Article Text

Abstract
Background To date, there are no formal guidelines or referral pathways for acute anterior uveitis (AAU) patients developed or endorsed by any international or national societies. The objective of our study was to develop and validate an assessment algorithm for referral from ophthalmologists of appropriate AAU patients to rheumatology that will aid the early diagnosis of the spondyloarthropathy (SpA).
Methods All consecutive patients attending the emergency department of local ophthalmology hospital with AAU, but who did not have a known diagnosis of SpA, were eligible to participate in this study. Patients with any other known cause of AAU were excluded. Two independent cohorts were enrolled. Test algorithm and Dublin Uveitis Evaluation Tool (DUET) algorithm (revised form of test algorithm) were used in these cohorts to identify patients as SpA suspects and non-SpA controls, respectively.
Results STUDY PHASE-1. ALGORITHM DEVELOPMENT COHORT (n=101): After rheumatologic evaluation of the entire cohort, 41.6% (n=42) had undiagnosed SpA. Our test algorithm was noted to have: sensitivity 100% and specificity 53.5%. Further regression analysis resulted in the development of the DUET algorithm which made the following improvements: sensitivity 95%, specificity 98%, positive likelihood ratio (LR) 56.19, and negative LR 0.04. STUDY PHASE-2. DUET ALGORITHM VALIDATION COHORT (n=72): After rheumatologic evaluation of the cohort, 40% (n=29) were diagnosed with SpA, with the following performance of DUET algorithm—sensitivity 96%, specificity 97%, positive LR 41.5 and negative LR 0.03.
Conclusions Approximately 40% of patients presenting with idiopathic AAU have undiagnosed SpA. A simple to apply algorithm is described with excellent sensitivity and specificity.
- Ankylosing Spondylitis
- Spondyloarthritis
- Low Back Pain
Statistics from Altmetric.com
Major strides have been made regarding the treatment of patients with spondyloarthritis (SpA), in particular those with dominant axial involvement. In parallel with a clear improvement in signs and symptoms, acute bony inflammation in the spine and sacroiliac joints, as detected by MRI, reduce impressively with effective treatment.1–3
The stumbling block towards ‘overall success’ in axial SpA remains the poor recognition and consequent late referral to rheumatologists. While there have been some improvements, the average time to diagnosis of SpA from symptom onset remains greater than 6 years,4 which is the longest delay of all the inflammatory joint diseases. Furthermore, axial SpA continues to be active for decades, and in contrast to previous beliefs, it does not burn out over time; rather, the majority of loss of function occurs in the first 10 years from disease onset.5 This clearly underscores the importance of early diagnosis.
Acute anterior uveitis (AAU) is the most common form of uveitis. Although infectious and neoplastic causes exist, the majority of cases of AAU are presumed to be autoimmune in origin. This is reflected in the high prevalence of systemic disease in patients with AAU, most commonly SpA.6 Earlier studies report that half of patients with anterior uveitis are human leucocyte antigen (HLA)-B27 positive, and more than half of these HLA B27-positive patients have underlying SpA.6
Clearly, a very close association exists between AAU and SpA. With this background, the key question that needs to be addressed is which patients presenting with AAU should be referred to rheumatology from ophthalmology services. Some experts have proposed that ophthalmologists should refer all AAU patients to rheumatologists who are HLA-B 27 positive.6–9 However, most ophthalmologists perform no investigations unless prompted to do so by findings from the history and examination that suggest an associated systemic disease, except in recurrent and persistent cases (personal communication with local ophthalmologists). To date, no formal guidelines or referral pathways for AAU patients have been developed and, commonly, the recognition of patients with underlying SpA is dependent on the individual ophthalmologist's expertise and interest. Therefore, in a condition in which significantly delayed diagnosis is common,6 and where AAU may frequently be the first interaction with medical care,10 ,11 an opportunity to identify SpA early is often missed leading to less than ideal care for SpA patients.
The objective of our study was to develop and validate an assessment algorithm to help select appropriate AAU patients for referral from ophthalmology to rheumatology to aid the early diagnosis of the SpA.
