Article Text

Abstract
Objectives Many female rheumatoid arthritis (RA) patients attempting to conceive have a time to pregnancy (TTP) of >12 months. During this period RA often cannot be treated optimally. We sought to identify clinical factors associated with prolonged TTP in female RA patients.
Methods In a nationwide prospective cohort study on pregnancy in RA patients (PARA study), women were included preconceptionally or during the first trimester. Cox regression analysis was used to study the association of disease characteristics and medication use with TTP.
Results TTP exceeded 12 months in 42% of 245 patients. Longer TTP was related to age, nulliparity, disease activity (DAS28), and preconception use of non-steroidal anti-inflammatory drugs (NSAIDs) and prednisone. These variables were independently associated with TTP, with HRs for occurrence of pregnancy of 0.96 (95% CI 0.92 to 1.00) per year of age, 0.52 (0.38 to 0.70) for nulliparity, 0.81 (0.71 to 0.93) per point increase in DAS28, 0.66 (0.46 to 0.94) for NSAIDs and 0.61 (0.45 to 0.83) for prednisone use. The impact of prednisone use was dose dependent, with significantly longer TTP when daily dose was >7.5 mg. Smoking, disease duration, rheumatoid factor, anti-citrullinated protein antibodies, past methotrexate use, and preconception sulfasalazine use did not prolong TTP.
Conclusions TTP in RA is longer if patients are older or nulliparous, have higher disease activity, use NSAIDs or use prednisone >7.5 mg daily. Preconception treatment strategies should aim at maximum suppression of disease activity, taking account of possible negative effects of NSAIDs use and higher prednisone doses.
- Rheumatoid Arthritis
- DAS28
- NSAIDs
Statistics from Altmetric.com
Introduction
Conceiving a child is a major life event and most adults try to have a child during their reproductive life span. In women with inflammatory rheumatic disease, however, it seems to be more difficult to achieve parenthood.1
Rheumatoid arthritis (RA) is one of the most prominent inflammatory diseases affecting women of child-bearing age. Nearly one-third of female RA patients diagnosed before the completion of child-bearing experience fertility problems.2 They have a prolonged time to pregnancy (TTP), the time between the start of actively trying to conceive and actually becoming pregnant.3 Pregnant RA patients are more likely to have had fertility treatment than pregnant controls.3 ,4 Women with RA have fewer children than women without RA,5–9 and more often fail to conceive at all.7 Hence fertility as well as fecundity seems to be compromised in women with RA.
Subfertility in RA has been studied only in retrospective studies or comparisons of registries.2 ,3 ,5–9 None of these studies have extensively examined the causes underlying the higher subfertility in RA, which may include disease activity, anti-rheumatic medication and immunological factors.
To identify clinical factors associated with a higher rate of subfertility in women with RA, we studied the TTP in consecutive RA patients who participated in a large prospective cohort study in the Netherlands on Pregnancy-induced Amelioration of Rheumatoid Arthritis (the PARA study).10
Methods
Patients
Patients were drawn from the PARA study, an observational nationwide prospective cohort study on pregnancy in RA.10 The study was approved by the Erasmus MC medical ethics review board.
From May 2002 until August 2008, rheumatologists in the Netherlands recruited RA patients defined according to the 1987 revised criteria of the American College of Rheumatology (ACR).11 To be eligible for the PARA study, patients should be actively trying to conceive or already pregnant. Teratogenic drugs, such as methotrexate (MTX), should have been stopped for at least 3 months.
Only patients included preconceptionally or during the first trimester of pregnancy were eligible for the current analysis. If a patient participated twice or more, only the first study episode was included.
Data collection
Patients were preferably visited before conception, during each trimester, and three times after delivery. Patients who did not conceive within 1 year after the first visit were visited again 1 year later. At each visit, patients filled out questionnaires, were interviewed by a research team member, and provided details on variables possibly influencing fertility such as age, parity and smoking habits. Disease activity was measured and serum samples were stored at −80°C. Using a structured questionnaire, the researcher recorded the use, frequencies and dosages of anti-rheumatic medication. At the first visit, the researcher recorded the date the patient first began actively trying to conceive.
