Article Text

Abstract
Rheumatoid arthritis is associated with an increased risk for cardiovascular events, such as myocardial infarction and stroke. Epidemiological evidence suggests that classic cardiovascular risk factors, such as hypertension, dyslipidaemia, insulin resistance and body composition alterations are important but not sufficient to explain all of the excess risk. High-grade systemic inflammation and its interplay with classic risk factors may also contribute. Some associations between classic risk factors and cardiovascular risk in people with rheumatoid arthritis appear counterintuitive but may be explained on the basis of biological alterations. More research is necessary to uncover the exact mechanisms responsible for this phenomenon, develop accurate systems used to identify patients at high risk, design and assess prevention strategies specific to this population of patients.
Statistics from Altmetric.com
Increasing recognition of the excess cardiovascular (CV) risk in patients with rheumatoid arthritis (RA) has resulted in a growing body of research in this field.1,–,4 Evidence for the pivotal role of inflammation driving increased CV risk in RA is compelling. Yet, despite improved control of inflammation, CV risk among people with RA remains elevated. Consequently, the emphasis of research is shifting from characterisation of the increased CV burden in RA towards the development of effective means of reducing this excess risk. This review highlights recent advances in our understanding of CV disease in RA from an epidemiological and a biological perspective.
It is well recognised that people with RA die prematurely.5 The mortality gap between people with RA and those in the general population has been widening6 because they have not enjoyed the improvements in survival evident in the general population over the past decades. As demonstrated by a recent meta-analysis, the increased mortality risk in RA occurs largely as a result of higher rates of CV death.7 Below, we review the relative contribution of traditional and of non-traditional risk factors (markers of inflammation, RA features) towards the excess CV risk in RA, identify gaps in our understanding and suggest directions for future research.
