Article Text

Abstract
Therapy for polymyalgia rheumatica (PMR) varies widely in clinical practice as international recommendations for PMR treatment are not currently available. In this paper, we report the 2015 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) recommendations for the management of PMR. We used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology as a framework for the project. Accordingly, the direction and strength of the recommendations are based on the quality of evidence, the balance between desirable and undesirable effects, patients’ and clinicians’ values and preferences, and resource use. Eight overarching principles and nine specific recommendations were developed covering several aspects of PMR, including basic and follow-up investigations of patients under treatment, risk factor assessment, medical access for patients and specialist referral, treatment strategies such as initial glucocorticoid (GC) doses and subsequent tapering regimens, use of intramuscular GCs and disease modifying anti-rheumatic drugs (DMARDs), as well as the roles of non-steroidal anti-rheumatic drugs and non-pharmacological interventions. These recommendations will inform primary, secondary and tertiary care physicians about an international consensus on the management of PMR. These recommendations should serve to inform clinicians about best practices in the care of patients with PMR.
- Polymyalgia Rheumatica
- Corticosteroids
- Giant Cell Arteritis
- Treatment
- Patient perspective
Statistics from Altmetric.com
Guidelines and recommendations developed and/or endorsed by the American College of Rheumatology (ACR) are intended to provide guidance for particular patterns of practice and not to dictate the care of a particular patient. The ACR considers adherence to these guidelines and recommendations to be voluntary, with the ultimate determination regarding their application to be made by the physician in light of each patient's individual circumstances. Guidelines and recommendations are intended to promote beneficial or desirable outcomes but cannot guarantee any specific outcome. Guidelines and recommendations developed or endorsed by the ACR are subject to periodic revision as warranted by the evolution of medical knowledge, technology, and practice.
The American College of Rheumatology is an independent, professional, medical and scientific society which does not guarantee, warrant, or endorse any commercial product or service.
Introduction
There are wide variations in the treatment of polymyalgia rheumatica (PMR) with respect to glucocorticoid (GC) dosages, tapering strategies, use of disease modifying anti-rheumatic drugs (DMARDs) and duration of treatment. Up to 29–45% of patients with PMR do not adequately respond to GCs within 3–4 weeks. Relapses and long-term GC dependency are common.1–4 GC side effects are frequently observed, occurring in around 50% of patients, and present a further challenge.5 ,6 Well considered, international recommendations can serve to standardise practice and improve patient care.
Primary objective of the recommendations
These recommendations are intended for the management of patients with PMR in various settings and are based on clinical evidence and expert opinion including informed patient decision-making.
Target population
The target population are patients with PMR based on clinician diagnosis which may be supported by currently available diagnostic or classification criteria.3 ,4 ,7–11 Management of PMR with concomitant giant cell arteritis (GCA), rheumatoid arthritis (RA) or other conditions that present with PMR features or mimic PMR is not addressed by these recommendations.
Target users
The target users of these recommendations are primary, secondary and tertiary care physicians (that is, general practitioners (GPs), specialists in general (internal) medicine and rheumatologists).
Methods
For a detailed description of methods, see online supplementary file S1.
In brief, we used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology as a framework.12–15 We formulated 12 PICO (problem/population, intervention, comparison, and outcome) questions on interventions and 10 questions on prognostic factors (see online supplementary box S1A and S1B, or the accompanying paper by Dejaco et al16). The systematic literature review (SLR) was conducted by two investigators (CDe and YPS) using Ovid MEDLINE, Embase, PubMed, CINAHL, Web of Science and the Cochrane Library databases (from January 1970 until April 2014), and applying the thesauri of PMR, text words, abbreviations and truncated text words. Outcome parameters used in the SLR may be found in supplementary box S2. Quality appraisal of interventional and prognostic studies was performed using GRADE17 ,18 and the Quality in Prognostic Studies (QUIPS) tool,19 respectively. According to GRADE methodology, a guideline panel should consider the following aspects when formulating recommendations: (1) overall quality of evidence; (2) balance between desirable and undesirable effects; (3) patients’ and clinicians’ values and preferences; and (4) resource use. External evidence (from other American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) recommendations; see online supplementary table S1 for details) on safety aspects related to the use of non-steroidal anti-inflammatory drugs (NSAIDs), GCs and methotrexate (MTX) was taken into account as indirect evidence, in order to identify the optimal trade-off between the benefit and harm of interventions. Prognostic factors were used to build subgroups and to adapt the recommendations based on the presence or absence of unfavourable prognostic factors. Final recommendations were either ‘in favour’ or ‘against’ an intervention, and were graded as ‘conditional’ or ‘strong’. A strong recommendation in favour (against) was considered when the panel was certain that benefits did (did not) outweigh risks and burdens, the preferences/values of patients were met (not met) and resource use was reasonable (unreasonably high). If uncertainty existed, a conditional recommendation was made.
Results
The results of the SLR are reported in a separate manuscript.16 See online supplementary file S2 for a summary of the SLR and external evidence considered by the guideline panel.
General aspects
These recommendations should be understood as clinical advice and do not dictate the care of a particular patient. The EULAR and ACR consider adherence to these recommendations to be voluntary, with the physician making the ultimate decision to apply them in light of each patient's individual circumstances.