Patients who were already pregnant during the first visit were asked when their last menstrual period had started. We calculated the TTP as the time elapsed between the first attempt to conceive and the first day of the last menstrual period before pregnancy. If the date of the last menstrual period was not known by the patient, this date was calculated by subtracting 280 days (40 weeks) from the due date based on sonographic examination during early pregnancy. In several cases the couple started to try for pregnancy after the start of the last menstrual period and succeeded within that first month. To avoid negative values for the TTP, we calculated a fictitious date for the pregnancy test for all patients by adding 28 days to the start of the last menstrual period. These dates were used only in the univariate survival analyses and the Cox regression analyses.
Measurements
Disease activity scores were calculated using the 28-joint Disease Activity Score (DAS28) with three variables based on the C-reactive protein (CRP) level (mg/L).12 We categorised the disease activity scores according to the recommendations of the European League against Rheumatism (EULAR): in remission (DAS28≤2.6), low disease activity (2.6<DAS28≤3.2), intermediate disease activity (3.2<DAS28≤5.1) and high disease activity (DAS28>5.1).13
Rheumatoid factors (RF) were measured by commercial ELISA (HYCOR Biomedical, Garden Grove, California, USA) or by the EliA RF IgM method on the ImmunoCAP 250 (Phadia, Uppsala, Sweden). For RF, the level above which only 5% of healthy controls were tested as positive was defined as positive. The presence of anti-citrullinated protein antibodies (ACPA) was tested by fluoroenzyme immunoassay using EliA CCP on the ImmunoCAP 250. A level >10 U/mL was considered positive.14
Statistics
Values are given as mean±SD, number (percentage) or median (IQR). We calculated inter-group differences using the Student t test or Mann–Whitney U test for continuous variables and Fisher's exact test for categorical variables. Differences between different time points were calculated by a paired t test or the Wilcoxon signed-ranks test.
Differences in TTP per categorised variable were studied using Kaplan–Meier curves. The significance of differences between curves was tested using the log-rank test. A multivariable analysis was performed by Cox regression analysis including age, nulliparity, smoking, disease duration, RF, ACPA, DAS28, non-steroidal anti-inflammatory drug (NSAID) use, prednisone use, sulfasalazine use and previous MTX use. If the patient had not become pregnant at the last time of contact, the TTP was considered censored at the date of the last visit or contact.
