with focal CNS disease. Seven patients of this group, were positive for anticardiolipin antibodies. The third group (n=4) consisted of patients with mixed form of CNS disease, presenting with transient ischaemic episodes, recurrent migraine or persistent headache.10Sera from all patients were studied for the presence of anti-dsDNA, and anti-cardiolipin antibodies by ELISA7 ,11 and for anti-Ro/SSA, anti-La/SSB, anti-U1RNP and Sm autoantibodies by counter immunoelectrophoresis.12
Sera from all patients were kept at −20°C for evaluation of anti-P antibodies. Disease activity of SLE at the time of serum collection was evaluated in each individual patient according to the European Consensus Lupus Activity Measurement (ECLAM).13
Sera from 58 patients with rheumatoid arthritis (48 women and 10 men; mean (SD) age 53.4 (6.1) years; mean (SD) disease duration 3.2 (1.1) years)14 and from 57 with primary Sjögren's syndrome15 (all women; mean (SD) age 56.4 (8.7) years; mean (SD) disease duration 6.4 (3.6) years) were used as disease controls. Sera from 10 patients with CNS disease, unrelated to SLE (four with Behçet's disease and six with multiple sclerosis) were also tested. Finally, sera from 124 normal healthy donors were used as normal controls.
PEPTIDE SYNTHESIS
The C-terminal 22-amino acid peptide of the ribosomal P protein has the following sequence: Lys-Lys-Glu-Glu-Lys-Lys-Glu-Glu-Ser-Glu-Glu-Glu-Asp-Glu-Asp-Met-Gly-Phe-Gly-Leu-Phe-Asp. This peptide was synthesised stepwise by solid-phase16using the Na -Boc-L-Asp (Bzl)- Pam resin (Boc:tertbutyloxycarbonyl, PAM:phenylacetamidomethyl). Glutamic acid was introduced as Na -Boc-L-Glu (Bzl), Lysine as Na -Boc-L-Lys (2-chloro-CBZ), while methionine was used without side protection. All protected amino acids were coupled using a ratio in mmol of amino acid /HOBT/DCC/resin 3/3/3/1 (HOBT: 1-hydroxybenzotriazole, DCC: N, N -dicyclohexylcarbodiimide). Completion of the coupling reactions was ensured by the use of the ninhydrin test. After the introduction of the Na Boc-L-Met, dimethyl sulphide was added during the removal of Boc groups to avoid oxidation of the Met side chain. The peptide was cleaved from the resin with anhydrous hydrogen fluoride in the presence of dimethyl sulphide, p-cresol and p-thiocresol as scavengers.17 The peptide was purified by preparative high performance liquid chromotography (HPLC) on a reversed phase C18 column using programmed gradient elution with the following solvents: A, H2O/. 0. 1% TFA; and B, CH3CN/o.1% TFA (TFA: trifluoroacetic acid). The purity of the peptide was confirmed by analytical HPLC and amino acid analysis.
ELISA DEVELOPMENT FOR THE DETECTION OF ANTIBODIES TO THE RIBOSOMAL P PROTEINS
We used 96 well polystyrene plates coated with different concentrations of the 22 amino acid ribosomal-P epitope ranging from 1.25 μg/ ml to 10 μg/ml in phosphate buffered saline (PBS) pH 7.3. The optimum peptide concentration of 5 μg/ml was selected as it was exhibited the highest specificity and sensitivity. Non-specific binding was eliminated using bovine serum (BS) 10% in PBS pH 7.3 (100 μl/well for two hours). Sera were tested in 1:100 dilution. This dilution was selected after several experiments with different positive controls and normal sera as it was the best discriminatory point between positive sera and normal controls. After three washes, alkaline phosphatase conjugated goat antihuman IgG antibody diluted at 1:2000 in 10% BS, PBS, pH=7.3 was added. After washing, with PBS, containing 0,1% Tween 20 and 0,01 %. NaN3, p-nitrophenylphosphate substrate was added (1 mg/ml) and the results were read within 30 minutes.