Methods
Patients
Consecutive patients attending the emergency department of the Royal Victoria Eye and Ear Hospital, Dublin, with AAU and no known diagnosis of SpA were invited to participate in this prospective study.
Inclusion criteria were: (1) presumed immune-mediated idiopathic AAU in one or both eyes and (2) age over 18 years. Exclusion criteria were: (1) a history of intraocular surgery, or penetrating or blunt eye trauma and (2) any known cause of AAU, for example, known SpA, sarcoidosis, Behcet's syndrome, HSV-1 or Varicella zoster virus (VZV) infection. All patients meeting these inclusion/exclusion criteria were invited to attend a dedicated research clinic where informed consent was obtained prior to further assessment.
Classification criteria used
Axial SpA was classified as per the Assessment of SpondyloArthritis international Society (ASAS) classification criteria.12 Axial SpA (AxSpA) was further subdivided into non-radiographic SpA (NR-SpA) and AS (see online supplementary data). The diagnosis of psoriatic arthritis (PsA) was made as per the internationally agreed CASPAR criteria (Criteria of the ClASsification of Psoriatic ARthritis).13
Clinical assessments
Two independent cohorts designated the Algorithm Development Cohort (recruited from September 2011 to June 2012) and the Dublin Uveitis Evaluation Tool (DUET) Algorithm Validation Cohort (recruited from October 2012 to April 2013) were enrolled to the study from the same geographic location, with all patients meeting the above mentioned criteria.
Study phase 1: algorithm development cohort
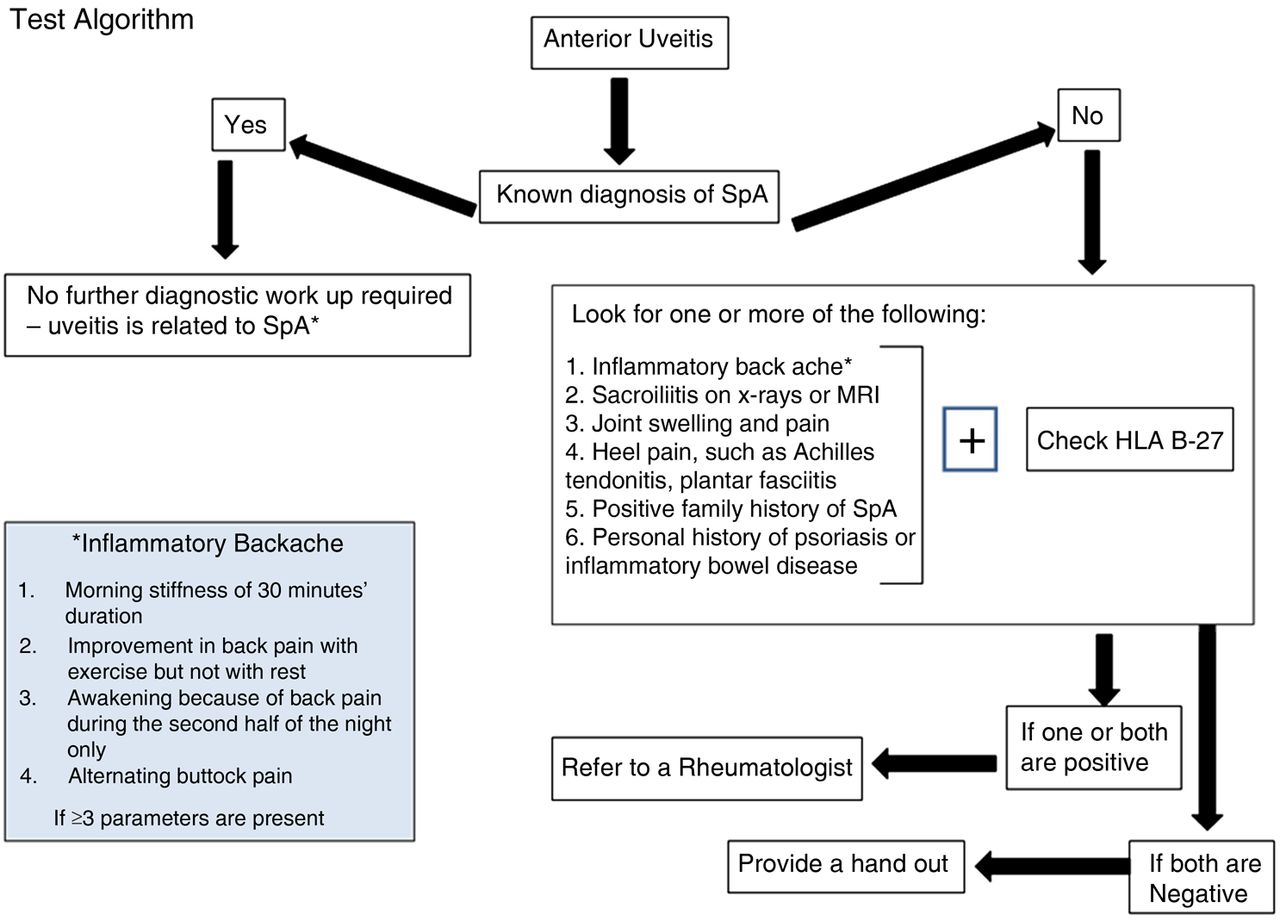
In the eye hospital, patients were assessed through standard clinical history, examination and laboratory work-up before labelling them as idiopathic uveitis. The HLA-B27 status was checked in all patients, and risk factors for SpA in the history were assessed as per the Test Algorithm, which combined clinical features and HLA-B 27 status (figure 1). Patients without risk factors for SpA or who had negative HLA-B27 status remained part of this study and were designated non-SpA controls. All patients, SpA suspects and non-SpA controls, underwent full rheumatologic evaluation by a rheumatologist at St Vincent's University hospital, Dublin.

Test algorithm was designed before the study was initiated. This algorithm, which combined clinical features and human leucocyte antigen (HLA)-B 27 status, was based on the literature search and inclusion of common clinical & associated features of spondyloarthropathy (SpA).
