Article Text

Abstract
No consensus has previously been formed regarding the types and presentations of infectious pathogens to be considered as ‘opportunistic infections’ (OIs) within the setting of biologic therapy. We systematically reviewed published literature reporting OIs in the setting of biologic therapy for inflammatory diseases. The review sought to describe the OI definitions used within these studies and the types of OIs reported. These findings informed a consensus committee (infectious diseases and rheumatology specialists) in deliberations regarding the development of a candidate list of infections that should be considered as OIs in the setting of biologic therapy. We reviewed 368 clinical trials (randomised controlled/long-term extension), 195 observational studies and numerous case reports/series. Only 11 observational studies defined OIs within their methods; no consistent OI definition was identified across studies. Across all study formats, the most numerous OIs reported were granulomatous infections. The consensus group developed a working definition for OIs as ‘indicator’ infections, defined as specific pathogens or presentations of pathogens that ‘indicate’ the likelihood of an alteration in host immunity in the setting of biologic therapy. Using this framework, consensus was reached upon a list of OIs and case-definitions for their reporting during clinical trials and other studies. Prior studies of OIs in the setting of biologic therapy have used inconsistent definitions. The consensus committee reached agreement upon an OI definition, developed case definitions for reporting of each pathogen, and recommended these be used in future studies to facilitate comparison of infection risk between biologic therapies.
- Infections
- Anti-TNF
- Rheumatoid Arthritis
Statistics from Altmetric.com
Background
The advent of biologic therapy has provided great clinical benefit for patients with rheumatoid arthritis (RA) and other immune-mediated inflammatory diseases (IMIDs). ‘Routine’ and ‘opportunistic’ infections have emerged as important complications of various targeted therapies, and much effort has been spent to understand the infectious profiles within and across biologic drug classes.1–3 While the majority of serious infections occurring in this setting (eg, pneumonia, cellulitis, others) are similar to those seen in the general population, it is clear that some infections are much more likely to be associated with immunosuppression (or relative degrees of immunosuppression), occur more severely in those who are immunosuppressed, or have important public health or clinical considerations (eg, tuberculosis (TB)) that distinguish them from ‘routine’ viral or bacterial infections that are frequently encountered in the general population. Further, such infections can be important markers of specific types of immunosuppression (eg, infections that occur with deficient cell-mediate immunity) and can serve as clinical harbingers of specific underlying immune defects.
Efforts have been made to categorise and define these infections as ‘opportunistic’ with such prior efforts tailored by experts to specific settings of immunosuppression. For example, in the HIV setting, the term ‘opportunistic infection’ (OI) has been defined as those infections that are ‘more frequent or more severe because of immunosuppression in HIV-infected persons’.4 This term and its definition are problematic, however, at some level most or all pathogens could be considered ‘opportunistic’ in that they typically are more likely to occur, or present more severely, in immunosuppressed patients. Streptococcus pneumonia would fit this definition of ‘OI’ within the HIV setting and the increased frequency of bacterial pneumonia is discussed within Centers for Disease Controls guidelines on the prevention and management of OIs within HIV.4 This organism also frequently causes disease (and invasive disease) in non-HIV immunocompetent individuals however, and to date, has not been considered or reported as an ‘opportunistic’ pathogen within the field of rheumatology. On the other hand, infections such as TB, generally considered an ‘opportunist’ in many settings of immunosuppression,5 often progress or cause disease in seemingly immunocompetent individuals (including disseminated disease), although certainly disseminated manifestations of disease are more common in immunocompromised individuals including those using some biologics.6 ,7 Unlike for those pathogens that cause disease strictly within immunosuppressed patients (eg, progressive multifocal leucoencephalopathy, PML), for most pathogens the designation of ‘opportunistic’ is neither straightforward nor consistent between immunosuppressive settings.
Given the inherent difficulties in defining the term ‘opportunistic’, and given the lack of a formal definition for this set of infections within rheumatology, a consensus committee was convened to review the published literature reporting the term ‘opportunistic’ infection or the occurrence of pathogens typically considered ‘opportunistic’ (as defined in other settings of immunosuppression) in conjunction with biologic therapy for rheumatic diseases. This information was used to inform the committee's drafting of a proposed working definition of the term ‘opportunistic’ infections and a candidate list of organisms that should be considered as potential ‘opportunistic’ infections in this specific setting of immunosuppression. Further, committee members with subject matter expertise drafted case definitions for each infection. These definitions (see online supplementary appendix) were agreed upon and the committee recommended using these definitions in the reporting of OIs during clinical trials and observational studies where clinical information is available.
