Article Text

Abstract
Introduction Vaccination represents a cornerstone in mastering the COVID-19 pandemic. Data on immunogenicity and safety of messenger RNA (mRNA) vaccines in patients with autoimmune inflammatory rheumatic diseases (AIIRD) are limited.
Methods A multicentre observational study evaluated the immunogenicity and safety of the two-dose regimen BNT162b2 mRNA vaccine in adult patients with AIIRD (n=686) compared with the general population (n=121). Serum IgG antibody levels against SARS-CoV-2 spike S1/S2 proteins were measured 2–6 weeks after the second vaccine dose. Seropositivity was defined as IgG ≥15 binding antibody units (BAU)/mL. Vaccination efficacy, safety, and disease activity were assessed within 6 weeks after the second vaccine dose.
Results Following vaccination, the seropositivity rate and S1/S2 IgG levels were significantly lower among patients with AIIRD versus controls (86% (n=590) vs 100%, p<0.0001 and 132.9±91.7 vs 218.6±82.06 BAU/mL, p<0.0001, respectively). Risk factors for reduced immunogenicity included older age and treatment with glucocorticoids, rituximab, mycophenolate mofetil (MMF), and abatacept. Rituximab was the main cause of a seronegative response (39% seropositivity). There were no postvaccination symptomatic cases of COVID-19 among patients with AIIRD and one mild case in the control group. Major adverse events in patients with AIIRD included death (n=2) several weeks after the second vaccine dose, non-disseminated herpes zoster (n=6), uveitis (n=2), and pericarditis (n=1). Postvaccination disease activity remained stable in the majority of patients.
Conclusion mRNA BNTb262 vaccine was immunogenic in the majority of patients with AIIRD, with an acceptable safety profile. Treatment with glucocorticoids, rituximab, MMF, and abatacept was associated with a significantly reduced BNT162b2-induced immunogenicity.
- Covid-19
- methotrexate
- vaccination
- biological therapy
- rituximab
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data used to support the findings of this study are included within the article.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
Data on efficacy and safety of the SARS-CoV-2 BNT162b2 messenger RNA (mRNA) vaccine in patients with autoimmune inflammatory rheumatic diseases (AIIRD) are limited.
What does this study add?
This is the largest observational prospective study conducted to confirm immunogenicity of the BNT162b2 mRNA vaccine in the majority of patients with AIIRD compared with controls.
Immunogenicity was severely impaired by rituximab; moderately impaired by glucocorticoids, abatacept, and mycophenolate mofetil; and mildly impaired by methotrexate.
The vaccine was generally safe in terms of adverse events.
Postvaccination disease activity remained stable in the majority of patients with AIIRD.
How might this impact on clinical practice or future developments?
Most disease-modifying antirheumatic drugs, including methotrexate, anticytokine biologics and Janus kinase inhibitors, can be continued with relation to the administration of the BNT162b2 mRNA vaccine.
Postponing treatment with rituximab, when feasible, should be considered to improve immunogenicity. Holding treatment with mycophenolate mofetil and abatacept, especially when combined with methotrexate, may be considered on an individual basis.
Introduction
The prevention of COVID-19 pandemic has become of paramount importance. BNT162b2, a messenger RNA (mRNA)-based vaccine, has demonstrated a high efficacy rate with an acceptable safety profile.1 2 A mass BNT162b2 vaccination campaign has been launched in Israel, with high uptake of vaccination in about 55.5% of the country’s population. Patients with autoimmune inflammatory rheumatic diseases (AIIRD) have been prioritised for urgent vaccination to mitigate COVID-19 risk, consistent with the American College of Rheumatology (ACR) guidelines,3 despite a paucity of data on the efficacy and safety of mRNA COVID-19 vaccines in this population. Recently, some encouraging data on mRNA vaccination in immunosuppressed patients have emerged based on two small studies with a limited follow-up.4–6 Therefore, we conducted a large prospective observational multicentre study to evaluate immunogenicity, efficacy, and safety of the BNT162b2 mRNA vaccine in patients with AIIRD compared with control subjects without rheumatic diseases or immunosuppressive therapies.