Traditional CV risk factors and CV risk in RA
The prevalence of traditional risk factors in patients with RA compared with controls has been well described and their relative contribution to the excess CV mortality in RA is continuously being assessed.8 9 10 Epidemiological work often shows unexpected or paradoxical results and associations, some of which may be explained on the basis of biological phenomena peculiar to the RA population.
Body composition – obesity – cachexia
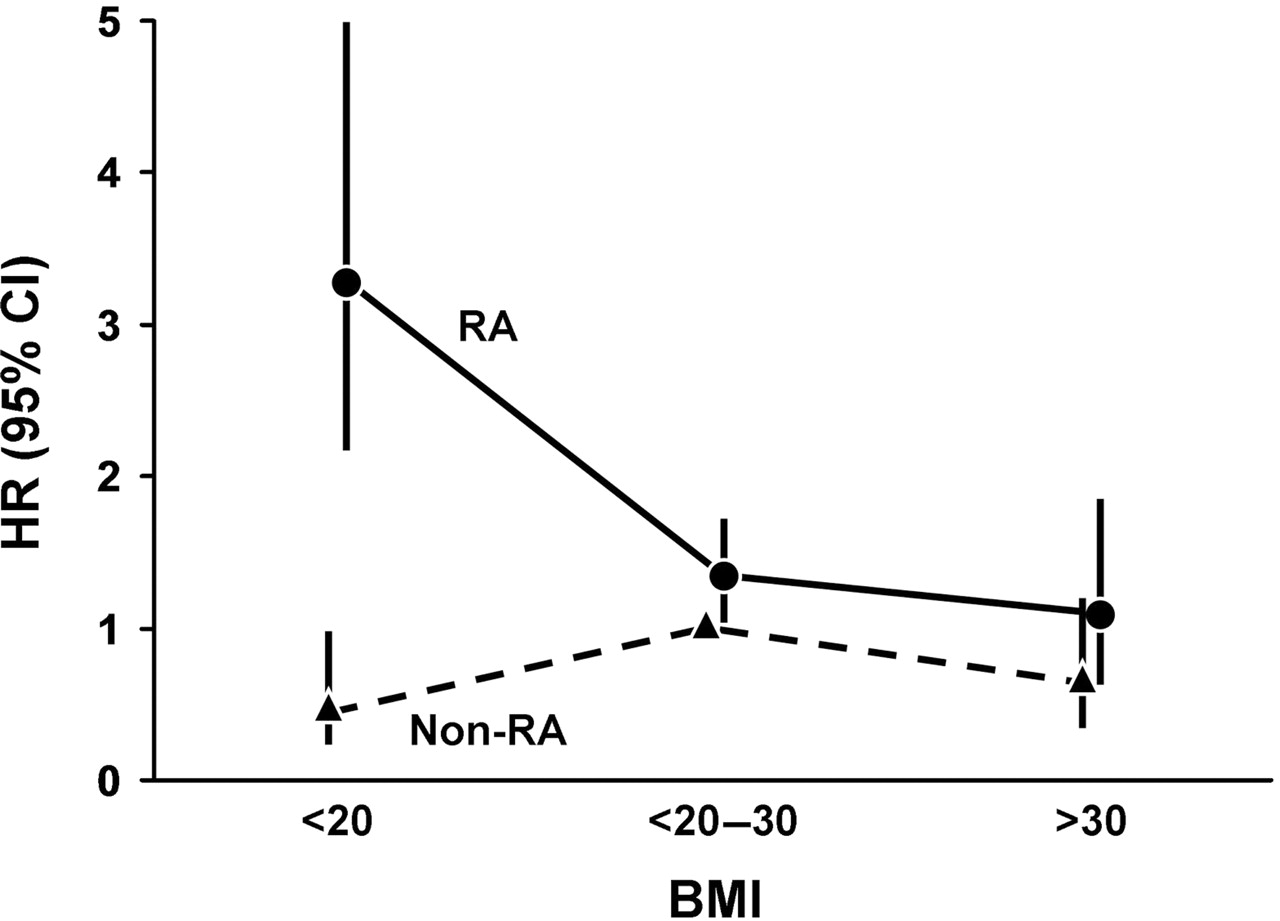
The relationship between the body mass index (BMI), overall and CV mortality in people with RA is notable. Escalante and colleagues reported a “paradoxical effect of BMI on survival in people with RA” demonstrating that as BMI declined so did survival probability among study subjects with RA.11 Among people who do not have RA, low BMI is not associated with increased risk of CV death (figure 1); if anything, low BMI may be protective for CV death. However, among patients with RA, low BMI has been shown to be associated with a threefold increased risk of CV death,12 even after adjustment for cardiac history, smoking, diabetes mellitus (DM), hypertension and malignancy. Thus, unlike the general population, low BMI in people with RA appears to be associated with a significant risk of CV death. Low BMI among people with RA may indicate uncontrolled active systemic inflammation, and this is one of many findings that lend support to the hypothesis that inflammation has a key role in the pathogenesis of CV death in people with RA.

Traditional cardiovascular risk factors in rheumatoid arthritis (RA) compared with non-RA patients—paradoxical effect of body mass index (BMI) on heart rate (HR). (Kremers HM, Nicola PJ, Crowson CS, et al. Prognostic importance of low body mass index in relation to cardiovascular mortality in rheumatoid arthritis. Arthritis Rheum 2004;50;3453. Reproduced with permission from John Wiley & Sons, Inc.)