Methods
The international consensus committee involved infectious disease, public health and pulmonary physicians with subject-matter expertise in mycobacterial, fungal, viral, bacterial or parasitic infections, as well as rheumatology physicians (JS, XM, LC, MEW) with expertise in immunology and biologic therapy. Upon first discussion session, a systematic approach was agreed upon to identify potential pathogens to be considered potentially ‘opportunistic’ within the setting of biologic therapy in certain immune-mediated inflammatory diseases/rheumatology. First, a candidate list of organisms was created by the committee using guidelines and recommendations for infections deemed clinically important in the area of HIV and transplantation medicine (see online supplementary appendix table S1). Next, a systematic review was conducted with the following goals: (1) to identify reports of infections from the above-mentioned candidate list in conjunction with biologic therapy (2) to identify reports of infections labelled as ‘opportunistic’ by investigators in patients using biologics, and (3) to identify what, if any, case definition for ‘OI’ was used in published clinical trials and observational studies reporting such infections.
Systematic review
We performed a systematic review of published literature reporting OIs within the setting of biologic therapy for rheumatic disease (details on search strategies can be found in online supplementary appendix). Two searches were performed. In both searches identical criteria were used to define subjects (IMID and biologic drug therapy). Subjects were defined as adults or children with a diagnosis of IMID (including RA, psoriasis, psoriatic arthritis, systemic lupus erythematosus, inflammatory bowel disease, spondyloarthritis, microscopic polyangiitis, granulomatosis with polyangiitis, and juvenile idiopathic arthritis) being treated with a biologic agent. Biologic agents included the tumour necrosis factor (TNF)-α antagonists adalimumab, certolizumab pegol, etanercept, infliximab and golimumab, as well as targeted therapies with other mechanisms of action including abatacept, anakinra, belimumab, rituximab, tocilizumab, ustekinumab and the small molecule tofacitinib. The first search identified studies that reported infections or safety issues surrounding receipt of biologic or tofacitinib therapy. The second search used more specific names/definitions to identify studies that reported the specific infections included in our candidate list of OIs. We grouped studies by study type including case-reports/series, observational studies (single and multicentre studies as well as large registries), and clinical trials, open-label and extension studies. Case-series were defined as retrospective studies that didn't provide a denominator (ie, unable to calculate proportion or incidence from data provided). The Medline database was searched from 1 January 1998 to 1 August 2014 for English language studies that met the above criteria. Additional studies were identified via review of references from selected studies. Two reviewers (SAN and KLW) independently reviewed titles and abstracts for inclusion. Information extracted from each study included any definition of OI or report of infection from list of candidate infections and how specific infections were defined (if indicated).
No attempt at formal meta-analysis of results across studies was made for several reasons. First, this was not the objective of the review. Second, it was the opinion of the committee that heterogeneity between methods and case definitions would preclude such a meta-analysis of observational data, and third, a recently published meta-analysis of OIs in the setting of biologic randomized controlled trials (RCTs) was available to the committee.8
Consensus process
The committee convened its first session via conference call in spring of 2014 to generate a preliminary list of candidate pathogens and to plan systematic review strategy. Later, the committee met in person June 2014 to review findings from the systematic review. After reviewing these data, the candidate list of OIs was refined and voted upon by the committee. Pathogens or specific presentations of pathogens were designated as opportunistic only if 80% or more of the committee agreed. Pathogens not reaching this level of agreement were dropped from further consideration. Pathogens known to strictly cause infection only in the immunosuppressed setting (eg, PML) were a priori considered ‘definite’ OIs. For those pathogens known to also occur outside of the immunosuppressed setting, pathogens were considered ‘probable’ OIs if current evidence (supported by the systematic review) suggested they are associated with biologic therapy, or in cases where data were limited, by expert opinion (eg, instances where few patients at risk for a specific pathogen have been treated with biologics). For each pathogen, using the Oxford evidence based medicine criteria, a level of evidence was agreed upon with regards to its particular association with biologic therapy.9
Development of case definitions for candidate pathogens
The committee was divided into subcommittees responsible for the development and refinement of case definitions for each proposed candidate infection. These work groups (viral, mycobacterial, bacterial, fungal, parasitic) of three to four physicians were led by infections disease specialty members of the work group with subject level expertise within each category. Each work group was charged with developing a case definition for each candidate infection. Subsequently, each definition was presented to the consensus group in person, definitions were refined by group consensus and definitions were accepted once 80% or more of the committee were in agreement.