A two-sided p value of <0.05 was considered significant. The statistical package Stata/SE V.12.0 for Windows (StataCorp LP, College Station, Texas, USA) was used.
Results
Patients
Of 475 patients recruited from May 2002 to August 2008, 369 were enrolled in the PARA study, and 245 of these were available for the present analyses (figure 1). There were no statistical differences in general characteristics between included and excluded subjects.
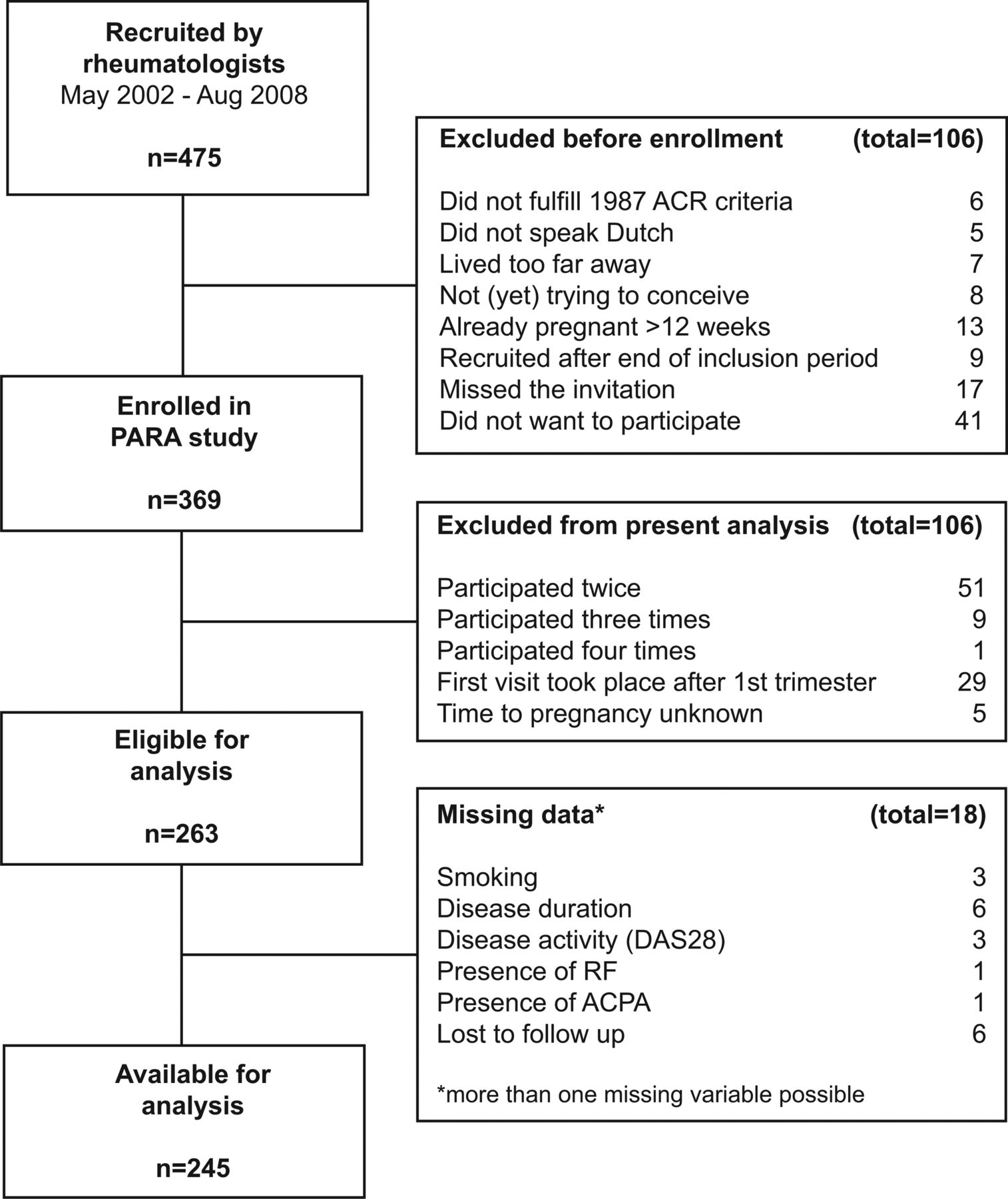
Flow chart showing the number of patients in the Pregnancy-induced Amelioration of Rheumatoid Arthritis (PARA) study who were available for the current analysis. ACPA, anti-citrullinated peptide antibodies; ACR, American College of Rheumatology; DAS28, 28-joint Disease Activity Score; RF, rheumatoid factor.
Study population details are shown in table 1. During the study period, 205 women (84%) conceived, 64 of whom (31%) had a TTP longer than 12 months. These 64 women together with the 40 women who did not become pregnant during follow-up, formed the subfertile group in this cohort (subfertility 42%). In the women who got pregnant, the median TTP was 0.50 year (IQR 0.19–1.28). Pregnancy resulted in a live born baby in 178 women (87%), 26 women (13%) miscarried and there was one intra-uterine fetal death.
Descriptive statistics of the study population
Thirty-five pregnant women had had fertility treatment. These women did not differ significantly from the other subjects. No data on fertility assessments were available.
Since only a few patients used cyclo-oxygenase-2 (COX-2) inhibitors, traditional NSAIDs and COX-2 inhibitors were regarded as one group for analyses.
In 61 women (25%) who were not assessed preconceptionally, only the first trimester DAS28 was available. In women who had been visited both preconceptionally and during pregnancy (n=109), a paired t test showed no significant difference between the preconception DAS28 (3.57±1.1) and the first trimester DAS28 (3.56±1.2; p=0.93). The first trimester DAS28 in these 109 women did not differ from the first trimester DAS28 in women who had not been assessed preconceptionally (3.53±1.1; p=0.86). The first trimester DAS28 was used for further analyses if the preconception DAS28 was missing.