Rheumatologic evaluation included clinical history and examination. Radiographs were taken of sacroiliac joints along with other involved joints of all recruited patients at the time of assessment and, where indicated, other relevant diagnostic investigations including MRI scanning of the sacroiliac joints, and ultrasound scanning of the entheses to confirm the diagnosis. These images were reported by a consultant musculoskeletal radiologist. The study was approved by the local medical research ethics committee.
Study phase 2: DUET algorithm validation cohort
To confirm the findings from the Algorithm Development Cohort, we recruited a second validation cohort from the same geographic area with similar entry and exclusion criteria. The DUET Algorithm, which is a revised form of the test algorithm, was used in this cohort for identifying patients as SpA suspects and non-SpA controls (figure 2). Similar to the development cohort, all patients in the DUET Algorithm Validation Cohort (SpA suspects and non-SpA controls) underwent the same full rheumatologic evaluation by the same rheumatologist at St Vincent's University Hospital, Dublin.

{kind=link}
{kind=link}
DUET algorithm is the revised form of Test algorithm. In study phase-1, the poor specificity of original Test algorithm was noted. This led to its modifications based on the data of study phase-1, which significantly improved its specificity without compromising the sensitivity. HLA, human leucocyte antigen; SpA, spondyloarthropathy.
Statistical analysis
Statistical analysis was performed using the SPSS software, V.17. Significance was defined as p<0.05 (two-tailed). We applied ORs and associated CIs to measure association between different categorical variables. The association of different clinical variables with the diagnosis of SpA was determined using univariate and multivariate logistic regressions.
The efficacy of the proposed algorithm in predicting a diagnosis of SpA was measured in terms of sensitivity and specificity. Positive (PPV) and negative predictive values (NPV) were also determined. Likelihood ratios (LR) were also used to assess how good the referral algorithm was, since these have an advantage over sensitivity and specificity because they are less likely to change with the prevalence of the disorder. Once the test algorithm had been fully evaluated, further simple stepwise reanalysis of the data was undertaken with a view to improving its specificity, which resulted in the development of algorithm version-1 (DUET algorithm). Sample size for replication of the test statistics was determined.