Overarching principles for the management of PMR
The group agreed upon several principles deemed to be fundamental aspects of clinical care in PMR as detailed in box 1. These principles have not directly resulted from the SLR, but are consensus based. They are intended as a framework for the implementation of the specific treatment recommendations and are of a general ‘overarching’ nature, a concept adapted from earlier EULAR recommendations.20–22
Summary of the 2015 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) recommendations for the management of polymyalgia rheumatica (PMR)
Target population:
Patients with PMR based on clinician diagnosis which may be supported by currently available diagnostic or classification criteria.3 ,4 ,7–11
Overarching principles for the management of PMR:
Adoption of a safe and specific approach to ascertain the PMR case definition. The clinical evaluation should be directed towards exclusion of relevant mimicking (eg, non-inflammatory, inflammatory (such as giant cell arteritis or rheumatoid arthritis), drug-induced, endocrine, infective and neoplastic) conditions.
Every case of PMR should have the following assessments prior to the prescription of therapy (primary or secondary care):
Documentation of a basic laboratory dataset. This will help to exclude mimicking conditions and establish a baseline for monitoring of therapy. This should include rheumatoid factor and/or anti-cyclic citrullinated peptide antibodies (ACPA), C-reactive protein and/or erythrocyte sedimentation rate (ESR), blood count, glucose, creatinine, liver function tests, bone profile (including calcium, alkaline phosphatase) and dipstick urinalysis. Additional investigations to consider are protein electrophoresis, thyroid stimulating hormone (TSH), creatine kinase and vitamin D.
Depending on clinical signs and symptoms and the likelihood of the alternative diagnoses, additional more extensive serological tests such as anti-nuclear antibodies (ANA), anti-cytoplasmic neutrophil antibodies (ANCA) or tuberculosis tests may be performed to exclude mimicking conditions. Additional investigations such as chest radiographs may be considered at the discretion of the physician in order to exclude other diagnoses.
Determination of comorbidities (particularly hypertension, diabetes, glucose intolerance, cardiovascular disease, dyslipidaemia, peptic ulcer, osteoporosis (and particularly recent fractures), presence of cataract or (risk factors for) glaucoma, presence of chronic or recurrent infections, and co-medication with non-steroidal anti-inflammatory drugs (NSAIDs) as outlined in Smolen et al21 and Gossec et al,22 other relevant medications and risk factors for steroid-related side effects. Female sex was associated with a higher risk of glucocorticoid (GC) side effects in low to moderate quality studies.23–25
The role of risk factors for relapse/prolonged therapy is not clear yet. Baseline factors that were associated in low to moderate quality studies with a higher relapse rate and/or prolonged therapy in PMR studies were: female sex,24 ,26 high ESR (>40 mm/1st hour)26–31 and peripheral inflammatory arthritis.32 A number of equally low to moderate quality studies, however, failed to demonstrate an association between these factors and relapse/prolonged therapy.27–30 ,32–44
Consideration of specialist referral, particularly in case of atypical presentation (such as peripheral inflammatory arthritis, systemic symptoms, low inflammatory markers, age <60 years), experience of or high risk of therapy-related side effects, PMR refractory to GC therapy, and/or relapses/prolonged therapy.
Treatment of PMR patients should aim at the best care and must be based on a shared decision between the patient and the treating physician.
Patients should have an individualised PMR management plan. Patient perspective and preferences should be considered in the individualised choice of initial GC dose and subsequent tapering of GCs in PMR.
Patients should have access to education focusing on the impact of PMR and treatment (including comorbidities and disease predictors) and advice on individually tailored exercise programmes.
Every patient treated for PMR in primary or secondary care should be monitored with the following assessments: risk factors and evidence for steroid-related side effects, comorbidities, other relevant medications, evidence and risk factors for relapse/prolonged therapy. Continuous documentation of a minimal clinical and laboratory dataset should be conducted while prescribing GCs. Follow-up visits are suggested every 4–8 weeks in the first year, every 8–12 weeks in the second year, and as indicated in case of relapse or as prednisone is tapered and discontinued.
It is important for patients to have rapid and direct access to advice from doctors, nurses or trained allied healthcare staff to report any changes in their condition such as flares and adverse events.
Specific recommendations for the management of PMR patients:
The panel strongly recommends using GC instead of NSAIDs in patients with PMR, with the exception of possible short-term use of NSAIDs and/or analgesics in PMR patients with pain related to other conditions. No specific recommendation can be made for analgesics.
The panel strongly recommends using the minimum effective individualised duration of GC therapy in PMR patients.
The panel conditionally recommends using the minimum effective GC dose within a range of 12.5–25 mg prednisone equivalent daily as the initial treatment of PMR. A higher initial prednisone dose within this range may be considered in patients with a high risk of relapse and low risk of adverse events, whereas in patients with relevant comorbidities (eg, diabetes, osteoporosis, glaucoma, etc) and other risk factors for GC-related side effects, a lower dose may be preferred. The panel discourages conditionally the use of initial doses ≤7.5 mg/day and strongly recommends against the use of initial doses >30 mg/day.