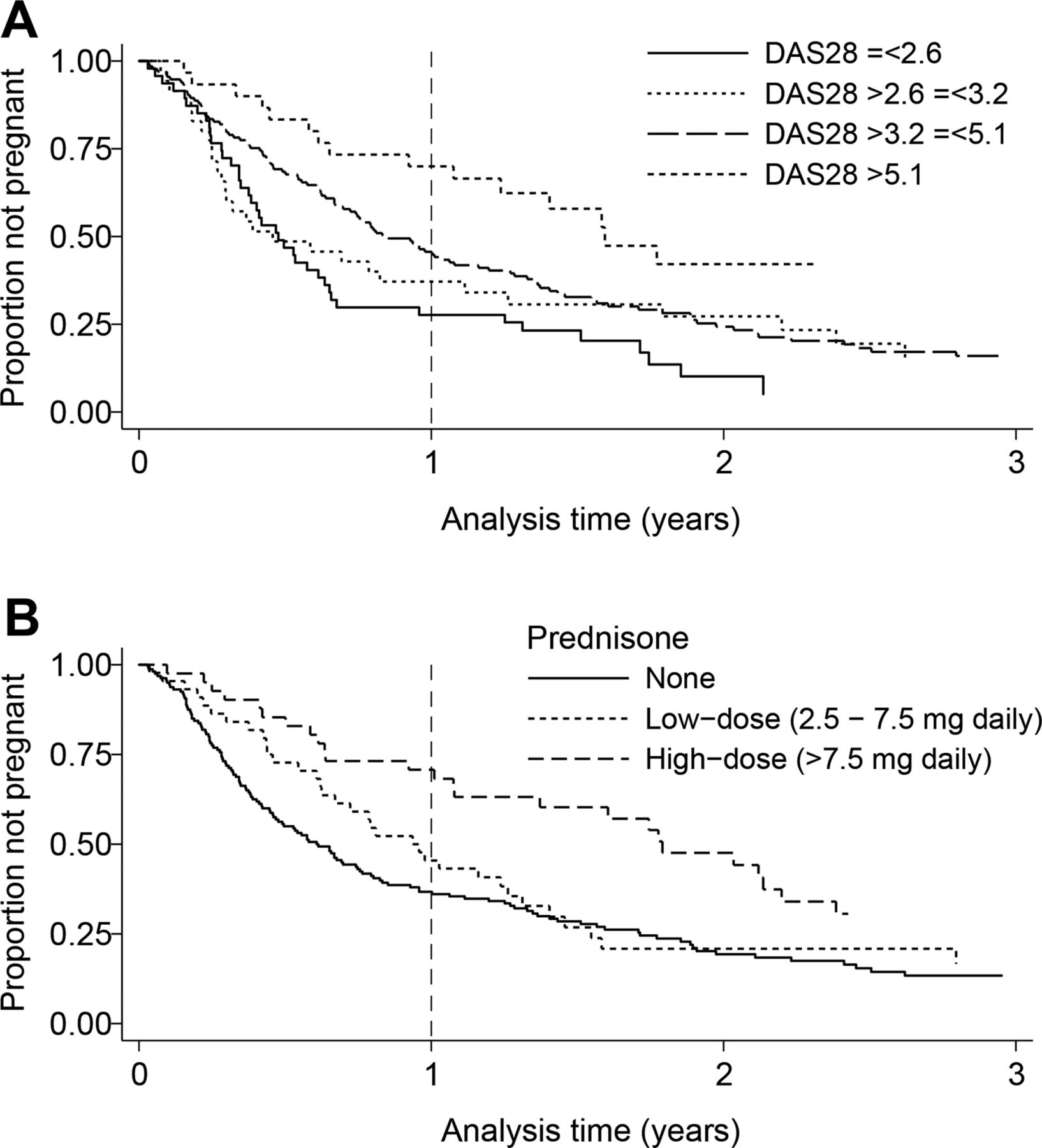
Overall, 67% of women in the high disease activity group (DAS28>5.1), 43% of women in the intermediate disease activity group (3.2<DAS28≤5.1), 37% of women in the low disease activity group (2.6<DAS28≤3.2) and 30% of women in remission (DAS28<2.6) were subfertile (figure 2A).