Sera were scored as positive if the optical density (OD) reading was more than the mean plus 3 standard deviations of the mean of 124 normal control sera tested. Optical density was read at 405 nm on a Dynatech (London, UK) ELISA reader.
To investigate the specificity of the method, homologous inhibition assays were performed. Briefly, several positive sera were incubated in a dilution of 1:100 with sequential concentrations of the 22-amino acid ribosomal P epitope, starting from 0.5 ng/ml to 250 μg/ml. The mixtures were kept for two hours at 37°C and overnight at 4°C. Afterwards they were tested on the ELISA plates as described above. The inhibition rate was calculated according to the equation:

PREPARATION OF RIBOSOMAL P PROTEINS AND WESTERN BLOT
To test whether anti-P antibodies reactive with the P peptide were also reacted against P proteins, an extract of ribosomes was separated by SDS-PAGE and an immunoblot was performed. An enriched fraction of ribosomal proteins were prepared from rat liver as previously described.18
Ribosomal proteins were loaded at a concentration of 5–7 μg/mm2 of gel surface on a 12.5% running gel for SDS-PAGE electrophoresis and run at constant current. Proteins were transferred onto a nitrocellulose membrane (NC). The sheet was cut for the western blot and the strips were saturated by immersion in a TRIS-HCl buffer (TBS: TRIS 0.01 M. NaCl 0.15 M pH 7.3) in which non-fat milk powder at 2% was dissolved. Serum samples were added at a 1:250 dilution in TBS and anti-human hyperoxidase conjugated IgG antibodies were used. Finally, freshly made substrate solution consisting of 3,3'-diaminobenzidine was added. Washes between steps were performed with TBS buffer pH 7.3.
STATISTICAL ANALYSIS
Statistical analysis was performed using the χ2 test with Yates's correction or Student's ttest where indicated.
Results
SPECIFICITY AND SENSITIVITY OF THE ELISA ASSAY FOR THE DETECTION OF ANTI-P ANTIBODIES