Results
After both searches and deduplication were performed, 2628 references were screened. Additional references were added via review of references from selected papers (see online supplementary appendix figure S1).
We identified 56 (population based and single-centre/multicentre) observational studies that reported incidence rates or risk ratios for OIs overall or specific candidate infections.10–65 Of the identified studies, few reported incidence rates or risk ratios for the overall category of ‘OIs’. Many studies mentioned the term opportunistic and categorised an infection as opportunistic with a statement such as “only one OI, histoplasmosis, was found”. However, only 11 studies provided a definition of infections considered as OIs within their Methods section, with variability in this definition noted across studies (table 1). In addition, it was difficult or impossible to discern whether the definition provided in most studies was complete (ie, formed a priori by the authors) or a representative sample of what the authors considered ‘opportunistic’ in conjunction with their study's findings. Studies more commonly reported incidence rates or risk ratios for specific types of infections from the candidate list, most frequently TB and herpes zoster (figure 1–⇓3; see online table S2 in supplementary materials).
Postmarketing observational studies reporting incidence or risk of opportunistic infections as a combined outcome measure
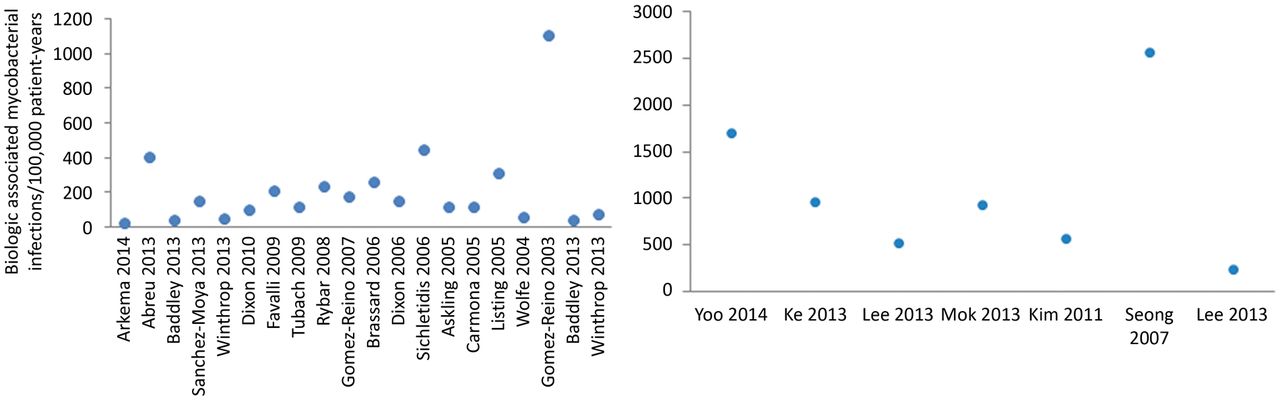
Postmarketing observational studies reporting incidence of mycobacterial infections in Europe/North American and Asia.12 ,21–43 TB incidence (patient-years) in biologic treated patients (incidence reflects combined outcome for anti-TNF therapy unless otherwise indicated): Arkema 2014 21.6/100 000 (anti-TNF, abatacept, anakinra, rituximab, tocilizumab); Abreu 2013 405/100 000 for etanercept (not pictured 792/100 000 for adalimumab and 1337/100 000 for infliximab); Baddley 2013 40/100 000; Sanchez-Moya 2013 146/100 000 (anti-TNF, ustekinumab, efalizumab); Winthrop 2013 49/100 000; Dixon 2010 95/100 000; Favalli 2009 212/100 000; Tubach 2009 116.7/100 000; Rybar 2008 237/100 000; Gomez-Reino 2007 172/100 000; Brassard 2006 257/100 000; Dixon 2006 150/100 000 for infliximab (not pictured 50/100 000 for etanercept and 90/100 000 for adalimumab); Sichletidis 2006 449/100 000; Askling 2005 118/100 000; Carmona 2005 117/100 000; Listing 2005 310/10 000 for infliximab; Wolfe 2004 52.5/100 000 for infliximab; Gomez-Reino 2003 1113/100 000 for infliximab; Yoo 2014 1700/100 000; Ke 2013 954.5/100 000; Lee 2013 519/100 000; Mok 2013 930/100 000 (anti-TNF, rituximab, tocilizumab); Kim 2011 561/100 000; Seong 2007 2558/100 000 for infliximab (not pictured 0/100 000 for etanercept); NTM Incidence (patient-years) in biologic treated patients: Baddley 2013 40/100 000; Winthrop 2013 74/100 000; Lee 2013 230.7/100 000. See online table S2 in supplementary materials for additional information. TB, tuberculosis; NTM, non-tuberculous mycobacteria; TNF, tumour necrosis factor.