The panel strongly recommends individualising dose tapering schedules, predicated to regular monitoring of patient disease activity, laboratory markers and adverse events.
The following principles of GC dose tapering are suggested:
Initial tapering: Taper dose to an oral dose of 10 mg/day prednisone equivalent within 4–8 weeks.
Relapse therapy: Increase oral prednisone to the pre-relapse dose and decrease it gradually (within 4–8 weeks) to the dose at which the relapse occurred.
Tapering once remission is achieved (following initial and relapse therapies): Taper daily oral prednisone by 1 mg every 4 weeks (or by 1.25 mg decrements using schedules such as 10/7.5 mg alternate days, etc) until discontinuation given that remission is maintained.
The panel conditionally recommends considering intramuscular (i.m.) methylprednisolone as an alternative to oral GCs. The choice between oral GCs and i.m. methylprednisolone remains at the discretion of the treating physician. In one clinical trial, a starting dose of 120 mg methylprednisolone i.m. injection every 3 weeks was applied.23
The panel conditionally recommends using a single rather than divided daily doses of oral GCs for the treatment of PMR, except for special situations such as prominent night pain while tapering GCs below the low-dose range (prednisone or equivalent <5 mg daily).
The panel conditionally recommends considering early introduction of methotrexate (MTX) in addition to GCs, particularly in patients at a high risk for relapse and/or prolonged therapy as well as in cases with risk factors, comorbidities and/or concomitant medications where GC-related adverse events are more likely to occur. MTX may also be considered during follow-up of patients with a relapse, without significant response to GC or experiencing GC-related adverse events. MTX has been used at oral doses of 7.5–10 mg/week in clinical trials.24–27
The panel strongly recommends against the use of TNFα blocking agents for treatment of PMR.
The panel conditionally recommends considering an individualised exercise programme for PMR patients aimed at the maintenance of muscle mass and function, and reducing risk of falls especially in older persons on long-term GCs as well as in frail patients.
The panel strongly recommends against the use of the Chinese herbal preparations Yanghe and Biqi capsules in PMR patients.
Specific recommendations
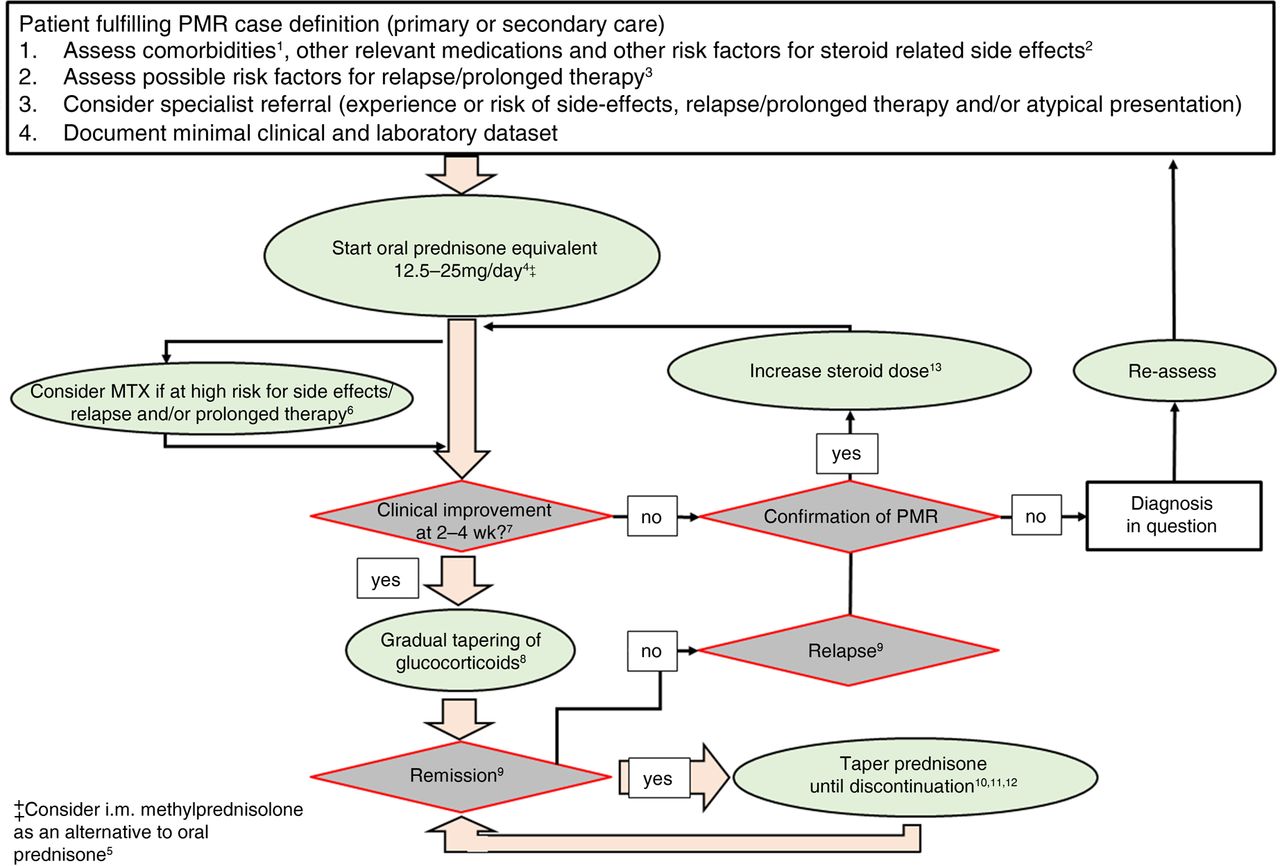
See box 1 for a summary of the recommendations. A flow-chart for the management of PMR patients is depicted in figure 1.