Results
Study phase 1: algorithm development cohort
One hundred and four consecutive patients with presumed idiopathic AAU who attended the ophthalmology emergency department from September 2011 through to June 2012 were recruited to this phase of the study. Table 1 illustrates the demographic details and clinical characteristics of the Algorithm Development Cohort and the DUET Validation Cohort, and demonstrates that there is no significant difference in the characteristics between the two groups. After application of the Test Algorithm, 71 patients were designated SpA suspects and 33 patients were designated non-SpA controls. Two of the SpA suspects and one of the non-SpA controls were lost to follow-up after initial assessment by the ophthalmologist; all other participants (n=101) underwent complete rheumatologic assessment.
Demographic and clinical characteristics of the two cohorts
After rheumatologic evaluation, 42 (41.5%) patients had undiagnosed SpA as per ASAS classification criteria. Forty (95%) of these newly diagnosed SpA patients had AxSpA and the remaining two patients had psoriatic arthritis with predominant peripheral joint involvement as per CASPAR criteria. Among patients with AxSpA, 65% had radiographic SpA (ankylosing spondylitis). The mean age of these newly diagnosed SpA patients was 40.8±13 years; HLA-B27 was negative in only four patients, and mean Bath Ankylosing Spondylitis Functional Index (BASFI) and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores were 1.83±1.58 and 3.58±1.89, respectively. Table 2 compares the demographic and clinical details of these newly diagnosed SpA patients to those who had no SpA after rheumatologic evaluation. Not surprisingly, SpA patients were more likely to be HLA-B27-positive, and had backache; nevertheless, these features were also present in 55.6% and 48% of non-SpA patients revealing their poor individual sensitivities as screening instruments.
Algorithm development cohort—a comparison of demographics and clinical characteristics of newly diagnosed spondyloarthritis (SpA) patients versus those who had no SpA after rheumatologic assessment
On multiple regression analysis, the model only predicted significant association of HLA-B27 positivity and the presence of backache with the diagnosis of SpA (OR 38.6, CI 9.4 to 158, and OR 34.9, CI 5.9 to 206, respectively) after adjusting for age, gender, duration of backache, and recurrent uveitis (see online supplementary data, table 1). Our test algorithm was noted to have a sensitivity of 100%, specificity 53.5%, PPV 61%, NPV 100%, positive LR 2.18, and negative LR of 0.00.
To improve the performance of our test algorithm, detailed stepwise analysis of the data was performed, which revealed that simple modifications of our original test algorithm, for example, providing rheumatologic assessment to only those AAU patients who have backache or who are HLA-B 27-positive, on their own or in different combinations, could significantly improve the detection of underlying SpA (table 3). Although, the presence of backache (age of onset <45 years) and HLA-B 27 positivity seemed a very effective referral tool (sensitivity 90%, specificity 98%), we observed that some psoriasis patients were HLA-B 27 negative and met the CASPAR criteria for the diagnosis of PsA and ASAS classification criteria of SpA. This led to the revision of our referral tool (DUET algorithm), which, as per the data of development cohort would lead to the following improvements: sensitivity 95%, specificity 98%, PPV 97.5%, NPV 96.6%, positive LR 56.19, and negative LR of 0.04.
Further analysis of the data using simple variables, for example, providing rheumatologic assessment to only those AAU patients who have backache or human leucocyte antigen (HLA)-B 27 positive, on their own or in different combinations, and their performance to improve the detection of underlying spondyloarthritis (SpA)
We noted that among the newly diagnosed SpA patients, 62% (n=26) had consulted either their general practitioner (GP) or other allied health professionals for their backache, as follows: GP=47% (n=20), chiropractics=21% (n=9), physiotherapists=26% (n=11). In total, 47 (average 1.8 per patient) medical and other professionals reviewed these 26 patients.
Study phase 2: DUET algorithm validation cohort
To replicate these findings (sensitivity 95%, specificity 98%, PPV 97.5%, and NPV 96.6%), the expected precision of the diagnosis statistics arising from a range of sample sizes was determined. To obtain a 95% CI of at least as narrow as ±10% for all the statistics, a sample size of 44 participants was deemed sufficient, and for a 95% CI width of ±8% on all the statistics, at least 69 participants were needed.