The specificity of the assay for the detection of anti-P antibodies was investigated by homologous inhibition assay. As shown in figure 1, preincubation of sera containing anti-P antibodies with soluble P peptide, inhibited the antibody binding in a dose dependent manner, reaching a maximum inhibition of 78%. Twenty sera (10 positive for anti-P antibodies by ELISA and 10 negative), were also evaluated by immunoblot. Eight of 10 sera positive by ELISA, reacted also with at least one protein in immunoblot (80%). Sera negative in ELISA, did not react on the immunoblot.

Inhibition of a serum positive for anti-ribosomal P antibodies with serial concentrations of soluble synthetic epitope analogue yielded a maximum inhibition of 78%.
PREVALENCE AND CLINICAL ASSOCIATION OF ANTI-P ANTIBODIES IN CONSECUTIVE SLE PATIENTS AND DISEASE CONTROLS
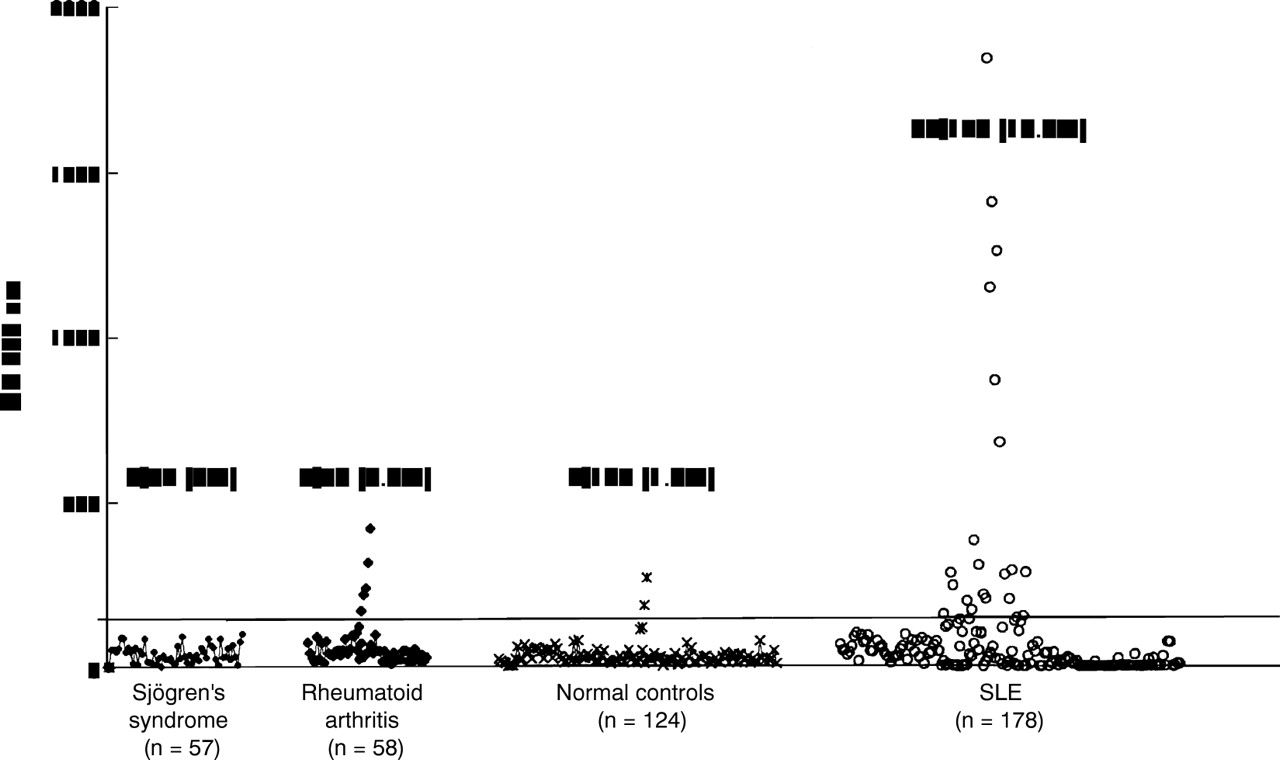
Thirty three of 178 (18.6%) consecutive patients with SLE had antibodies to ribosomal-P peptide (fig 2). Three of the patients with anti-P antibodies belonged in the group of 17 patients with secondary antiphospholipid syndrome (17.6%). Thus, 30 of 161 SLE patients (18.6%), without antiphospholipid antibodies were found to be positive for anti-P antibodies. Five of 58 (8.6%) patients with RA and two of 124 (1.6%) of normal controls had also low titres of anti-P antibodies; none of primary SS presented a positive reaction.

The prevalence of antibodies to ribosomal P synthetic epitope analogue in unselected patients with SLE, rheumatoid arthritis, primary Sjögren's syndrome and normal controls.
The presence of anti-P antibodies in patients with SLE was highly correlated with the disease activity as it was demonstrated using the ECLAM scoring system. Patients with anti-P antibodies had a mean (SD) ECLAM: score 2.9 (1.84), while patients without anti-P antibodies had a mean ECLAM: 1.45 (1.34), t=4.52 p<0.001). In addition, SLE patients with anti-ribosomal P antibodies had more commonly antibodies to dsDNA and lower levels of C4(χ2=5.53, p<0.05 and χ2= 9.38 p<0.01, respectively). Patients with anti-P antibodies had a higher prevalence of rash as compared with the remainder (χ2 = 14.25 p<0.005). CNS involvement was found in four of 35 (11.4%) of anti-P antibody positive patients and in six of 143 (4.1%) of anti-ribosomal P negative patients. Seven of these patients had past history of CNS involvement and three had active CNS disease (one was positive for anti-P antibodies and two for anticardiolipin antibodies).