A possible explanation of the paradoxical association between BMI and CV outcomes in this population is that RA appears to be associated with profound alterations in body composition, which are not reflected in the BMI thresholds used in the general population.13 Activation of the NF-κB pathway triggers muscle degradation (cachexia), while an inactive lifestyle may contribute to accumulation of fat,14 resulting in stable or slightly increased body weight. There appear to be two states of cachexia in RA: rheumatoid cachexia (characterised by low muscle mass and high fat mass), and classic, low BMI cachexia (low muscle and low fat mass). The latter is now relatively rare in RA, associated with severe, uncontrolled systemic inflammation and much worse arthritis and CV outcomes. In contrast, rheumatoid cachexia is more prevalent and may represent, from the CV perspective, the ‘worst of both worlds’, having features of classic cachexia (low muscle) and of obesity (high fat); however, data remain inconclusive, partly owing to the lack of a clear, agreed definition for it15 (figure 2). Obesity is associated with the presence of traditional CV risk factors in patients with RA,16 as it is in the general population. In particular, abdominal fat is associated with insulin resistance, cardiometabolic risk and inflammatory load in patients with RA17 and there is new evidence that in such patients, abdominal fat is distributed differently between the visceral and subcutaneous compartments, with visceral fat more strongly associated with cardiometabolic risk.18 Adipose tissue is metabolically active and through a network of adipocytokines regulates energy intake and expenditure and also inflammation. Research on adiposity in RA remains in its infancy but is obviously important from both, the rheumatological and the CV perspectives.19 Similarly, interventions to reverse rheumatoid cachexia, control obesity and regulate insulin resistance in RA have been little studied: the effects of pharmacological interventions with anti-tumour necrosis factor α (TNFα)20 and other biological agents, structured exercise and diet require further evaluation.15 19 21
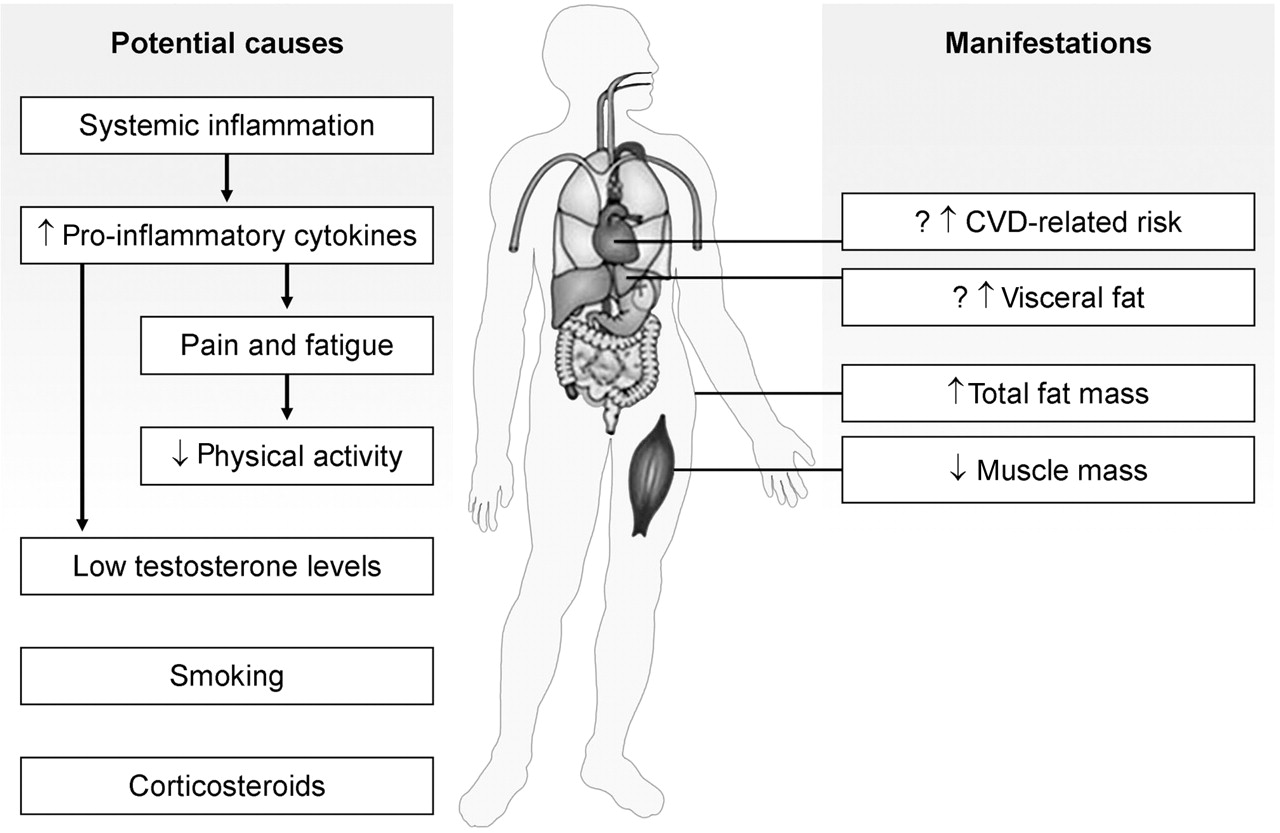
Causes and manifestations of rheumatoid cachexia. CVD, cardiovascular disease. (Summers GD, Metsios GS, Stavropoulos-Kalinoglou A, et al. Medscape. Rheumatoid cachexia and cardiovascular disease. Nat Rev Rheumatol 2010;6:445–51. Reproduced with permission from Nature Publishing Group.)