Methods
This prospective observational exploratory multicentre study was conducted at the Rheumatology Departments of Tel Aviv Sourasky, Carmel, and Hadassah Medical Center, Israel, between December 2020 and March 2021.
End points of the study
The primary end point was immunogenicity of the BNT162b2 mRNA vaccine in adult patients with AIIRD compared with controls measured 2–6 weeks after the second vaccine dose.
Secondary end points included
Effect of immunosuppressive treatments on vaccine’s immunogenicity.
Efficacy of vaccination, defined as prevention of COVID-19 disease, confirmed by a PCR testing.
Safety of vaccination in patients with AIIRD compared with controls.
Effect of vaccination on clinical disease activity in patients with AIIRD.
Study population
Consecutive adult patients (aged ≥18 years) were recruited into the study according to the following inclusion criteria: rheumatoid arthritis (RA)/ACR/European League Against Rheumatism (EULAR) 2010 classification criteria7; psoriatic arthritis (PsA)/Classification Criteria for PsA8; axial spondyloarthritis (axSpA)/Assessment of SpondyloArthritis International Society classification criteria9; systemic lupus erythematosus (SLE)/1997 ACR10 or 2012 Systemic Lupus Erythematosus International Collaborating Clinics criteria11; systemic vasculitis: large vessel vasculitis (LVV), antineutrophil cytoplasmic antibody-associated vasculitis (AAV), including granulomatosis with polyangiitis (GPA), microscopic polyangiitis and eosinophilic GPA/Chapel Hill Consensus Conference definitions12; central nervous system (CNS) vasculitis, including primary CNS vasculitis, neuro-Behcet and Susac syndrome; and idiopathic inflammatory myositis (IIM)/EULAR/ACR classification criteria.13
Patients were instructed to continue all medications during the vaccination period, except for rituximab treatment that was delayed after the vaccination in certain cases on a physician’s discretion.
The control group included a sample of the general population, consisting mainly of healthcare personnel. Exclusion criteria for all groups were pregnancy, history of past vaccination allergy, and previous COVID-19 infection and for controls—history of AIIRD and immunosuppressive treatment.
Vaccination procedure
All study participants were administered the two-dose regimen BNT162b2 mRNA vaccine (Pfizer-BioNTech), 30 µg per dose, by intramuscular injection in the deltoid muscle 3 weeks apart, as indicated by the national guidelines.
Immunogenicity of the vaccine
The vaccine immunogenicity was evaluated by measuring the serum IgG neutralising antibody levels against SARS-CoV-2 trimeric spike S1/S2 glycoproteins, using the LIAISON (DiaSorin) quantitative assay, performed 2–6 weeks after the second vaccine dose. This Food and Drug Administration-authorised assay has a clinical sensitivity and specificity above 98%.14 A value above 15 binding antibody units (BAU) was considered as positive, according to the manufacturer’s instruction.
Efficacy of the vaccine
The participants were questioned whether they contracted COVID-19 infection, confirmed by PCR, following each vaccine dose. In addition, up to the data cut-off, the patient files were reviewed for evidence of COVID-19 infection.
Safety of the vaccine
The participants were contacted by phone within 2 weeks after the first vaccine dose and within 2–6 weeks after the second vaccine dose to complete a questionnaire regarding adverse events.
Clinical assessment of AIIRD
Medical history and the use of medications were recorded. Data regarding disease activity before vaccination were retrieved from patients’ medical records, within up to 3 months before vaccination. Postvaccination disease activity was assessed by an in-person clinical examination within 2–6 weeks after the second vaccine dose. The following disease activity indices were included: Clinical Disease Activity Index, Simplified Disease Activity Index, DAS-28-CRP for RA, Disease Activity in Psoriatic Arthritis, Leeds Enthesitis and Dactylitis Index, Psoriasis Area Severity Index for PsA, Bath Ankylosing Spondylitis Disease Activity Index and Ankylosing Spondylitis Disease Activity Score for axSpA, Systemic Lupus Disease Activity Index for SLE, and patients’ and physician’s global assessment, using a visual analogue scale of 0–10 mm, for vasculitis and inflammatory myositis.