{kind=link}
Algorithm based on the 2015 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) recommendations for the management of polymyalgia rheumatica (PMR). The algorithm is applied to patients with PMR based on clinician diagnosis which may be supported by currently available diagnostic or classification criteria.3 ,4 ,7–11 The algorithm assumes the consideration of overarching principles emphasising the importance of assessing comorbidities, other relevant medications and possible risk factors for steroid-related side effects and relapse/prolonged therapy. In addition, patients diagnosed in primary care should be considered for specialist referral, particularly in case of atypical presentation (such as peripheral inflammatory arthritis, systemic symptoms, low inflammatory markers, age <60 years), experience or high risk of therapy-related side effects and/or relapse/prolonged therapy. A minimal clinical and laboratory dataset should be documented in each patient before prescribing therapy. 1Examples for comorbidities associated with an increased risk of glucocorticoid (GC)-related side effects are (according to Duru et al32 and Hoes et al35): hypertension, diabetes, glucose intolerance, cardiovascular disease, dyslipidaemia, peptic ulcer, osteoporosis (and particularly recent fractures), presence of cataract or (risk factors for) glaucoma, presence of chronic or recurrent infections, and co-medication with NSAIDs. 2A baseline factor that was associated with a higher risk of GC-related adverse events in PMR studies was: female sex.37–39 3The role of risk factors for relapse/prolonged therapy is not yet clear. Baseline factors that were associated with a higher relapse rate and/or prolonged therapy in PMR studies were: female sex,38 ,47 high erythrocyte sedimentation rate (ESR) (>40 mm/1st hour)47–51 ,53 and peripheral inflammatory arthritis.54 A number of studies, however, failed to demonstrate an association between these factors and relapse.48–51 ,54 ,67–78 4Use the minimum effective dose out of a range of 12.5–25 mg prednisone equivalent daily: a high risk of relapse/prolonged therapy favours a higher dose, while a high risk of side effects favours a lower dose. 5In one randomised controlled trial, 120 mg methylprednisolone intramuscular (i.m.) injection was used every 3 weeks as a starting dose.23 I.m. methylprednisolone may not be available in all countries and the possible long-term benefit in terms of efficacy and GC-sparing effects of this preparation is unknown. 6Methotrexate (MTX) has been used at oral doses of 7.5–10 mg/week in clinical trials.24–27 7Clinical improvement should be noted after 2 weeks, and almost complete response can be expected after 4 weeks. The definition of response criteria was beyond the scope of this project; however, a definition of response was proposed in Dasgupta et al.3 ,4 8For initial GC tapering, we recommend reducing the oral dose gradually to a dose of 10 mg/day prednisone equivalent within 4–8 weeks; after relapse therapy the dose should be decreased gradually (within 4–8 weeks) to the dose at which the relapse occurred. For i.m. methylprednisolone, a dose of 120 mg every 3 weeks was used for the first 9 weeks in Dasgupta et al.23 No recommendation about dose adjustments of MTX can be made. 9The definition of criteria for remission and relapse was beyond the scope of this project. Definitions of remission and relapse used in clinical studies are summarised in Dejaco et al.65 10Once remission is achieved (following initial and relapse therapies), taper oral prednisone by 1 mg/4 weeks (or similar, eg, 2.5 mg/10 weeks) until discontinuation given that remission is maintained. In case i.m. methylprednisolone is used, the following tapering regimen was previously applied:23 100 mg methylprednisolone i.m. at week 12, then continuation of the injections at monthly intervals with the dose reduced by 20 mg every 12 weeks until week 48. Thereafter, the dose was reduced by 20 mg every 16 weeks until discontinuation. 11The group suggests that PMR patients be followed up every 4–8 weeks in the first year, every 8–12 weeks in the second year and as indicated in case of relapse or as prednisone is tapered off. 12No recommendation can be made for minimal/optimal duration of therapy. In case patients are treated with a combination of GCs plus MTX and GCs have been withdrawn already, discontinuation of MTX may be considered. 13Initial lack of response (eg, insufficient improvement of symptoms within 2 weeks): increase oral dose up to 25 mg prednisone equivalent. In case i.m. methylprednisolone is used, consider switching to oral GCs. Relapse therapy: increase dose to the previously effective (ie, pre-relapse) dose.
Recommendation 1: (PICO 1) The panel strongly recommends using GCs instead of NSAIDs in patients with PMR, with the exception of possible short-term use of NSAIDs and/or analgesics in PMR patients with pain related to other conditions (eg, co-existing osteoarthritis). No specific recommendation can be made for analgesics.