{kind=link}
{kind=link}
Survival curves showing the time to pregnancy (TTP) in rheumatoid arthritis (RA) patients with (A) various levels of disease activity and (B) different prednisone dosages. When the TTP exceeded 1 year, patients were considered subfertile. If women had not become pregnant at the last time of contact, the TTP was considered censored at the date of the last visit. (A) Patients with high disease activity (DAS28>5.1) had a longer TTP than patients in the other groups (3.2<DAS28≤5.1, p=0.03; 2.6<DAS28≤3.2, p=0.04; DAS28<2.6, p=<0.001). Patients with intermediate disease activity (3.2<DAS28≤5.1) had a longer TTP than patients with RA in remission (DAS<2.6; p=0.008), but TTP did not differ significantly from that in patients with low disease activity (2.6<DAS28≤3.2). The TTP in patients with low disease activity did not differ significantly from that in patients in remission. (B) Patients using high prednisone dosages had a longer TTP than patients using low dosages (p=0.04), and a longer TTP than patients using no prednisone (p=0.002). The TTP between the low-dose group and the group with no prednisone did not differ significantly. DAS28, 28-joint Disease Activity Score.
In the subfertile group, age and DAS28 were significantly higher than in the fertile group (table 2). Subfertile patients were more frequently ACPA positive and used NSAIDs and prednisone more often.
Differences between subfertile and fertile female patients with rheumatoid arthritis
The women who did not become pregnant at all (n=40) had a significantly higher DAS28 (4.14±1.3) than those who became pregnant (3.61±1.1; p=0.008).
RF positivity was more common in women who did not conceive (90%) than in those who did (70%; p=0.01). ACPA was positive in 80% of women who did not conceive compared to 63% of women who did get pregnant (p=0.05). Disease duration did not differ significantly: it was 4.4 (1.7–7.8) years in non-pregnant women and 3.4 (1.2–8.5) years in women who did get pregnant (p=0.76).
Cox regression
Cox regression analysis with multiple variables showed that older age, nulliparity, higher DAS28, preconception use of NSAIDs, and preconception use of prednisone were associated with a longer TTP (table 3). Smoking, time since RA diagnosis, RF positivity, ACPA positivity, past MTX use and preconception sulfasalazine use were not significantly associated with TTP.
Cox regression analysis for occurrence of pregnancy in female patients with rheumatoid arthritis
When analysis was restricted to pregnancies resulting in a live birth, the same factors were identified as significantly associated with TTP (data not shown).
Because DAS28 and prednisone use may show interaction, we introduced an interaction term (DAS28 × daily prednisone dosage) into our model. This showed no significant effect (HR 1.00, 95% CI 0.99 to 1.02; p=0.41).
Prednisone
The effect of prednisone usage on subfertility was further assessed. Eighty-five patients used prednisone in dosages of 2.5–20 mg daily (median 7.5 mg). They were divided into two groups: a low-dose group (≤7.5 mg prednisone daily, n=44) and a high-dose group (>7.5 mg prednisone daily, n=41). In the high-dose group, 66% of women were subfertile compared to 43% in the low-dose group and 36% in the women who did not use prednisone. Kaplan–Meier curves showed a significantly longer TTP in prednisone users versus non-users (p=0.005), and in high-dose users versus low-dose users (p=0.045) (figure 2B). In the Cox regression with the complete variable list, a dummy variable was introduced to distinguish between low-dose prednisone and high-dose prednisone. The HR for low-dose use was not significant (0.83, 95% CI 0.57 to 1 0.21; p=0.33), but use of high-dose prednisone significantly extended the TTP, with an HR of 0.50 (0.33 to 0.76; p=0.001). The significance of other variables in the analysis did not change.