Postmarketing observational studies reporting incidence of other bacterial infections (salmonellosis, legionellosis or listeriosis).44–48 Incidence (patient-years) in biologic treated patients (incidence reflects combined outcome for anti-TNF therapy unless otherwise indicated): Lanternier 2013 46.7/100 000; Tubach 2006 33–42/100 000; Davies 2013 51/100 000 pre 2006 (prior to implementation of warning issued in 2006 to avoid high risk foods among those treated with anti-TNF agents), 14/100 000 post 2006; Pena-Sagredo 2009 73/100 000; Pena-Sagredo 2008 25.6/100 000. See online table S2 in supplementary materials for additional information. TNF, tumour necrosis factor.

Postmarketing observational studies reporting incidence of viral infections. Pictured in figure are studies reporting incidence of herpes zoster.11 ,41 ,49 ,52–54 ,56–59 ,62 Incidence (patient-years) in biologic treated patients (incidence reflects combined outcome for anti-TNF therapy unless otherwise indicated): Beukelman 2013 510/100 000; Galloway 2013 1600/100 000; Winthrop 2013 1090/100 000; Dreiher 2012 1930/100 000 for infliximab (not pictured 1390/100 000 for etanercept); Failla 2012 520/100 000 (anti-TNF, rituximab, ustekinumab); Zuber 2011 800/100 000 for etanercept; McDonald 2008 1060/100 000; Strangfeld 2009 1010/100 000. Not pictured Garcia-Doval 2010 32/100 000 (shingles requiring hospitalisation), 26/100 000 (chickenpox requiring hospitalisation); Listing 2005 3380/100 000 for infliximab and 1860/100 000 for etanercept (combined outcome of herpes zoster and simplex); Arkema 2012 2.3/100 000 for PML (undefined class of biologics). See online table S2 in supplementary materials for additional information. PML, progressive multifocal leucoencephalopathy; TNF, tumour necrosis factor.
We identified an additional 139 observational studies (single-centre/multicentre studies and population based) (references available in online supplementary appendix) that did not report incidence or risk ratios of OIs, but rather reported only raw numbers of cases involving candidate OI pathogens (references in online supplementary appendix). In addition to the infections detailed above that had incidence rates or risk ratios reported, we found cases of pneumocystosis, herpes simplex, nocardiosis/actinomycosis, cytomegalovirus, hepatitis B reactivation, hepatitis C progression, histoplasmosis, aspergillosis, candidiasis, coccidiomycosis, cryptococcosis, cryptosporidiosis, Epstein-Barr virus, microsporidiosis, toxoplasmosis, leprosy and leishmaniasis.
Clinical trial data
We identified 368 individual clinical trials of biologics or tofacitinib (including pilot studies, open-label and postmarketing surveillance) (references available in online supplementary appendix). None of these studies provided a specific definition of OIs in their methods or available online supplementary materials. One study by Fleischmann et al66 reported that OIs were defined ‘in accordance with guidelines of the US Centers for Disease Control’. Studies that included post hoc analysis or combined data from multiple trials were more likely to include some definition of OIs but this was not true in the individual studies themselves. For example, Schiff et al67 in a post hoc analysis of patients with comorbidities in an anakinra trial reported a definition of ‘infections that were either unusual due to their severity or setting, or were recognised as OIs (common in immunocompromised patients) or TB (with attention to extrapulmonary presentations) or atypical mycobacterial infections’ but this was not included in the manuscript describing the original trial. A recent meta-analysis reported the risks of OIs in clinical trials of biologic agents in those with RA.8 They included 69 trials involving all currently approved biologics for RA, and defined OIs based on a meta-analysis by Ford and Peyrin-Biroulet68 that evaluated the risk of OIs in patients with inflammatory bowel disease. This list included mycobacterial disease (TB, Mycobacterium avium diseases), oral or oesophageal candidiasis, primary varicella zoster virus infection, herpes zoster, cytomegalovirus, Epstein-Barr virus, nocardiosis, Pneumocystis jirovecii pneumonia, histoplasmosis, herpes simplex infection and ‘other unspecified OIs’. In this analysis the overall risk of OIs was increased (OR 1.79 (1.17, 2.74)) for biologics versus non-biologics (including placebo). The risk was highest for mycobacterial disease (OR 3.73 (1.72, 8.13)) and invasive fungal infections (OR 2.85 (0.68, 11.91)).