Explanation: The group recommends strongly against the use of NSAIDs compared to GCs in the treatment of PMR since the relative harm of long-term NSAID use (as mainly indicated by external evidence) outweighs the possible small benefits in PMR. No specific recommendation can be made for analgesics. On a basis of consensus, the panel recognised that the short-term use of NSAIDs and/or analgesics may be necessary in the setting of pain related to conditions other than PMR.
Recommendation 2: (PICO 2) The panel strongly recommends using the minimum effective individualised duration of GC therapy in PMR patients.
A more specific recommendation is not possible due to the lack of published evidence on this issue. On a basis of consensus and in accordance with the overarching principles, the group unanimously agreed to choose the minimum effective individualised duration and dose of GCs to balance benefit versus harm after assessing risk factors for GC-related adverse events, comorbidities, concomitant medications, relapses and prolonged therapy. Our recommended GC tapering schedule (see Recommendation 4) assumes a minimum of 12 months of treatment. A more specific statement is not possible because of the lack of PMR studies on this particular topic and because of the multiple subgroups and factors that need to be taken into account.
Recommendation 3: (PICOs 3–5) The panel conditionally recommends using the minimum effective GC dose within a range of 12.5–25 mg prednisone equivalent daily as the initial treatment of PMR. A higher initial prednisone dose within this range may be considered in patients with a high risk of relapse and low risk of adverse events, whereas in patients with relevant comorbidities (eg, diabetes, osteoporosis, glaucoma, etc) and other risk factors for GC-related side effects, a lower dose may be preferred. The panel discourages conditionally the use of initial doses ≤7.5 mg/day and strongly recommends against the use of initial doses >30 mg/day.
According to the SLR on prognostic factors and based on clinical experience, the group agreed upon the existence of various PMR subgroups that are characterised by different risks of relapse, prolonged GC therapy and/or GC-related adverse events as well as by various comorbidities and co-medications. As there are insufficient data to make evidence-based recommendations for all conceivable subgroups, and taking current clinical practice into account,28–30 the panel agreed upon the use of the minimum effective GC dose out of a range of 12.5–25 mg prednisone equivalent daily balancing benefits versus harms. The panel did not construct case vignettes as a possible aid for clinical practice; however, it is suggested that a higher initial prednisone dose (within the given range) may be used in patients with a high risk of relapse and low risk of adverse events, whereas in patients with relevant comorbidities (eg, diabetes, osteoporosis, glaucoma, etc) and other risk factors for GC-related side effects, a lower dose may be preferred.
The group conditionally discourages low (≤7.5 mg/day) and strongly recommends against high (>30 mg/day prednisone equivalent) initial GC doses. For this statement the group extrapolated the data from randomised controlled trials,29 ,31 and took clinical experience, national PMR guidelines,28–30 as well as current ACR and/or EULAR recommendations on the use of GCs in rheumatic diseases into account.32–35 In addition, there is incontrovertible external evidence of harm from long-term large doses of GCs32–35 and lack of evidence for any benefit of a high-dose regimen in PMR. It was unanimously agreed among the group that patients requiring high doses of GCs should be evaluated for alternate diagnoses and an alternate management plan.
Recommendation 4: (PICO 6) The panel strongly recommends individualising dose-tapering schedules, based on regular monitoring of patient disease activity, laboratory markers and adverse events.
The following principles of GC dose tapering are suggested:
Initial tapering: Taper dose to an oral dose of 10 mg/day prednisone equivalent within 4–8 weeks
Relapse therapy: Increase oral prednisone to the pre-relapse dose and decrease it gradually (within 4–8 weeks) to the dose at which the relapse occurred.
Tapering once remission is achieved (following initial and relapse therapies): Taper daily oral prednisone by 1 mg every 4 weeks (or by 1.25 mg decrements using schedules such as 10/7.5 mg on alternate days, etc) until discontinuation as long as remission is maintained.
In accordance with the overarching principles, the panel agreed upon a strong recommendation to individualise dose tapering and to regularly monitor PMR patients. Further, the panel proposed general principles for initial and post-relapse tapering of GCs (based on consensus and current clinical practice) but did not fix a schedule as in other guidelines.28–30 The panel agreed that equivalent objectives may be achieved by alternative tapering schedules. For example, a patient with a high initial prednisone dose (eg, 25 mg/day) may have a fast initial taper followed by a more gradual decrease in the GC dose, whereas in a patient starting at a lower initial dose (eg, 12.5 mg/day), the initial dose may be kept constant for longer and then eventually reduced.
The group suggested prednisone should be tapered by 1 mg/4 weeks or similar once remission is achieved. Again, the panel emphasised the important overall principle of gradual GC reduction without the need to prescribe a fixed schedule. The group further recognised that 1 mg prednisone tablets are not available in all countries (making a reduction of 1 mg/4 weeks unfeasible) and that other regimens such as alternate day reductions (eg, 10/7.5 mg on alternate days, etc) are common clinical practice.28
Recommendation 5: (PICO 7) The panel conditionally recommends considering intramuscular (i.m.) methylprednisolone as an alternative to oral GCs. The choice between oral GCs and i.m. methylprednisolone remains at the discretion of the treating physician.