A subgroup analysis on patients with DAS28<3.2 still showed a significant association between prednisone use and a longer TTP (HR 0.21, 95% CI 0.10 to 0.45; p<0.001).
DAS28 after 1 year
A subgroup of women who did not conceive within 12 months after the first visit, were revisited after 1 year. In the 17 patients who were still actively trying to conceive, the DAS28 for this visit did not differ from the DAS28 1 year earlier (3.96±1.6 vs 3.91±1.8; p=0.85).
Discussion
In this prospective cohort of female RA patients, we showed that a prolonged TTP in RA is related to older age, nulliparity, higher disease activity, and preconception use of NSAIDs and prednisone (>7.5 mg daily).
Forty-two percent of the patients had a TTP exceeding 12 months. This is much higher than the reported subfertility of 9–20% in the general population with a pregnancy wish in Western countries.15 ,16 The median TTP of 6 months in pregnant RA women in our study is significantly longer than in the general Western European population, where 50% of women have a TTP of 3 months and approximately 70% conceive within 6 months after starting unprotected intercourse.16
The fertility rates in this study are similar to those shown by other studies in female RA populations of reproductive age. The proportion of 42% of subfertile women in our study is consistent with a recent study that reported subfertility in 36% of women with RA diagnosed before family completion.2 A Danish birth registry study found a TTP exceeding 12 months in 25% of pregnant RA women.3 Since they did not include miscarriages or women who failed to conceive at all, these data are compatible with our study.
We identified various risk factors for a longer TTP in women with RA, including older age and nulliparity, which were already known to prolong TTP. As in the general population, higher age negatively affects fertility.17 The mean age in our patient group was 31.3±3.9 years, which is slightly older than the mean maternal age at child birth in the Netherlands (31.0 years in 2000–2010).18 Therefore, we cannot explain the higher subfertility in this patient group by age alone.
Concerning nulliparity, it has been shown that a previous pregnancy increases the chance of a subsequent pregnancy, at least in subfertile couples.19 In our study, 58% of patients were nulliparous compared to 47% in the general Dutch population.4 Having a chronic disease may influence the time at which a woman starts having a family, or the choice to have fewer children, thereby explaining the higher number of nulliparous patients.20 It seems unlikely that the higher number of nulliparous patients reflects a selection bias, with relatively more subfertile women enrolling in our study, since the subfertility rate in this study is comparable with that reported in the literature.2 ,3 Furthermore, it is not expected that this influenced the proper identification of RA-associated risk factors for a prolonged TTP in this study.
RA related factors that were associated with TTP in our cohort were DAS28, and preconception use of NSAIDs and prednisone >7.5 mg. To our knowledge, RA disease activity has not previously been related to reduced fertility, probably because of the retrospective design of previous studies. In inflammatory bowel disease, disease activity has been related to subfertility, but this is mainly attributed to tubal and ovarian dysfunction due to local inflammation or as a result of previous surgery.21
The impact of high RA disease activity on fertility could be mediated via inflammatory mediators, since many cytokines, chemokines and growth factors play an important role in the preimplantation blastocyst–endometrial interactions.22 We have previously shown that high IL-6 serum levels are associated with lower birth weight in children born to women with RA.23
Since DAS28 did not increase during a 1-year follow-up in the preconception period, it is not likely that increasing disease activity over time explains an even longer TTP in these women.
The second factor is the use of NSAIDs. NSAIDs may interfere with ovulation, implantation and placentation through inhibition of prostaglandin synthesis.10 ,24 ,25 Selective COX-2 inhibitors seem to inhibit ovulation more potently than traditional non-selective NSAIDs. However, this finding is only based upon case reports or small case series.24
Finally, the use of prednisone prolongs the TTP. Although prednisone has been considered not to have any effect on fertility when used for the treatment of chronic inflammatory diseases,26 ,27 our results show that in daily dosages >7.5 mg it does indeed significantly lengthen the TTP. A possible explanation for this may be the transient suppression of the hypothalamic-pituitary-ovarian axis by glucocorticoids. Glucocorticoids in therapeutic dosages have been shown to decrease luteinising hormone pulse frequency from the pituitary gland.28 ,29 Another possibility is a direct effect of prednisone on ovarian function or on the endometrium.30–32
Use of MTX in the past did not have a negative effect on the TTP. This is in contrast to animal studies, where MTX has been shown to cause a reduction in the number of primordial follicles (ie, ovarian reserve) and a subsequent loss of ovarian function.33 We have previously shown that short-term MTX use in early RA does not affect ovarian reserve.34 As the women in the current study had been using MTX for several years, our results suggest that long-term use of MTX also does not have a negative effect on ovarian function and fertility.