Case series/reports
Candidate infections were reported within case report/series format (references available in online supplementary appendix) (see online table S3 in supplementary appendix). The most commonly reported infections included granulomatous infections such as TB, as well as P. jiroveci pneumonia, herpes zoster and hepatitis B reactivation. Other diseases of interest (not on the initial list of candidate infections) identified during the review of case reports/series included human herpes virus 8 (Kaposi's sarcoma) (references available in online supplementary appendix) and Tropheryma whippelli (Whipple's disease) (references available in online supplementary appendix).
Discussion
We evaluated the published literature to identify infections that could be considered opportunistic in the setting of biologic therapy for IMID. Our systematic review suggested that most studies reporting ‘OIs’ lacked a formal definition of this term, and when present, heterogeneity between studies was noted with regards to the types of infections considered or reported as opportunistic. Recognising these findings, the consensus committee chose to construct a formal list of pathogens and/or specific presentations of certain pathogens that should be considered as clinically important in the biologic setting. It is recognised that this list is neither complete nor absolutely ‘correct’, but rather we believe that this list of infections should be considered potential indicators of alterations in host immunity, and that this list and the associated case definitions should be used to standardise reporting of OIs in future biologic and other disease modifying antirheumatic drug clinical trials and observational studies (table 2).
Pathogens and/or presentations of specific pathogens to be considered as opportunistic (or ‘indicator’) infections in the setting of biologic therapy (level of evidence I–V)
The systematic review provided level of evidence for the increased risk of candidate OIs in the setting of biologic therapy. A recent meta-analysis of biologic RCT data grouped OIs into categories (eg, viral, parasitic, etc) and identified either significant or non-significant increases in OI risk in patients exposed to biologics within those trials.8 Population-based observational studies, while dominated by data involving the three anti-TNF therapies longest in the marketplace (etanercept, infliximab and adalimumab), reported relatively high incidence, or when comparator groups were available, elevated risk for combined OI outcomes as well as for most individual pathogens studied. For those studies with combined outcomes, incidence estimates varied markedly between studies. This is in part due to heterogeneity in the OI case definition used across these studies. For example, in the UK, the British Biologic Registry observed OI rates of approximately 200/100 000 in patients using anti-TNF therapies (etanercept, infliximab and adalimumab were studied).21 Likewise in the French Research Axed on Tolerance of Biotherapies (RATIO) registry, the OI rate with the same three anti-TNF agents was similar: 268/100 000.14 ,33 However, just several years later, the Consortium of Rheumatology Researchers of North America (CORRONA) registry published rates over 10 times this estimate within their observational cohort study conducted within North America.15 While various factors can explain some of this difference in risk, much of this risk difference was driven by the inclusion of herpes zoster within the OI case definition of the CORRONA study. In this study, all forms of zoster were considered an ‘OI’, while in the French RATIO Registry and some other studies, only disseminated or multi-dermatomal cases of zoster were considered within the OI definition. Incidence differences between studies also likely reflect differences in endemicity of various pathogens (eg, TB) between regions and populations. Taken together, however, these studies highlight the increased risk in the TNFi setting primarily of those infections associated with granulomatous responses, but also the potential risk elevation with various other intracellular pathogens, and their findings are consistent with signals from RCT data as identified in the RCT meta-analysis included within our systematic review.8 Lastly, some infections traditionally considered ‘opportunistic’ within other settings (eg, Cryptosporidiosis, severe Strongyloides) lack formal study, although in some instances, individual case reports have identified such infections can occur in the biologic setting. In some instances, these infections are endemic to tropical regions in which little population-based study has taken place with regard to biologic therapy.