PREVALENCE OF ANTI-P ANTIBODIES IN PATIENTS WITH ACTIVE CNS DISEASE
Serum was obtained from 28 SLE patients during active CNS involvement. Eleven patients had diffuse CNS involvement (seven had psychiatric disorders and four had grand mal seizures), 13 patients had focal CNS involvement, seven of whom were associated with antibodies to cardiolipin, and four patients had a mixed form of CNS disease. All sera were tested for the presence of anti-P antibodies. The overall prevalence of anti-P antibodies in active CNS lupus was 11 of 28 (39.3%). Sera from eight of 11 (72%) of patients with diffuse CNS disease (five with psychiatric disorder and three with seizures), two of 13 (15.4%) of patients with focal disease and one of four patients with mixed form presented antibodies to P protein. None of seven patients with anti-cardiolipin antibodies were found to be positive for anti-P antibodies. Thus, the frequency of the antibodies was found to be higher in lupus patients with CNS involvement without anti-cardiolipin antibodies (11 of 21, 52.4%). The prevalence of anti-P antibodies was statistically significantly higher in patients with active CNS lupus as compared with consecutive SLE patients (χ2=6.04 p<0.05). The statistically significant difference was more evident taking into consideration only patients with CNS disease without anti-cardiolipin antibodies (χ2=9.76 p<0.005) (fig 3). The titre of anti-P antibodies did not substantially differ in patients with and without CNS disease. Serum samples taken from three patients with active CNS disease after remission (two samples for each patient) in three and six months intervals did not show significant differences regarding the presence and titre of anti-P antibodies. Finally, all sera from patients with CNS involvement, unrelated to SLE, were found to be negative for anti-P antibodies.

{kind=link}
{kind=link}
{kind=link}
The prevalence of antibodies to ribosomal P synthetic epitope analogue in unselected patients with SLE, patients with SLE and active CNS involvement, and patients with antiphospholipid syndrome and CNS involvement. Patients with active CNS lupus, had more frequently anti-P antibodies as compared with unselected patients with SLE. * χ2= 6.04, p<0.05 and patients with antiphospholipid syndrome † χ2= 9.76, p<0.005.
Discussion
Autoantibodies to ribosomal P proteins are found among the systemic autoimmune rheumatic diseases, more frequently in sera of patients with SLE.4
The target antigens of anti-ribosomal P antibodies are cytoplasmic, producing a cytoplasmic/nuclear pattern, with Hep-2 staining, in the absence of other autoantibodies. Methods for the detection of these autoantibodies include western blot, where the antibodies recognise one or more of the ribosomal P proteins (P0, P1, P2) or ELISA using recombinant P-proteins as substrate.18-20 Most of the anti-P antibodies are directed against a dominant epitope that is located on the carboxyl terminal of all three proteins and consists of 22 amino acids.3 In the majority of patients the autoantibody responses are even more restricted because they are bound to the C-terminal 11 amino acids and not to other subregions of the 22-mer peptide.21 In recent years, several laboratories have developed methods for the detection of anti-ribo-P using as substrate synthetic epitope analogues corresponding to the 22-mer common epitope. These methods have been shown to present high sensitivity and specificity.18 ,22 In this study the detection of anti-P antibodies was also performed using an ELISA method based on a synthetic analogue of the 22-mer major antigenic determinant. The specificity of the method was evaluated using homologous inhibition assays and comparison of the ELISA with western blot.