Even in the era of biologicals, our results are still relevant due to safety concerns regarding biologicals during pregnancy, and because not all women have access to them. Therefore, prednisone and NSAIDs are still important anti-rheumatic drugs during pregnancy and the preconception period.
It has been reported that women with inflammatory joint disease are more often nulliparous when diagnosed in early adulthood than when diagnosed in childhood or at a later age.9 However, introducing age at diagnosis into our analysis has no significant effect on TTP (data not shown).
A reduced frequency of intercourse may also play a role in explaining the observed fertility problems. If a patient has chronic pain (eg, in the hip or knee joints), intercourse frequency is expected to be lower, thereby diminishing the chance of conception in a given month. This was not assessed in our study, but after adjustment for DAS28, which reflects a patient's pain, other variables are still significant.
Body mass index (BMI) is also known to affect fertility. Overweight and underweight women both have a higher chance of ovulation disorders.35 Overweight women with regular menses also have an increased risk of subfertility.36 The association between RA and BMI is less clear.37 ,38 BMI was not recorded for the women included in the PARA study, but the median BMI for women aged 18–42 years in a representative Dutch RA cohort was 24.2 (21.9–28.3).34
Based upon our results, it should be recommended that RA patients trying to conceive should strive for low disease activity, thereby avoiding NSAIDs and daily dosages of prednisone exceeding 7.5 mg. The treatment of some women in our cohort, reflecting common care for women with RA during the preconception period, does not seem to have been optimal as two-thirds of patients had a DAS28>3.2. While nearly a third of these women used no medication, over a third received monotherapy with sulfasalazine or prednisone. Combination therapy with sulfasalazine, prednisone and hydroxychloroquine in these patients may have resulted in lower disease activity.
Suppression of disease activity in RA women who wish to conceive is also important for the outcome of pregnancy. Higher DAS28 is associated with lower birth weight and rapid postnatal catch-up growth, which are both related to worse cardiovascular and metabolic profiles in adults.4 ,39 Use of prednisone during pregnancy is associated with lower birth weight due to delivery at a lower gestational age and with higher cortisol levels in the offspring.4 ,40 Furthermore, women with high DAS28 more often undergo caesarean section.4
As the proportion of subfertile women is much larger in the RA population than in the general population,15 patients likely to have a longer TTP might be helped by early consultation with a gynaecologist on options for reproductive treatment. If the TTP can be limited in these patients, this may prevent extended suboptimal treatment and consequently functional disability and progression of joint damage.
The results of our study also have implications for patients with conditions other than RA. When patients wish to conceive and are using high daily dosages of prednisone, or NSAIDs on a regular basis, their treatment should be critically evaluated. Similarly in patients with other inflammatory auto-immune diseases, disease activity may impair fertility and should be suppressed whenever possible.
Acknowledgments
We are grateful to all patients participating in the PARA study, as well as to the Dutch rheumatologists for their voluntary contributions to the study. We thank Yaël de Man, Fleur van de Geijn, Esther Gasthuis and all research assistants and laboratory workers for their help with data collection.
References
Footnotes
Handling editor Tore K Kvien
Contributors JH, RD, JL and JB: study design and analysis plan; JH and RD: data acquisition; JB: cleaning of data; JB and RD: analysis; JB and RD: draft paper; JH, JL, RD, JB: revision of paper and final approval for publication.
Funding This study was funded by the Dutch Arthritis Association (Reumafonds) (project number: 12-1-305).
Competing interests None.
Ethics approval The Erasmus MC Medical Ethics Review Board approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.