Given these considerations, the committee developed and ratified a list of pathogens and specific presentations of various pathogens that should be considered OIs in the setting of targeted therapies. The committee roundly acknowledged that some of these infections are frequently seen in immunocompetent individuals, but the committee agreed that when present they raise the likelihood that alterations of host immunity are present. In this manner, the committee felt that these infections would be better considered as ‘indicator infections’ rather than ‘opportunistic’ infections (figure 4). This concept of ‘indicator infection’ was used throughout the committee's deliberations when considering individual infections. It also explains why some presentations of certain infections were included, while others were not. For example, oral candida was included while vaginal candida infections were not. The former is usually seen in patients with local or systemic immunodeficiency, while the latter is much more commonly observed in patients with simple alterations in bacterial flora rather than impaired host immunity. With regards to salmonella and other bacterial diarrhoeal pathogens, only invasive forms were considered to be indicators of potential alternations in the host immunity. Uncomplicated diarrhoeal disease, on the contrary, occurs frequently after exposure within immunocompetent hosts and should not raise the possibility of a host immune defect per se. Herpes zoster, in all forms, was considered to be an OI. While the committee acknowledged that zoster can occur in ‘normal’ hosts, it is readily understood that a diminishment in varicella-specific cell-mediated immunity leads to zoster of all forms69 and that since cell-mediated immunity is potentially altered by some or most biologic therapies, it would be most appropriate to consider all forms of zoster as potential indicators of alterations in the host immunity. This is distinct from primary varicella (‘chicken pox’) which occurs in patients who lack prior exposure no matter their immune function. Lastly, in the case of environmental organisms, only invasive forms of disease should be considered as potential indicator infections, as colonisation states can occur due to environmental exposure particularly in case of underlying lung disease (eg, non-tuberculous mycobacteria or Aspergillus respiratory colonisation).70 ,71

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Definition of indicator infection.
After finalisation of the OI list, the committee constructed case definitions with an attempt to balance sensitivity and specificity for each with regards to surveillance during clinical trials (see online supplementary appendix). It is hoped that such definitions will guide the collection of necessary data during the conduct of clinical trials such that the proposed infections can be accurately categorised and classified. For cases reported during clinical trials, efforts should be made to obtain the necessary clinical, laboratory and imaging data to determine whether the reported infection is confirmed or probable. Although included in the review, little data was retrieved regarding tofacitinib, belimumab and the newer anti-TNF agents. It appears they have a safety profile similar to the biologics although some differences might be present with regards to OIs.72 A higher rate of zoster and other viral infections has been reported with tofacitinib, and like TNF blockers, the rate of TB appears elevated.73 ,74 For the purposes of these recommendations, we believe the pathogen list drafted herein should also be appropriate for this and other small molecules within the pipeline until further data are known.
For TNF blockers and other targeted therapies of novel mechanisms, comparative effectiveness and safety studies are still being conceived and conducted. Further, the ongoing clinical development programmes for drugs of similar and novel mechanism must collect and report rates of OIs to regulatory agencies and the comparison of these rates between therapies has become increasingly important to patients and physicians choosing these therapies. At present, there is great need to develop standardised methodologies and definitions for OIs as observed during these studies. The work of this committee represents a systematic review-informed consensus opinion by infectious disease and rheumatologist experts in this field. It is hoped that the output of this committee will provide a standardised definition for the outcome measure of ‘opportunistic’ infection and, perhaps, push the infectious diseases field to adopt the more clinically relevant term of ‘indicator’ infection for use across all immunosuppressive settings, such that the appearance of these infections should alert the clinician to the possibility of altered host immunity as playing an aetiological role for that infection in the setting of biologic therapy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Funding The consensus process was funded with an unrestricted grant from UCB. SAN was supported by the National Institutes of Health under the training grant 2T32HL083808-06.
Competing interests KLW reported consulting for Genentech, Pfizer, UCB, Abbvie and Amgen, and research grant support from Pfizer, and UCB. JWB reported consulting for Pfizer, Lilly, Merck and Astellas and research grant support from BMS. ML reported attending advisory boards for Gilead and Pfizer. XM reported consulting for BMS, GSK, Pfizer, Sanofi, UCB and research grant support from Biogen, GSK and Pfizer. OL reported consulting for Pfizer, Merck, Astellas, Gilead Sciences, Novartis, UCB and research grant support from Merck, Pfizer and Novartis. MEW reported consulting for Amgen, Abbvie, Bristol Myers Squibb, Genentech, Astra Zeneca, Mediummune, Lilly, Merck, Pfizer, UCB, Crescendo Bioscience, Corrona, Sanofi, Regeneron,Vertex and research grant support from BMS, Crescendo Bioscience and UCB.
Provenance and peer review Not commissioned; externally peer reviewed.