Patient and public involvement
The research question and outcome measures of this study were developed in collaboration with the representatives of patients with AIIRD based on a shared priority to investigate the efficacy and safety of the novel mRNA BNT162b2 vaccine. Patients with AIIRD under the care of the medical centres conducting the trial were actively informed regarding the study and offered to participate. In view of the ongoing COVID-19 pandemic and related stringent restrictions, patients were not involved in the conduct of the study. The main study results will be disseminated to the participants, and we will seek patient and public involvement in the development of an appropriate method of dissemination.
Statistical analysis
Differences between continues variables were tested for significance using the independent-samples t-test. Differences between categorical variables were tested for significance using the χ2 test or Fisher’s exact test (as appropriate). Multivariate models (linear and logistic) were adjusted for age, diagnosis, treatment with methotrexate and anti-CD20. All tests applied were two-tailed. The widths of the intervals have not been adjusted for multiplicity, and the inferences drawn from inferences may not be reproducible. Missing data were assumed as missing at random. No imputations were done. The data were analysed using R V.4.0.5 (R Development Core Team, Vienna, Austria).
Results
Study population
A total of 710 patients with AIIRD and 124 controls vaccinated with the two-dose regimen BNT162b2 mRNA vaccine were enrolled in the study. The final analysis included 686 patients with AIIRD and 121 controls due to missing serology tests (table 1; online supplemental figure S1). RA was the most common disease (n=263), followed by PsA (n=165), SLE (n=101), systemic vasculitis (n=70), axSpA (n=68) and IIM (n=19). Patients with AIIRD included a subgroup of elderly patients aged ≥65 years (32.8%, n=225) and were significantly older than controls, mean age±SD 56.76±14.88 vs 50.76±14.68, respectively; p<0.0001.
Supplemental material
Demographic characteristics of patients with AIIRD and controls
A total of 95.2% (n=653) of patients with AIIRD were treated with immunomodulatory medications (table 2). Glucocorticoids (GC) were used in 18.95% (n=130), at a mean prednisone dose of 6.7±6.25 mg/day. Conventional synthetic disease-modifying antirheumatic drug (csDMARD) monotherapy was used in 23.18% (n=159). Biologic DMARDs were used as a monotherapy or in combination with csDMARDs in 38.19% (n=262) and 13.56% (n=93), respectively. Janus kinase inhibitors (JAKi) were used as a monotherapy or in combination with csDMARDs in 3.06% (n=21) and 3.79% (n=26), respectively. Eighty-seven (12.68%) patients were treated with CD20-depleting (anti-CD20) therapies, of whom 86 received rituximab at a mean dose of 1656.1±623.6 mg. The mean interval between the last dose of rituximab and BNT162b2 vaccination was 51±83 days. One patient received ocrelizumab. During the study period, changes in immunomodulatory drugs after the first vaccine dose were reported in 3% (n=20) of patients and after the second vaccine dose in 4.04% (n=27).
Treatments used in patients with AIIRD
Immunogenicity of the BNT162b2 vaccine
The seropositivity rate was 86% (n=590) in patients with AIIRD compared with 100% in controls (p<0.0001). The level of the S1/S2 antibodies was significantly reduced in patients with AIIRD compared with controls (mean±SD, 132.9±91.7 vs 218.6±82.06; p<0.0001). In patients with PsA, axSpA, SLE and LVV, the seropositive rate was above 90%. In patients with RA, the seropositive rate was 82.1%, whereas the lowest seropositive rate (<40%) was observed in patients with AAV and IIM (table 3).