In 1987, in a retrospective study by Bonfa et al,23 anti P-protein antibodies were reported to be highly specific for lupus psychosis. Since then, a number of different studies of anti-P antibodies, in regard to their association with neuropsychiatric lupus, disclosed conflicting findings. In fact, some studies supported the results of the study by Bonfaet al,5 ,22 ,24-26 but others found no association between anti-P antibodies and neuropsychiatric lupus.27-29 In this regard, the clinical part of this study was constructed to investigate the real significance of anti-P antibodies in SLE patients. Therefore, two targeted SLE populations were studied. The first consisted of 178 unselected patients evaluated prospectively and the second of 28 SLE patients with active CNS involvement evaluated retrospectively. Both groups contained patients with increased levels of anti-cardiolipin antibodies. In the first SLE population studied, the prevalence of anti-P was 19% and their presence was associated with a higher disease activity index, as it was evaluated by the ECLAM system. These findings are in agreement with previous studies by Sato et al who also described a high prevalence of anti-P antibodies in active SLE.27 However, this was not substantiated by other reports.28 In our study, patients with lupus rash, (including butterfly rash, photosensitivity, subacute cutaneous rash and discoid lesions), also presented a higher prevalence of anti-P antibodies. This positive association was reported also by Van Damet al.28 Although, SLE patients with anti-P antibodies reported in this study had higher prevalence of CNS involvement as compared with patients without anti-P antibodies, these differences were not statistically significant. Among these patients only three had active CNS involvement (two had antiphospholipid syndrome, and one psychiatric disorder) during this time period, while seven patients had a past history of CNS disease. The patient with active CNS involvement (psychosis) also had anti-P antibodies in her serum.
The discrepancies observed in different reports on the correlation of anti-P antibodies and lupus psychosis or depression have probably a multifactorial aetiology. In fact, some studies were prospective while others were retrospective (reviewed by Teh and Isenberg4). Differences in the methods and criteria used to define neuropsychiatric disease are most probably the main cause of conflicting results. In two recent reports from Japan, both authors, using the same reagents (recombinant P0 fusion protein) and the same assay, presented different results with respect to the association of anti-P antibodies with lupus psychosis.30 ,31 Another reason for the discrepant findings could be the ethnic differences in the patients studied. For example in a study by Bonfaet al,23 one third of patients who had increased anti-P antibodies were black Americans while in a study by Teh et al 29 the majority of patients were a white population. Japanese24 ,27 and Malaysian Chinese patients,32 present a higher prevalence of anti-P antibodies as compared with patients from other ethnic origin. This was further substantiated by a recent multiethnic study, where, it was found that anti-P antibodies were more frequent in Chinese patients (36%) and less common in Bulgarians (6%).5 The same study reported that the presence of anti-P antibodies in SLE patients was strongly influenced by certain MHC-II alleles. In this report the prevalence of anti-P antibodies in Greek SLE patients was 19%, which is similar with the previous study,5 where the frequency of anti-P antibodies in Greek patients with SLE was found to be 13%.
To estimate the prevalence of anti-P antibodies during active CNS disease, a second group consisting of 28 patients was studied. None of patients with anticardiolipin antibodies presented anti-P antibodies, while the proportion of anti-P antibodies in unselected SLE patients with anticardiolipin antibodies, did not differ from these without anticardiolipin antibodies. Thus, the dissociation of the autoimmune response against these two autoantigens in SLE probably suggests a different pathogenetic role of these two types of autoantibodies in CNS disease. In contrast, the majority of patients with diffuse CNS manifestations including epilepsy or psychiatric disorders had anti-P antibodies in their sera. The overall prevalence of anti-P antibodies in selected SLE patients suffering from active diffuse CNS disease was statistically significantly higher as compared with the unselected SLE population. Thus, the presence of anti-P antibodies is associated with active lupus CNS disease. Despite the fact that the origin of this autoantibody is unknown, its association with active disease and certain MHC class II alleles, suggests that its production is probably attributed to an intrinsic or extrinsic trigger on a susceptible genetic background. On the other hand serum samples taken from three patients after CNS disease remission, showed no differences in the autoantibody levels, leading to the suggestion that active disease does not influence the quantity of the autoantibody.
In conclusion, the method used for the detection of anti-P antibodies in SLE patients, using the synthetic common epitope for the detection of anti-ribosomal P proteins is reliable and easy to use for every day clinical practice. The clinical significance of the presence of anti-P antibodies in a general lupus clinic is rather limited. On the other hand, their significance in patients presenting with active CNS involvement is very useful because it can discriminate between active diffuse and focal CNS involvement of SLE. It should be stated, however, that the diagnosis of CNS lupus, is still based on clinical grounds.
Acknowledgments
The authors wish to thank Ms Pola Papadopoulou for excellent secretarial assistance.