Hence, 74 consecutive presumed idiopathic AAU patients (mean age 40±14 years, 54% male, 54% HLA-B27 positive) who attended the ophthalmology emergency department from November 2012 through to April 2013 were recruited. The DUET algorithm was used in this cohort for identifying patients as SpA suspects and non-SpA controls. Two patients were lost to follow-up prior to rheumatologic assessment. Table 1 describes the demographics of this cohort and also shows that development and validation cohorts were comparable. After rheumatologic evaluation of the cohort of 72 patients, 29 (40%) patients were diagnosed with SpA (mean age of 41±14 years, HLA-B27 positive in 86%, 59% were male, mean BASFI 1.84±1.86, and mean BASDAI of 3.76±2.40). Among these newly diagnosed SpA patients, 28 (96.5%) had AxSpA and only one patient had predominant peripheral joint involvement with a diagnosis of PsA as per CASPAR criteria. Among patients with AxSpA, 71% had radiographic SpA (ankylosing spondylitis). Referral of patients as per the DUET algorithm resulted in very similar statistics compared to its performance in phase 1 of the study—sensitivity 96%, specificity 97%, positive LR 41.5 and negative LR of 0.03 (table 4).
Performance of DUET algorithm in both cohorts
Similar to our development cohort, 72% (21 out of 29) of newly diagnosed SpA patients had interactions with their GP and/or other allied health professionals regarding their backache; in total, 56 (average 2.6) medical and allied health professionals had reviewed these 21 patients, but in each case the diagnosis of SpA was missed.
Discussion
Since, the early diagnosis and treatment of SpA has consistently been shown to improve short and long-term outcomes,14–17 it is imperative that efforts are made to expedite its diagnosis. The use of a long-awaited referral algorithm by ophthalmologists can prove to be the best practice, since uveitis is one of the common initial medical presentations of SpA.
There is a strong case for collaboration between rheumatologists and ophthalmologists, as there are compelling reasons for rheumatologists to be interested in uveitis patients attending ophthalmologists. Earlier studies have shown that about one quarter of patients with uveitis have underlying SpA, and of them about half were diagnosed with SpA after an episode of uveitis.11 A recent Spanish study has shown that 64.6% of uveitis patients had SpA, and this prevalence was to 76.4% among HLA-B27-positive uveitis patients.18 Our study is unique since we included all consecutive patients with presumed idiopathic AAU and found that in two independent cohorts, about 40% of patients had undiagnosed SpA.
From the clinical standpoint, the results of this study are significant in a number of ways. First, our proposed algorithm can be of great significance in streamlining the early and appropriate referrals from ophthalmologists. This is important since early rheumatologic intervention can significantly improve the outlook of this chronic disease—SpA (see online supplementary data). Furthermore, it is known that patients with identical clinical problems receive different care depending on their clinician's knowledge, interest and location. Clinical guidelines may offer a solution by making it more likely that patients will be referred in the same manner regardless of where or by whom they are treated. This study provides the first evidence-based development of such guidelines.
Second, in our cohort, since backache or arthralgia were not the primary reason for presentation to the ophthalmologist, the degree of pain and disability, as reflected by BASFI, BASDAI, was noted to be mild. Nevertheless, typical radiographic features of sacroiliitis were evident in 65% of patients with undiagnosed SpA in our two independent cohorts. This possibly reveals that there can be some disconnect between the severity of back symptoms and the development of structural damage, which further underscores the challenge of identifying these patients (see online supplementary data).
Third, early referral and diagnosis using this algorithm can provide timely initiation of an appropriate management plan which has been shown to reduce structural damage.19 Furthermore, tumour necrosis factor inhibitor (TNFi) therapy, which has revolutionised the management of SpA, has been shown to be significantly more efficacious in disease of shorter duration compared to patients with a disease duration of greater than 10 years.14–16 ,20 Our proposed DUET algorithm has been specifically designed to be used as a referral tool to rheumatology for patients presenting with anterior uveitis, regardless of whether they had axial or peripheral SpA features. We would suggest that it is equally important to try to identify patients with peripheral joint disease as we have recently shown that a diagnostic delay of even 6 months in PsA is associated with poor radiographic and functional outcomes.21 Additionally, our referral tool does not suggest carrying out any imaging studies prior to making a rheumatology referral.