In one clinical trial, i.m. methylprednisolone was applied at a dose of 120 mg every 3 weeks until week 9. At week 12, 100 mg were used and subsequently, injections were continued at monthly intervals and the dose was reduced by 20 mg every 12 weeks until week 48. Thereafter, the dose was reduced by 20 mg every 16 weeks until discontinuation.23 ,36
The panel did not specify a clinical phenotype where i.m. GCs would be appropriate or adequate therapy; however, the panel agreed that in clinical practice this preparation may be considered in cases where a lower cumulative GC dose is desirable, for example in female patients with difficult to control hypertension, diabetes, osteoporosis and/or glaucoma.37–39 Nonetheless, the panel acknowledged that there is a lack of convincing evidence showing significantly fewer side effects with i.m. methylprednisolone than with oral GC therapy.
The reasons why the panel did not endorse a strong recommendation for the use of i.m. methylprednisolone are the following: (1) the efficacy of i.m. methylprednisolone is supported by a single randomised controlled trial and confirmation of these data is still necessary;23 ,36 (2) this trial was neither designed nor powered as a non-inferiority trial and therefore, a difference between the efficacy of i.m. and oral GC cannot be excluded; (3) the trial failed to demonstrate a reduction in GC-related adverse events except for weight gain; (4) the long-term benefit of this preparation is unknown (particularly with respect to a possible reduction in GC side effects); and (5) i.m. methylprednisolone is not available in all countries.
Recommendation 6: (PICO 8) The panel conditionally recommends using a single rather than divided daily doses of oral GCs for the treatment of PMR, except for special situations such as prominent night pain while tapering GCs below the low-dose range (prednisone or equivalent <5 mg daily).
There are no studies available addressing this issue specifically in PMR. Based on clinical experience and because of the concern that adverse events (including disturbance of the hypothalamic–pituitary–adrenal axis) may be higher with divided doses, the group agreed against the general use of divided GC doses in PMR.40–43 The effectiveness and acceptability of a single daily GC dose has been standard clinical practice in PMR and other inflammatory conditions44 ,45 and evening doses can cause circadian rhythm and sleep disturbances.46
In special situations such as in case of night pain while tapering below the low-dose range (prednisone or equivalent <5 mg daily), split doses may be considered. However, persistent break-through symptoms should prompt re-consideration of the diagnosis.
Recommendation 7: (PICO 9) The panel conditionally recommends considering early introduction of MTX in addition to GCs, particularly in patients at high risk of relapse and/or prolonged therapy as well as in cases with risk factors, comorbidities and/or concomitant medications where GC-related adverse events are more likely to occur. MTX may also be considered during follow-up in patients with a relapse, without a significant response to GC or experiencing GC-related adverse events.
In clinical trials, MTX has been used at oral doses of 7.5–10 mg/week.24–27
Similar to the explanation of Recommendation 5, the panel felt that there is no clinical prototype unconditionally warranting treatment with MTX, rather the use of this drug should be discussed on an individual basis. In clinical practice, MTX may be considered for example in female patients36–39 ,47 with high initial erythrocyte sedimentation rate (ESR) (>40 mm/1st hour),48–53 peripheral inflammatory arthritis54 and/or comorbidities that may be exacerbated by GC therapy.
The panel also reached a consensus that MTX should be considered in patients who have relapsed (either on or off GCs), cases without significant response to GC or patients experiencing GC-related adverse events. The group further agreed that MTX may be used with oral or i.m. GC preparations even if the concomitant use of MTX and i.m. methylprednisolone has not been tested formally.
The efficacy of MTX was addressed in four randomised controlled trials and one retrospective study testing the use of MTX plus oral GCs (initial prednisone doses ranging from 15 to 25 mg/day).24–27 ,51 There was moderate to high quality of evidence (QoE) from studies indicating a benefit of MTX regarding remission (1 study),27 relapse rate (1 study),24 discontinuation of GC (1 study)24 and cumulative GC doses (3 studies).24 ,26 ,27 Evidence from one to four studies (1 related to remission, 4 to relapse, 1 to discontinuation of GC) indicating no benefit regarding these outcomes was of very low quality.25–27 ,51
The reasons why the panel did not support a stronger recommendation for the use of MTX in PMR are the following: (1) the total number of patients investigated in randomised trials was small (n=194),24–27 hence further confirmation of the present data is necessary; (2) results were contradictory in part, although trials with a negative result had a very low QoE; (3) a reduction in GC-related adverse events with the use of MTX has not been demonstrated. The power of the prospective studies to address this outcome, however, was insufficient. The panel nevertheless felt that earlier discontinuation of GC24 and a lower cumulative GC dose in MTX users26 ,27 decreases the likelihood of GC-related side effects; and (4) the cost-effectiveness of MTX use in PMR is not clear. More frequent prescriptions of MTX may lead to higher utilisation of healthcare resources in the short term (eg, because of specialist referral, monitoring visits, blood tests, etc) but may in the long term save costs by reducing GC-related side effects. Future studies are necessary to clarify this issue.