Immunogenicity of the BNT162b2 messenger RNA vaccine in patients with AIIRD and controls
Effect of immunosuppressive treatments on the immunogenicity of the BNT162b2 vaccine
More than 97% of patients treated with anticytokine therapies, including tumour necrosis factor inhibitors (TNFi), interleukin 17 inhibitors (IL-17i) and interleukin 6 inhibitors (IL-6i), had an appropriate immunogenic response when used as monotherapy (table 4). Anti-CD20 significantly impaired vaccine’s immunogenicity, with the lowest seropositivity rate of 39%. The time interval between the prevaccination administration of rituximab and the BNT162b2 vaccination had a significant impact on the vaccine’s immunogenicity, as shown in figure 1. The seropositivity rate in patients vaccinated within 6 months after rituximab treatment was below 20% but increased to about 50% in patients vaccinated 1 year after rituximab treatment. Similarly, the use of GC, MMF, and abatacept was significantly associated with a lack of humoral response. Seropositivity rate in patients treated with MTX monotherapy and in combination with other treatments was significantly reduced (92% and 84%, respectively), although at a lesser magnitude than with anti-CD20, MMF, and abatacept treatments. The combination of TNFi with MTX reduced the rate of seropositivity to 93% (p=0.04).
Immunogenicity of the BNT162b2 messenger RNA vaccine according to the use of immunosuppressive treatments in comparison with controls

Cumulative seropositive rate according to the interval (days) between the last course of rituximab administration and BNT1622b vaccination. mRNA, messenger RNA.
In the univariate logistic regression model (table 5), age >65 years,diagnosis of RA, IIM, and AAV and treatment with GC, MMF, and anti-CD20, and abatacept were associated with a lack of humoral response to vaccination. Multivariate regression analysis (using PsA, the largest subgroup with the highest seropositivity, as a reference) accounting for age, AIIRD diagnosis, and treatment with MTX and anti-CD20 confirmed these associations (table 5). The impact of GC, MMF, anti-CD20 and abatacept on immunogenicity was independent from the concomitant use of other DMARDs (data not shown).
Unadjusted and adjusted logistic regression models examining the factors associated with seropositivity
Efficacy of the BNT162b2 vaccine
There were no COVID-19 symptomatic disease among AIIRD patients during the study follow-up, whereas one subject in the control group was diagnosed with mild COVID-19 after the second vaccine dose.
Safety of the BNT162b2 vaccine
The prevalence of mild adverse events was similar in patients with AIIRD and controls. There were no serious or major adverse events in the control group. Two patients with AIIRD died after the second vaccine dose. The first patient had a history of AAV, in remission and without any immunosuppressive therapy for 3 years before the vaccination, apart from a low-dose prednisone. Three weeks after the second vaccine dose, she developed fulminant haemorrhagic cutaneous vasculitis with subsequent fatal sepsis. The second patient suffered from PsA which was in remission under treatment with secukinumab and had multiple comorbidities, including diabetes mellitus and ischaemic heart disease. He died from a myocardial infarction 2 months after the second vaccine dose. Adverse events of special interest in patients with AIIRD included uveitis (n=2), herpes labialis (n=1), pericarditis (n=1), and non-disseminated herpes zoster (HZ)15 in five patients after the first vaccine dose and in one patient after the second vaccine dose. One case included HZ ophtalmicus, without corneal involvement (table 6).