Lipids
Hyperlipidaemia (high total or low-density lipoprotein (LDL) cholesterol) appears to be less common in RA than in non-RA subjects8 10 but dyslipidaemia (alterations of individual lipid components and their ratios as defined by specific criteria) may affect up to half of all patients with RA in hospital care.22 Although findings have been somewhat inconsistent, like BMI, lipids also appear to have a paradoxical effect on CV risk in people with RA10 22,–,26—for example, decreased lipid levels are associated with increased CV risk. Serum levels of total cholesterol and LDL cholesterol decline precipitously during the 3–5-year period before RA incidence,27 and lower total and LDL cholesterol levels have been shown to be associated with higher CV risk28 (figure 3).

Changes in low-density lipoprotein (LDL) and total cholesterol (Tch) from 5 years before the rheumatoid arthritis (RA) incidence/index date until 5 years after the RA incidence/index date among RA and non-RA subjects. (Gabriel SE. Heart disease and rheumatoid arthritis: understanding the risks. Ann Rheum Dis 2010;69(Suppl 1):i61–4. Reproduced with permission from BMJ Publishing Group Ltd.)
Alterations of the lipid profile have been extensively reported in RA: suppression of total and LDL cholesterol levels during acute or chronic high-grade inflammation is well described, as is also a proportionately greater suppression of high-density lipoprotein (HDL), giving a disadvantageous atherogenic index. However, in vitro animal model and human in vivo studies in subjects without RA clearly demonstrate that the interplay between inflammation and lipid components is far more complex than just alterations of their serum levels (reviewed by Toms et al29) (figure 4). For example, acute phase proteins, such as serum amyloid A and phospholipase A2 can alter HDL composition and function, while inflammation may have profound effects on enzymes fundamental to the metabolism of HDL (eg, hepatic lipase) or indeed the enzymatic content of HDL itself (eg, reduced paraoxonase); this may increase susceptibility to oxidation and convert HDL to a more pro-oxidant, pro-atherogenic complex. Such inflammation-induced alterations of structure and function are not confined to HDL but involve also triglycerides and LDL; they require further study, specifically in people with RA and in the context of disease control with non-biological and biological disease-modifying antirheumatic drugs. To date, several studies suggest that antirheumatic treatments, including glucocorticoids, hydroxychloroquine, gold, ciclosporin, as well as the biological agents anti-TNFα, rituximab and tocilizumab, affect lipid levels: these are generally short-term studies of small numbers of patients dealing predominantly with serum levels rather than other modifications or mechanisms.20 30 Multiple other factors are involved in lipid regulation and function, including physical activity, adiposity, diet, alcohol intake and smoking: their effects have not been assessed in any detail in people with RA. Similarly, the importance of genetic regulation of lipid metabolism, particularly in the context of gene–environment interactions, has not been examined in the RA population. This may be particularly important, since lipid alterations appear to predate the diagnosis of RA.

The effects of inflammation on lipid structure and function. (Toms TE, Symmons DP, Kitas GD. Dyslipidaemia in rheumatoid arthritis: the role of inflammation, drugs, lifestyle and genetic factors. CETP, cholesterylester transfer protein; HDL, high-density lipoprotein; HL, hepatic lipase; LCAT, lecithin-cholesterol acyltransferase; LDL, low-density lipoprotein; LPL, lipoprotein lipase; PAF-AH, platelet activating factor-acetylhydrolase; SAA, serum amyloid A; sPLA2, serum phospholipase A2; PLTP, phospholipid transfer protein; VLDL, very-low-density lipoprotein. Curr Vasc Pharmacol 2010;8:301–26. Reproduced with permission from Bentham Science Publishers Ltd.)
Statins are well established in the primary prevention of CV events in the general population and at-risk subpopulations (eg, patients with DM) and may have additional anti-inflammatory effects useful for patients with RA.31 Despite that, they are underused for primary prevention in patients with RA, even in those who have a high risk according to general population risk algorithms.22 This may be owing to a lack of systematic screening for CV risk, confusion of rheumatologists and general practitioners, and concerns about the efficacy and safety of such treatment in this patient population. A recent meta-analysis of 26 randomised controlled trials (RCTs) of statins suggests that each 1 mmol/l reduction in LDL cholesterol reduces the risk of heart attacks, revascularisations and strokes by about 20%. Such impressive results do not negate the need for trials in specific patient subpopulations, including RA, as some recent statin RCTs in other high-risk populations with renal failure and chronic heart failure have not shown clear evidence of benefit. It has been suggested that the results of the JUPITER trial could be used to justify widespread usage of statins for primary prevention in patients with RA.32 Patients with RA, however, were completely excluded from JUPITER. They usually have C-reactive protein (CRP) levels massively in excess of the arbitrarily chosen threshold of 2 mg/l used in that trial, as well as a significant classical CV risk factor load, unlike the participants in JUPITER, who had no other risk factors. For these reasons, including the epidemiological data showing the paradoxical inverse association of lipid levels and CV risk in patients with RA, a hard end-point statin trial specifically in this population is imperative. Such a trial (TRACE RA; http://www.dgoh.nhs.uk/tracera/) requiring almost 4000 patients with RA has started in the UK, has already recruited over 2250 patients but is not likely to report before 2016.