The group recognised that no recommendation can be made for the use of other non-biologic (ie, conventional synthetic and conventional targeted) DMARDs in PMR because of the lack of good evidence from PMR studies. Hydroxychloroquine was investigated by a single very low QoE retrospective study reporting no benefit regarding relapse rate.51
Recommendation 8: (PICOs 10–11) The panel strongly recommends against the use of TNFα blocking agents for the treatment of PMR.
The group agreed strongly against the use of TNFα blocking agents in PMR at this time since there is no evidence for benefit, but there is a considerable risk of potential harm and high resource use.55
No recommendation can be made for other biologic agents as no prospective trials have been published so far. There is one ongoing randomised study on the use of tocilizumab (clinicaltrials.gov NCT01396317) and another three-arm trial comparing secukinumab, canakinumab and GCs (clinicaltrials.gov NCT01364389) in PMR. The results of these studies may lead to a modification of this recommendation.
Recommendation 9: (PICO 12) The panel conditionally recommends considering an individualised exercise programme for PMR patients aimed at the maintenance of muscle mass and function, and reducing risk of falls.
There are no studies investigating the value of non-pharmacological therapies (eg, physiotherapy, relaxation techniques, diets, etc) in PMR and there is insufficient clinical experience on this issue to agree on a specific recommendation. Nevertheless, the panel agreed on recommending an individualised exercise programme (see overarching principles) in view of its benefit for maintaining muscle mass and function and reducing risk of falls, especially in older persons on long-term GCs as well as in frail patients.
Use of herbal preparations in PMR
The panel strongly recommends against the use of the Chinese herbal preparations Yanghe and Biqi capsules in PMR patients.
There were some discussions about whether herbal preparations could be considered non-pharmacological interventions (and were therefore within the scope of PICO 12); however, the panel felt the need for comment on this issue because several preparations are available which may be popular with PMR patients.
The SLR identified two studies testing Chinese Yanghe herb decoction and Chinese Biqi capsules in PMR patients.56 ,57 For Chinese Yanghe there is moderate QoE for a lower ESR at week 8 (mean difference 6.0 mm/h) and 12 (6.4 mm/h) and very low QoE indicating a lower rate of GC-related adverse events (with borderline significance of the effect estimate) as well as reduced morning stiffness at week 12.56 For Biqi capsules there is low QoE indicating a higher response rate at week 12.57
The group nevertheless agreed (after balancing evidence, benefit/harm, availability and resource use) to recommend strongly against the regular use of these preparations at this time for the following reasons: (1) the relevance of the small effect of Chinese Yanghe herb decoction on ESR is minimal for patients and good evidence for a clinical benefit of the substance is not available; (2) neither of the two substances is approved by the US Food and Drug Administration (FDA) or the European Medicines Agency (EMA); (3) the generalisability of the evidence for benefit is unclear; (4) these preparations may have unforeseeable adverse effects; (5) the availability of high quality preparations is unclear; and (6) resource impact (ie, costs) is unknown.
Release and implementation of the recommendations
See online supplementary file S2.
Cost implications and conflicts of interest
Cost implications are outside the scope of these recommendations.
None of the panel members disclosed any conflict of interest associated with the development of these recommendations.
Discussion
See online supplementary file S3 for a full-length discussion. The 2015 EULAR/ACR recommendations for the management of PMR is the first collaborative project between EULAR and ACR to endorse treatment recommendations in rheumatology.
We recognise that our recommendations are only partially supported by evidence, and that they do not cover all aspects important for the management of PMR. The group therefore unanimously agreed that the research agenda (covering the evidence gaps related to PMR management) is an important result of this project (box 2).
Research agenda
The group agreed that future studies in polymyalgia rheumatica (PMR) should be multicentre and properly powered using an agreed, validated core outcome set and a robust trial design that would maximise the power of studies, facilitate regulatory approvals and allow future meta-analysis.
Specific research questions:
Which outcome measures including patient-related outcomes, and response, remission and relapse criteria should be used in PMR? What is the value of a composite score? What are the most relevant treatment targets in PMR?
What is the efficacy and safety of different routes of glucocorticoid (GC) administration (oral, intramuscular, intra-articular), different initial GC doses, various GC tapering regimens, and different GC flare doses?
What is the efficacy and safety of DMARDs (non-TNFα biologic, conventional synthetic and conventional targeted) in PMR? What is the optimal strategy for using DMARDs in PMR: monotherapy versus combination therapy, early versus late introduction, and (particularly for biologics) use with or without GCs?
What is the minimal/optimal duration of therapy and which strategies for withdrawing GCs and/or DMARDs yield the best efficacy/safety profile?
What is the optimal strategy for shared primary and specialty care including recommendations for specialist referral? How can patients be better involved in treatment decisions, and are there any decision aids? What is the role of self-management?
What is the value of tight control (ie, treat to target) versus conventional management strategies in PMR?
How should patients with long-standing disease and long-term low-dose GC therapy be managed?
What is the cost utility and effectiveness of DMARD use in PMR (versus GC use alone)?
What is the value of non-pharmacological therapies in PMR? Particularly, it is assumed but not yet demonstrated that physiotherapy may support preservation of function and reduce the risk of adverse events related to GC use. Patients may benefit from exercise by maintaining muscle mass and function as well as by fall prevention especially in the frail. What is the role of diet in PMR and nutrition supplements (eg, fish oil) related to outcomes?