Adverse events of the BNT162b2 vaccine in patients with AIIRD and controls
BNT162b2 vaccine effect on disease activity in patients with AIIRD
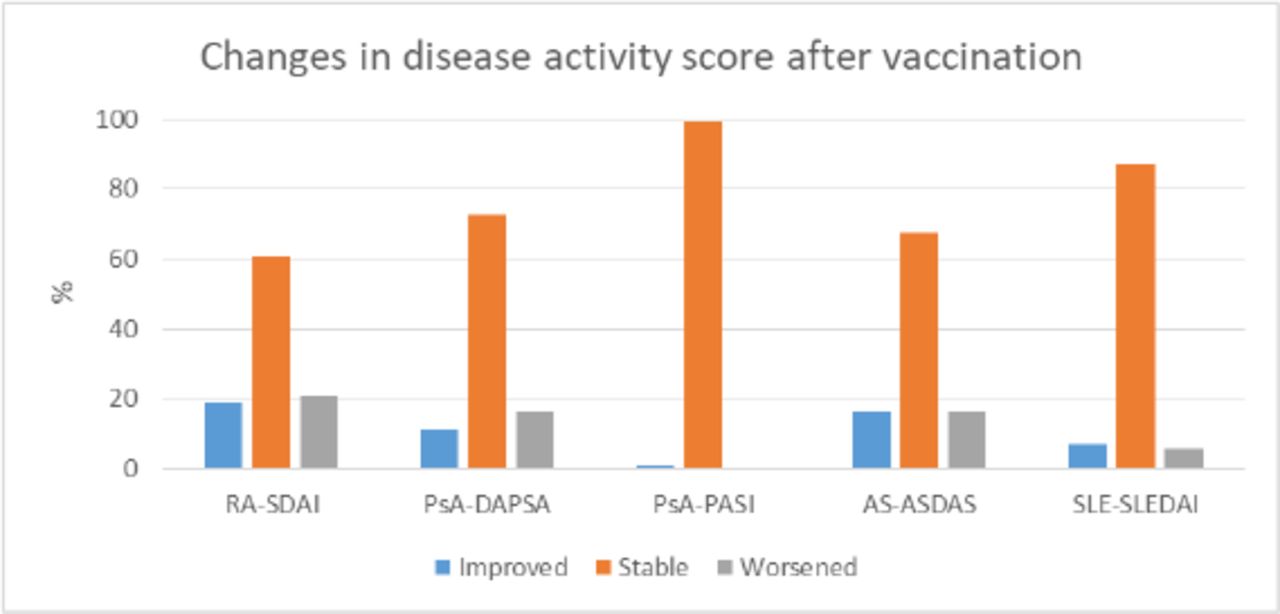
In patients with RA, PsA, axSpA and SLE, the postvaccination indices of disease activity remained stable (figure 2).

{kind=link}
{kind=link}
Disease activity scores before and after completing two doses of BNT162b2 vaccine. Data on prevaccination and postvaccination disease activity measures were available for 165 patients with RA-SDAI, 182 patients with RA-CDAI, 164 patients with RA-DAS-28-CRP, 121 patients with PsA-CDAI, 117 patients with PsA-DAPSA, 131 patients with PsA-PASI, 43 patients with AxSpA-ASDAS, 47 patients with AxSpA-BASDAI and 85 patients with SLE-SLEDAI. ASDAS, Ankylosing Spondylitis Disease Activity Score; axSpA, axial spondyloarthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CDAI, Clinical Disease Activity Index; DAPSA, Disease Activity in Psoriatic Arthritis; PASI, Psoriasis Area Severity Index; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SDAI, Simplified Disease Activity Index; SLE, systemic lupus erythematosus; SLEDAI, Systemic Lupus Disease Activity Index for SLE.
Discussion
The current approach to COVID-19 vaccination of patients with AIIRD is mainly based on data extrapolated from studies on other vaccines. Herein, we report the results of the first large multicentre prospective study conducted during the COVID-19 pandemic demonstrating that BNT162b2 mRNA vaccine was immunogenic in the majority of patients with AIIRD compared with controls, with a seropositivity rate of 86% vs 100%, respectively. S1/S2 IgG levels were significantly lower among patients with AIIRD compared with controls. These findings confirm the results reported by Geisen et al, where considerable immunogenicity was induced by anti-SARS-CoV-2 mRNA vaccines in a small group of patients with chronic inflammatory diseases.4 The mean level of the anti-spike S1/S2 IgG neutralising antibodies measured 2–6 weeks after the second vaccine dose was significantly lower in patients with AIIRD compared with controls in all age groups, consistent with the response to a single dose of mRNA vaccines in patients with rheumatic disease reported by Boyarsky et al,5 raising concerns about the long-term protection of the vaccine in patients with AIIRD.