Hypertension
Hypertension is common in patients with RA but it remains unclear whether it is more common than in a comparable general population of subjects without RA.33 There is evidence, however, for underdiagnosis and undertreatment of hypertension in patients with RA,34 despite the fact that it is the major determinant of target organ damage in these patients.35 A link between low-grade inflammation and hypertension has been suggested from general population studies. High CRP can reduce endothelial nitric oxide, leading to vasoconstriction, increased endothelin-1, platelet adherence, oxidation and thrombosis; it can also upregulate angiotensin type 1 receptor expression and thus influence the rennin–angiotensin system33 (figure 5). The relationship between the high-grade systemic inflammation of RA and blood pressure has not been investigated in detail. A cross-sectional study did not demonstrate significant differences in RA disease activity between hypertensive and normotensive patients with RA34 but in the same population, long-term corticosteroid use was a significant independent predictor of hypertension,36 raising the possibility of channelling bias. A recent post hoc analysis of the BeST trial suggested that effective control of RA disease activity is associated with blood pressure reduction,37 and some work from our group suggests that this may be through reductions in arterial stiffness. Multiple other factors may influence blood pressure control in people with RA, including physical inactivity, obesity, specific genetic polymorphisms and several antirheumatic drugs. Their relative contribution requires further investigation, as it may lead to the development of effective intervention strategies, which need to be specifically evaluated in this population.

The interaction between systemic inflammation and hypertension in patients with rheumatoid arthritis. CRP, C-reactive protein; IL, interleukin; INFγ, interferon γ; RA, rheumatoid arthritis; TNF, tumour necrosis factor; VCAM1, vascular cell adhesion molecule-1. (Panoulas VF, Metsios GS, Pace AV, et al. Hypertension in rheumatoid arthritis. Rheumatology (Oxford) 2008;47:1286–98. Reproduced with permission from Oxford University Press.)
Impact of traditional CV risk factors in patients with RA
The relative impact of traditional CV risk factors, including male gender, current smoking, personal and family history of ischaemic heart disease, hypertension, hyperlipidaemia, BMI >30 kg/m2 and DM, appears to be less in RA than in non-RA subjects (figure 6), while some risk factors show paradoxical associations. Clearly, much more research is needed to better understand the mechanisms underlying these relationships. While the reasons remain unclear, we posit the existence of a complementary mechanism, perhaps related to chronic ‘high-grade’ systemic inflammation, which imparts additional CV risk in RA but not in non-RA subjects. This could result in an apparent dilution effect, making the relative contribution of each individual mechanism or risk factor appear smaller, and may have a significant adverse effect on the ability of risk algorithms developed for the general population to accurately assess future CV risk in patients with RA.

Relative impact of traditional cardiovascular (CV) risk factors on combined CV end point in patients with rheumatoid arthritis (RA) and non-RA subjects. BMI, body mass index. (Gabriel SE. Heart disease and rheumatoid arthritis: understanding the risks. Ann Rheum Dis 2010;69(Suppl 1):i61–4. Reproduced with permission from BMJ Publishing Group Ltd.)
Maradit Kremers et al38 reported the 10-year absolute CV risk in people with RA and demonstrated that while relative risk information is useful, estimating absolute risk by age group is more clinically meaningful. In this analysis, a high 10-year absolute CV risk was seen at RA onset across the four age groups from 40 through 80 years of age. The absolute CV risk in RA subjects was equivalent to that in non-RA subjects who were 5–10 years older. Further studies suggest that CV disease and CV death in RA are of similar magnitude to that seen in patients with type 2 DM39 (figure 7). This information, together with the findings that traditional CV risk factors behave differently in subjects with RA, suggest that risk scores based on traditional CV risk factors alone are likely to underestimate CV risk in RA. Indeed, recent studies have reported that such risk scores (eg, Framingham) can underestimate CV risk fivefold in some patients with RA.40 Interestingly, research has also shown that these scores underestimate CV risk in other chronic diseases such as chronic kidney disease and diabetes.41,–,44 All this clearly highlights the need for RA-specific risk prediction tools. To this end, the European League Against Rheumatism has recently proposed the application of a ×1.5 multiplier to the risk calculated on the basis of standard algorithms.45 This approach, while appealing in its simplicity, requires long-term validation.