What is the efficacy and safety of herbal preparations in PMR?
What is the role of imaging (particularly ultrasound) for the assessment and monitoring of PMR, identification of overlap with other diseases (eg, large vessel vasculitis or inflammatory arthritis) alongside clinical and patient reported outcomes?
Which biomarkers may be useful in PMR? Why do some patients do better than others? How can we identify these groups and what is the biological mechanism behind it? Should different drugs be applied to different PMR subgroups?
What is the morbidity and mortality of PMR patients (with a particular focus on cardiovascular risk) in long-term observational studies?
What is the aetiopathogenesis of PMR? Which targeted therapies could be developed based on new knowledge of disease mechanisms?
Bolded points indicate the top 5 items of the research agenda according to the opinion of the guideline panel.
Due to our rigorous SLR approach to select high quality papers, we did not include other reviews, case reports or case series indicating possible treatment options in treatment-resistant PMR patients. For example, we found one earlier SLR reporting similar conclusions regarding the value of MTX in PMR.58 In addition, two case series were recently published on the use of leflunomide59 ,60 and a few case reports are available on tocilizumab.61–63 Azathioprine has been tested in a double-blind randomised controlled trial in patients with PMR and GCA; however, as PMR patients were not analysed separately, we did not include this study in the SLR.64
It was beyond the scope of this recommendation project to define treatment targets in PMR. ‘Clinical improvement’ was considered as the first treatment goal after the initiation of GCs, and the response criteria used in the 2012 classification criteria study may be considered.3 ,4 Remission and relapse have been heterogeneously defined in the literature, as we pointed out previously.65 Future prospective studies aimed at the validation of new definitions of response, remission and relapse are, therefore, required to enable a targeted treatment approach in PMR.66
The most important limitations of this project are the paucity of high quality trials (as mentioned above) and the fact that GRADE is less well developed for the assessment of rare outcomes. Consequently, the QoE for adverse events is usually lower than for efficacy data. This necessitated the use of relevant external evidence to strengthen this aspect of our recommendations.
These recommendations should support clinicians to achieve the best patient outcomes. Further research on existing drugs is necessary to offer additional, evidence-based treatment options to our patients. We anticipate an update of these recommendations 3 years after their publication; however, an earlier revision may be necessary if new data emerge that would modify the current recommendations.
Acknowledgments
We thank Catherine Wardle from Southend library for her assistance retrieving full text articles.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online Methods
- Data supplement 2 - Online Results
- Data supplement 3 - Online Discussion
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
ELM and BD are co-senior authors.
This article is published simultaneously in the October 2015 issue of Arthritis & Rheumatology.
Supported by the American College of Rheumatology and the European League Against Rheumatism.
Twitter Follow Sarah Mackie at @Sarah_L_Mackie and Andreas P Diamantopoulos at @adiamanteas
Contributors All authors contributed to conception and design of the study, acquisition and/or interpretation of data, drafting the article or revising it critically for important intellectual content, and approved the final version of the manuscript. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was supported by research grants from the American College of Rheumatology and the European League Against Rheumatism.
Competing interests All the participants of this project made a disclosure of possible conflicts of interest. The individual declarations are available on demand at the American College of Rheumatology secretariat and are summarised below as remuneration for consultation and/or speaking engagements (‘R’) or industry-related research funding (‘F’). AB—R: MEDAC, Abbott, ENEL-MED, Wyeth, Lilly; F: Wyeth, Lilly; PB—R: Pfizer, Csont Dg (Military Medical Institute Warsaw), Sonosite, APLAR, Abbott; F: Abbott, BMS; FB—R: Merck Serono, Horizon Pharma (formerly Nitec Pharma), Mundipharma International Ltd; F: Merck Serono, Horizon Pharma; SC—R: Centocor; MCid—R: Centocor, Roche, BMS; F: Marato TV3 (private foundation); MCim—R: Roche, BMS, Menarini; F: Roche; BD—R: Merck; F: Roche, Mundipharma, Servier; CDe—R: BMS, Pfizer, AbbVie, MSD, Merck Serono, Roche; F: Pfizer, MSD; CDu—R: BMS, Pfizer, AbbVie, MSD, Merck Serono, Roche; DJ—R, F: Roche/Genentech; SMa—R: Pfizer, Napp Pharmaceuticals, AstraZeneca; AM—R: AstraZeneka, Pfizer; VM-T—R: UCB-Pharma, Pfizer, UCB Pharma, Cellerix, Abbott; F: Roche; ELM—F: Ardea, Sanofi, Centocor-Jansen, Celgene, Amgen, Roche, Genentech, Mesoblast, Novartis, Pfizer, UCB Pharma; SMo—F: Bristol-Myers Squibb; CS—R: Novartis; MS—R: Abbott, Pfizer, Amgen, GSK, MSD; WS—R: Berlin-Chemie, Medac, Pfizer, AbbVie, Roche, Mundipharma, UCB, MSD; F: Mundipharma, Novartis, MJD, Actelion, GE, Esadie, Savient; RS—F: funded research by Roche-Genetech.
Provenance and peer review Not commissioned; externally peer reviewed.