Our study provided detailed information regarding the impact of various immunosuppressive treatments on vaccine-induced immunogenicity. GC are essential for many patients with AIIRD. The seropositivity rate of patients with AIIRD treated with GC was only 66%. The data are scarce regarding the pure effect of GC on vaccination response in patients with AIIRD, as GC are commonly used in combination with other immunosuppressants and their doses tend to vary over the disease course. A dose of ≥10 mg/day was associated with a reduced vaccine-induced humoral response to pneumococcal vaccine in patients with various inflammatory diseases.16 The mean GC dose in our study population was relatively low (6.2 mg/day), precluding analysis on the dose-dependent effect of GC on vaccination response. MTX represents a cornerstone medication in a spectrum of rheumatic diseases. MTX may reduce humoral response to influenza and pneumococcal vaccines in patients with RA .17–20 Temporary discontinuation of MTX for 2 weeks after vaccination improved the immunogenicity of influenza vaccination in patients with RA.21 22 In our study, the use of MTX as monotherapy or in combination with other treatments was mainly associated with a slightly reduced seropositivity and lower levels of the S1/S2 IgG antibodies compared with controls, suggesting no need for treatment modification with MTX in most cases of anti-COVID-19 vaccination. Holding of MTX may be considered if combined with abatacept or rituximab, in view of a prevalent negative serological response under these regimens. Importantly, anticytokine biologics including TNFi, IL17i and IL6i did not interfere with the production of BNTb262-induced antibodies. This observation is in line with the studies demonstrating a considerable immunogenicity induced by influenza and pneumococcal vaccines in patients with treated with TNFi,20 23–26 IL-6i27–29 and IL-17i.30 31 JAKi, representing a smaller fraction of treatments in our study, demonstrated a minor non-significantly negative effect on the production of BNTb262-induced antibodies. Limited data regarding other vaccines have shown that patients with RA treated with tofacitinib achieved a considerable response to influenza vaccine but an impaired response to a pneumococcal vaccine, especially when combined with MTX.32 Holding of tofacitinib for 1 week prevaccination and postvaccination had little impact on the immunogenicity of either vaccine.32 A considerable pneumococcal humoral response was achieved in patients with RA treated with baricitinib.33
Treatment with anti-CD20 therapies, mainly represented by rituximab in this study, significantly reduced vaccine-induced humoral response, with seropositivity of 41.3% when administered as monotherapy and 36% when administered in combination with MTX. The interval between the administration of rituximab and vaccination had a critical role in predicting the response to the vaccine. Our findings are in line with the previously published data regarding the negative impact of anti-CD20 therapy on the humoral response to various vaccines, although seroprotection could be still achieved after vaccination in rituximab-treated20 26 34–36 and ocrelizumab-treated37 patients. The degree of B-cell recovery at the time of vaccination correlated with the extent of the humoral response to vaccination, as reported for influenza vaccine in patients with RA treated with rituximab.38 In a retrospective analysis of 30 patients with rheumatic diseases treated with rituximab, only 10 patients (33.3%) developed a serological response to anti-SARS-CoV-2 vaccination.39 B-cell depletion was associated with a lack of serological response, based on data available for 11 patients.39 Unfortunately, these data were not available for patients treated with anti-CD20 therapies in our study. As protection from SARS-CoV-2 relies on both humoral and T-cell-mediated immunity,40 41 patients with a deficient humoral response may be still protected by the latter. Treatment with abatacept reduced vaccine-induced humoral response, with a seropositive rate of 71% as monotherapy, reduced to 40% when combined with MTX. Previous data regarding the impact of abatacept on other vaccination-related immunity are conflicting.29 42 Treatment with MMF reduced humoral response to a seropositivity rate of 64% in 28 patients. Consistently, solid organ transplant recipients treated with regimens including MMF were at risk of a negative humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine.43 44
From the standpoint of particular AIIRD at risk of low immunogenic response to vaccine, RA, AAV and IIM were associated with a low humoral response to the vaccine. This finding seems to be at least partially explained by the underlying treatment.