Cardiovascular event-free probability to 3 years among non-diabetic controls (black line), patients with type 2 diabetes mellitus (DM) (light grey line) and non-diabetic patients with rheumatoid arthritis (RA) (dashed line). The hazard ratios for the non-diabetic controls and patients with RA as compared with non-diabetic controls were as follows: for patients with type 2 DM, 2.0 (95% CI 1.1 to 3.7); for non-diabetic patients with RA, 2.2 (95% CI 1.3 to 3.6). Differences were estimated from age- and sex-adjusted Cox proportional hazards models. (Peters MJ, van Halm VP, Voskuyl AE, et al. Does rheumatoid arthritis equal diabetes mellitus as an independent risk factor for cardiovascular disease? A prospective study. Arthritis Rheum 2009;61:1571–9. Reproduced with permission from John Wiley & Sons, Inc.)
Whereas our understanding of the exact role of traditional CV risk factors in RA needs to be improved and the potential beneficial impact of interventions for their control need to be evaluated specifically in this population, a lot is already known that can be applied in the clinical setting, using common sense. Traditional CV risk factors can be easily identified in individual patients with appropriate screening and monitoring strategies; they are obvious targets for intervention aiming to achieve at least thresholds applied to the general population while waiting for more information; and their control is likely to have a beneficial effect on CV outcomes. In this modern era, disease-specific CV risk assessment tools need to be developed and become fully embedded in the routine care of the patient with RA.
Inflammation and CV risk in RA
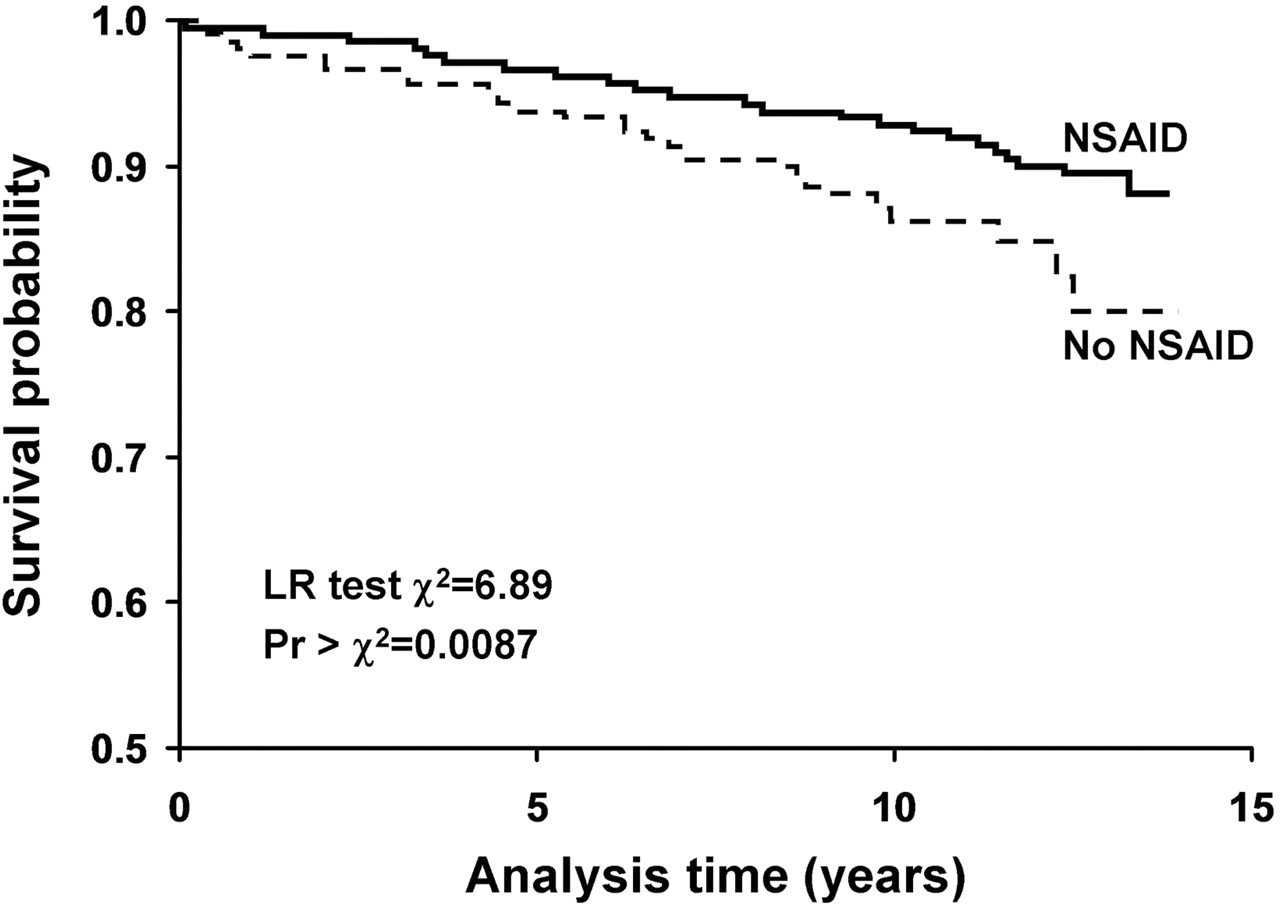
The independent contribution of inflammatory indicators and RA characteristics towards risk of CV death has been studied. High erythrocyte sedimentation rate (ESR), rheumatoid factor, anticyclic citrullinated peptide antibodies, other inflammatory mediators, RA activity and severity—that is, small and large joint swelling, destructive changes on joint radiographs, rheumatoid nodules, vasculitis, rheumatoid lung disease and corticosteroid use are statistically significantly associated with increased risk of CV events and/or death.38 46,–,52 