Fourth, although, patients with recurrent uveitis were more likely to have underlying SpA in the development cohort, this relationship was insignificant in the validation cohort. In other words, SpA diagnosis could have easily been overlooked in approximately 40% of both cohorts, should only patients with recurrent uveitis be referred (see online supplementary data).
Finally, poor recognition of SpA happened despite the fact that the majority of patients had sought medical help for their back pain, and the diagnosis of SpA was not considered by their family physicians or other allied health professionals. Inconsistencies in diagnosing inflammatory back pain (IBP) in primary care are well established,22 and recent developments as regards the diagnostic criteria for IBP and AS have not permeated into primary care. In our cohorts, an ideal sensitivity and specificity was achieved without including IBP in the referral pathway, and this is an important strength of our study.
Our study confirms HLA-B27 as a strong predictor for underlying SpA in patients with uveitis. We noted that if HLA-B 27 positivity was used solely as the criterion for making a rheumatologic referral, this would have excellent sensitivity, specificity and LR (90%, 74.5%, 3.5, respectively). Moreover, on multiple regression analysis, presence of HLA-B27 predicted significant association with SpA with an OR of 38.6. Similarly, the presence of backache as a referral criterion among patients with AAU would have a good sensitivity of 95% but a low specificity of 51% for detecting underlying SpA. Interestingly, we noted that if the presence of backache is used along with the coexistence of HLA-B27, it would lead to significant improvement in test statistics with no additional use of resources—laboratory, human or otherwise (DUET algorithm, sensitivity 95%, specificity 98%, LR 56). In our development cohort, there was only one patient who had back pain for less than 3 months; but, the onset of backache in this patient was after the age of 45. Therefore, adding chronicity of back pain to the algorithm did not lead to further improvement of its performance. However, we believe that chronicity of lower back pain is relevant, since acute back pain is so common in the population, which normally resolves in about 12 weeks and can be a source of unnecessary referral. For this reason, we have added the duration of back pain to our DUET algorithm. Interestingly, in our validation cohort, there were four patients who suffered from backache with duration of less than 3 months and had no SpA, which clearly justified its inclusion in the algorithm.
In phase 2 of this study, we tested the DUET algorithm in a second cohort of patients with presumed idiopathic AAU, the validation cohort. The performance of the DUET algorithm in this independent cohort had striking resemblance to its use in the development cohort, confirming that this algorithm is easy to apply and has a strong validity (table 4).
We acknowledge that we used ASAS classification criteria for diagnosing SpA, which was initially developed as classification criteria but are also likely to be useful as diagnostic criteria. Very recently, ASAS group has published the modification of the Berlin algorithm for diagnosing axial SpA.23 If we use this modified Berlin algorithm for diagnosing SpA in our cohorts, a 100% concordance with ASAS classification criteria was noted of phase-1 patients; however, it led to one additional patient being diagnosed with SpA in phase 2. In other words, our newly diagnosed SpA patients largely fulfilled ASAS classification and diagnostic criteria
In conclusion, approximately 40% of patients presenting with idiopathic AAU have undiagnosed SpA. The effective recognition of SpA among patients with uveitis is an achievable goal and requires an integrated multidisciplinary approach. A simple-to-apply algorithm is described with excellent sensitivity and specificity, which will result in appropriate and timely referrals from ophthalmology to rheumatology to the benefit of patients with spondyloarthropathies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
MH and MOR are the joint first authors.
Contributors MH, MOR, PR conceived the study, its design and carried out the work, collection and interpretation of data and manuscript drafting. CCM and OF conceived the study, its design, coordination, data interpretation and manuscript drafting and editing.
Competing interests MH: Unrestricted educational grant from Abbvie; OF has received honoraria and grant support and has been a member of advisory boards for Pfizer, Abbvie, MSD, Roche, UCB, Janssen and Cellgene.
Patient consent Obtained.
Ethics approval Royal Victoria Eye and Ear Hospital, Ethics and Medical Research Committee.
Provenance and peer review Not commissioned; externally peer reviewed.