Regarding the safety of vaccination, our study provides a reassurance for a good safety profile of the vaccine, with most adverse events being transient and mild, consistent with two other studies.4 6 No causal link between the two deaths of the patients with AIIRD and vaccination could be established. Other rare adverse events in patients with AIIRD were limited in number and did not seem to cause long-term complications. Occurrence of HZ in six patients with AIIRD merits a special attention as reported by our group.15 In this study, the affected patients were women within the age range of 36–61 years (mean, 49±11 years) with a mild or stable rheumatic disease. Two patients were treated with JAKi and one with rituximab and MMF, indicating a baseline increased risk for HZ, whereas three others had a low level of immunosuppression, calling for a potential causal link between the events.15 As the occurrence of HZ was not specifically captured in the mRNA vaccine clinical trials, no data are available on the postvaccination HZ prevalence in the general population. Case reports on HZ following the BNT162b2 mRNA vaccination in subjects without immunosuppressive treatment45 46 and in one patient with AAV in remission47 were recently published. Further epidemiological studies and surveillance programmes are needed to investigate the prevalence of HZ in vaccinated subjects.
There was no evidence of significant disease flares across different AIIRD. Yet, this should be interpreted with a certain caution due to an exploratory analysis of disease activity assessment performed within a variable prevaccination and postvaccination time frame.
The limitations of our study include a non-randomised design, a lack of matching between patients and controls by age, and the absence of long-term follow-up data. Neither data on B-cell repopulation at the time of vaccination for patients under anti-CD20 therapy nor data on cellular immunity were available.
In summary, the data presented in this study have important implications for the management of anti-COVID-19 vaccination in patients with a wide spectrum of AIIRD. Most immunosuppressive treatments, including csDMARDs, anticytokine biologics and JAKi, can be safely continued without significantly attenuating vaccine-induced immunogenicity. The results of our study do not support withholding MTX and JAKi in relation to COVID-19 vaccination as recommended by the ACR.3
Treatment with GC, rituximab, abatacept in combination with MTX, and MMF was associated with significantly decreased vaccine-induced immunogenicity. Therefore, timing of vaccination has a critical role in these cases. Postponing administration of rituximab and abatacept, especially when combined with methotrexate, when clinically feasible, seems to be reasonable to improve vaccine-induced immunogenicity. Yet, the absence of a humoral response does not preclude T-cell-mediated vaccine-induced immunity, and if shown effective, may serve as a rationale for anti-COVID-19 vaccination of these patients. Importantly, this study provides evidence of overall good tolerance of the BNT162b2 mRNA vaccine in adult patients with AIIRD. Further studies are needed to assess the durability of the humoral vaccination response, T-cell-mediated immunity in patients with a poor humoral response and long-term efficacy and safety of vaccination in patients with AIIRD.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data used to support the findings of this study are included within the article.
Ethics statements
Ethics approval
The study was performed in accordance with the principles of the Declaration of Helsinki and approved by the research ethics committees of the three medical centres: TLV-1055-20, CMC-0238-20 and HMO-0025-21, respectively. The participants signed an informed consent on recruitment into the study.
Acknowledgments
We thank Mr Yoram Neufeld and Ms Maayan Pel for their assistance with data management and Mr Yishai Friedlander, MPH, for performing the statistical analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Correction notice This article has been corrected since it published Online First. The author affiliations have been amended.
Contributors The study was designed, directed and coordinated by OE, the principle investigator. VF, TE, DZ and HP, the sub-investigators, were in charge of the study conducted at all stages. All the MD co-authors recruited participants into the study and evaluated predisease and postdisease activity measures in patients. GS and OS performed the serology tests. SP and SN served as main study coordinators and questioned the study participants regarding the adverse events of vaccination. OE, VF and TE had full access to the study’s data and wrote the article, which was critically reviewed by DP, DZ and HP.
Funding The study was funded by the department’s fund of each medical centre participating in the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.