One study examined ESR as a CV risk factor in RA. Analyses of ESR levels in 172 patients with RA and heart failure demonstrated that the proportion with significantly elevated ESR (≥40 mm Hg) was higher during the 6-month period before heart failure diagnosis than at any other time over the entire follow-up period.19 Other studies have demonstrated a significantly increased risk of myocardial infarction, heart failure and/or vascular disease as well as overall mortality in subjects testing positive for rheumatoid factor, even after adjusting for the presence of rheumatoid disease.47 50 The same relationships have also been observed for antinuclear antibody-positive subjects,47 53 suggesting that immune dysregulation may promote CV risk in people with rheumatic disease and also in the general population47 and further supporting the hypothesis that inflammation and immune dysregulation are responsible, at least in part, for the excess CV risk in RA. Drugs may also affect CV outcomes in RA. Because of the almost universal use of non-steroidal anti-inflammatory drugs (NSAIDs) and concerns surrounding CV risk with their use, this has been extensively studied. Strong recent evidence indicates that NSAID use54 is not associated with increased CV risk in RA (figure 8). In contrast, use of disease-modifying antirheumatic drugs (methotrexate in particular) and/or biological agents, has been suggested to decrease CV risk55,–,58 and this is again thought to be due to effective long-term control of systemic inflammation. While these findings are intriguing, they cannot be considered definitive evidence that these agents reduce CV risk, owing to confounding by indication/contra-indication.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiovascular mortality: Kaplan–Meier survival estimates, by ever use of non-steroidal anti-inflammatory drug (NSAID). LR, likelihood ratio. (Goodson NJ, Brookhart AM, Symmons DP, et al. Non-steroidal anti-inflammatory drug use does not appear to be associated with increased cardiovascular mortality in patients with inflammatory polyarthritis: results from a primary care based inception cohort of patients. Ann Rheum Dis 2009;68:367–72. Reproduced with permission from BMJ Publishing Group Ltd.)
Inflammation and ‘accelerated’ atherosclerosis in RA
The thesis that ‘high-grade’ systemic inflammation has a central position in driving the increased CV risk in RA is supported by evidence that ‘low-grade’ inflammation, as reflected usually by high-sensitivity CRP and several other indicators of the acute phase response, is also associated with higher risk and worse CV outcomes in the general population.59 The biological basis of this began to become evident in the early 1990s, with the then emerging, but now compelling, evidence that atherosclerosis has a chronic inflammatory aetiopathogenesis.60 The cell types, cytokine signalling, adhesion interactions and tissue-damaging processes involved in the generation, progression, instability and rupture of atheromatous plaques are reminiscent of those seen in chronic rheumatoid synovitis.61 The suggestion was therefore made over 15 years ago, that ‘high-grade’ systemic inflammation in RA may be related to generalised vascular injury, enhanced CV morbidity and mortality.62 This could be through direct effects of inflammation on the endothelium but also through a complex interplay between inflammation, traditional CV risk factors and the vasculature.63
Despite much work in the intervening years, the concept of accelerated atherosclerosis in RA has still not been proved. Most of the evidence is indirect and comes from studies employing non-invasive assessments of vascular function or morphology in people with RA compared with controls. Such functional and/or morphological changes reflect early, preclinical stages of atherosclerosis and some have been associated with long-term CV outcomes in the general population. Only one study has suggested that this may be the case in RA.64 The majority of studies performed to-date are cross-sectional, with few, short-term, longitudinal studies and a handful of RCTs of anti-TNFα biological agents; they are as a rule underpowered, of varying quality and in most cases have not dealt with important confounders. Although they collectively demonstrate worse vascular function and morphology in RA than in controls, these studies have not provided definitive answers as to whether this relates to mechanisms operating before or since the onset of RA, or the relative contribution of current versus cumulative inflammation versus traditional CV risk factors and their interplay.
Effective RA treatment appears to be associated with some, often transient, improvements in vascular function but there are no clear, consistent relationships between this and contemporary disease activity. In agreement with epidemiological data,39 the frequency and severity of functional and morphological vascular abnormalities appear to be similar between patients with RA and those with diabetes of similar duration, despite a worse traditional CV risk profile of diabetics, suggesting a significant additional risk conferred by RA-related factors.65 These may of course include inflammation but also other important factors such as physical inactivity, genetic susceptibility or antirheumatic treatment. Interestingly, analysis of autopsy specimens has shown more features of advanced plaque instability rather than more advanced atherosclerotic disease in people with RA compared with matched non-RA subjects.66 This agrees with clinical observational studies showing a worse outcome and higher reinfarction rates after acute coronary syndromes in patients with RA compared with controls.67 It is therefore possible, and entirely compatible with the epidemiological data, that high-grade systemic inflammation in RA does not necessarily imply accelerated atherosclerosis but rather an increased propensity to plaque instability and rupture. This could explain some of the epidemiological paradox as to the contribution of classical CV risk factors to CV outcomes in RA. Classical CV risk factors, rather than high-grade inflammation, may be as important in RA as in the general population for the generation and progression of stable atherosclerotic disease, whereas local and systemic high-grade inflammation may contribute more specifically to plaque instability and therefore higher rates of, and worse outcomes from, acute coronary syndromes and strokes.
Non-invasive assessments of vascular function and morphology, including the use of more recent imaging modalities, such as coronary CT angiography, MR coronary angiography and positron emission tomography among others, remain a very important area of future inquiry, particularly if linked to biomarker research. They provide good human in vivo systems to investigate specific mechanisms involved in vascular pathophysiology and the short-term effects of different treatments. If proved to be good surrogates of future CV events in people with RA, they could be used as primary end points for RCTs of treatments targeting either inflammation or traditional CV risk factors in people with RA in order to establish best primary and secondary prevention strategies. This is particularly pertinent, in view of the very high numbers and length of follow-up required for trials based on hard CV end points.
Summary and conclusions
CV disease remains a major problem for people with RA. Systemic inflammation and its interplay with traditional CV risk factors appears to have a major role, through direct and indirect effects on the vasculature. Future work should focus on further delineating the exact mechanisms involved, develop and evaluate risk assessment tools and biomarkers, as well as prevention and treatment strategies specific to the RA population. Effective, even optimal control of traditional risk factors is imperative but may be insufficient to reduce CV risk for people with RA; tight control of systemic inflammation is likely to be required for optimal results. These approaches should be evaluated in the long term, including in large, hard endpoint trials. In addition to pharmacological interventions, patient and health professional education,68 and adoption of lifestyle changes, particularly physical activity, should also be considered and evaluated in order to reduce CV risk in RA.
References
Footnotes
-
Funding Arthritis Research, UK, the British Heart Foundation, the Medical Research Council and the National Institutes of Health, National Institute of Arthritis and Musculoskeletal Diseases.
-
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous