Article Text

Abstract
Objective: To assess the efficacy of anti-tumour necrosis factor (TNF) therapy to induce remission in patients with Takayasu arteritis (TAK) refractory to other immunosuppressive therapies.
Methods: Retrospective single-centre study of 25 patients with refractory TAK.
Results: Patients were treated with infliximab (IFX) or etanercept (ETA) for up to 7 years; 21 with IFX (median 28 months (range 2–84)) and 9 with ETA (median 28 months (range 4–82)); 5 patients initially treated with ETA subsequently switched to IFX. Following anti-TNF therapy, remission was achieved and prednisone was discontinued in 15 patients (60%) and successfully tapered below 10 mg/day in an additional 7 patients (28%). Of 18 patients treated with other immunosuppressive agents concurrent with anti-TNF therapy, 9 (50%) could taper or discontinue the additional agent. Major relapses occurred in four patients that initially achieved stable remission. Four patients suffered adverse events, including one with opportunistic infections and one with breast cancer.
Conclusions: In this group of patients with refractory TAK, anti-TNF therapy was associated with remission in a majority of patients, facilitating dose reduction or discontinuation of prednisone and other immunosuppressive therapy. These findings strengthen the rationale for the conducting of a randomised controlled trial of anti-TNF therapy in TAK.
Statistics from Altmetric.com
Takayasu arteritis (TAK) is an idiopathic, granulomatous vasculitis with a predilection for the aorta and its major branches. Vessel inflammation may result in segmental stenosis, occlusion, dilatation and/or aneurysm formation. While up to 20% of patients with TAK have a monophasic illness, most have a relapsing/remitting course, typically requiring prolonged treatment with glucocorticoids and additional immunosuppressive agents, such as methotrexate. However, only a minority of patients achieve sufficient disease control on these therapies to allow successful taper or discontinuation of glucocorticoids.1 2
There is increasing evidence to suggest that tumour necrosis factor (TNF)α may be an attractive therapeutic target in TAK. Firstly, TAK is characterised by granulomatous inflammation and TNFα plays a central role in granuloma formation.3 Secondly, it has been demonstrated that TNFα is upregulated in peripheral blood mononuclear cells4 and increased serum TNFα concentrations5 occur in patients with TAK, compared to healthy controls, and CD3+ T cells from patients with active disease have higher TNFα production than noted in patients in remission or in healthy controls.6 Lastly, in preliminary studies, anti-TNF therapy has been successfully employed in patients with TAK refractory to other immunosuppressive therapies.7 A prior study of 15 patients with relapsing TAK, reported encouraging results over a median follow-up time of 12 months after initiation of anti-TNF therapy. Several case reports have since noted similar results with anti-TNF therapy.8–11 The objective of the current study was to extend these previous observations by reporting the outcome of anti-TNF therapy in a larger number of refractory patients with TAK followed for a longer period.
PATIENTS AND METHODS
Study patients
This retrospective study was intended to assess the utility of anti-TNF therapy in facilitating remission induction, glucocorticoid tapering and a reduction in relapse rate and to evaluate toxicity associated with anti-TNF therapy in patients with refractory TAK in whom repeated prior relapses occurred following gradual taper of glucocorticoid therapy. Patients received their care at a single referral centre. All patients met American College of Rheumatology (ACR) classification criteria for TAK. Patients were considered to have “refractory TAK” if stable remission could not be achieved with use of low-dose prednisone (less than 10 mg/day) despite an adequate trial of at least one additional immunosuppressive agent (see table 1). Anti-TNF treatment schedules were as previously described.7
Data collection
Cases were identified from the records of the Cleveland Clinic, Cleveland, Ohio, USA. Approval for the retrospective chart review was obtained from the Cleveland Clinic Institutional Review Board. Information on symptoms, clinical findings and results of laboratory testing and serial magnetic resonance (MR) imaging was extracted from a standardised electronic medical record database for TAK that is a component of care for the Cleveland Clinic vasculitis program. All patients were seen by at least one of the study authors at each clinic visit. Data was collated using Microsoft Excel (Microsoft, Redmond, Washington, USA) and analysed with JMP statistical software (SAS, Cary, North Carolina, USA).
Study outcomes
The primary outcome of interest in this study was the achievement of partial or complete remission; secondary outcomes included the occurrence of disease relapse and adverse events associated with anti-TNF therapy. The definitions of remission and relapse for the purpose of this study were based on the method of assessment of disease activity, as previously described.7 Relapses were considered as major or minor depending on the presence or absence, respectively, of new lesions in new arterial territories on vascular imaging (performed at least every 6 months) that resulted in abnormal calibre of the vessel wall (ie, occlusion, stenosis or aneurysm).
RESULTS
Patient characteristics
In total, 28 patients with TAK received anti-TNF therapy; 3 patients were excluded because of insufficient follow-up data. No patient was in remission at the time of initiation of anti-TNF therapy; 13 had not achieved remission at any time since initial diagnosis. Patients were treated with anti-TNF therapy for up to 7 years; 21 were treated with IFX with a median follow-up of 28 months (range 2–84) and 9 patients were treated with ETA, with a median follow-up of 28 months (range 4–82). Five patients received both agents; all five were initially treated with ETA and subsequently switched to IFX. No patients were treated with adalimumab.
All but three of the patients were female. Mean age was 35 years (range 15–64). Mean age at onset of TAK was 25 years (range 10–53) and median disease duration was 116 months (range 39–344). In total, 20 patients were Caucasian, 4 were Asian and 1 was Hispanic. All patients were treated with prednisone and a mean of two additional immunosuppressive agents prior to commencement of anti-TNF therapy (range 0–6, see table 1).
Clinical response
Outcomes of ETA therapy are summarised in fig 1. Two patients that continued on ETA after achieving complete remission have discontinued prednisone; one also discontinued methotrexate. Of the two patients that were switched to IFX despite initially achieving complete remission with ETA, one switched to IFX at 28 months due to unavailability of ETA and subsequently had a sustained remission. The other patient had a number of minor disease flares requiring increased dose of prednisone and of ETA, was switched to IFX due to a major disease flare at 67 months, but relapsed after two infusions and IFX was subsequently stopped. All three of the initial non-responders to ETA subsequently achieved complete remission with IFX. Of the three patients that initially entered remission with ETA, but subsequently stopped ETA either permanently or temporarily (without immediately commencing IFX), all three had a disease flare within 1–2 months.

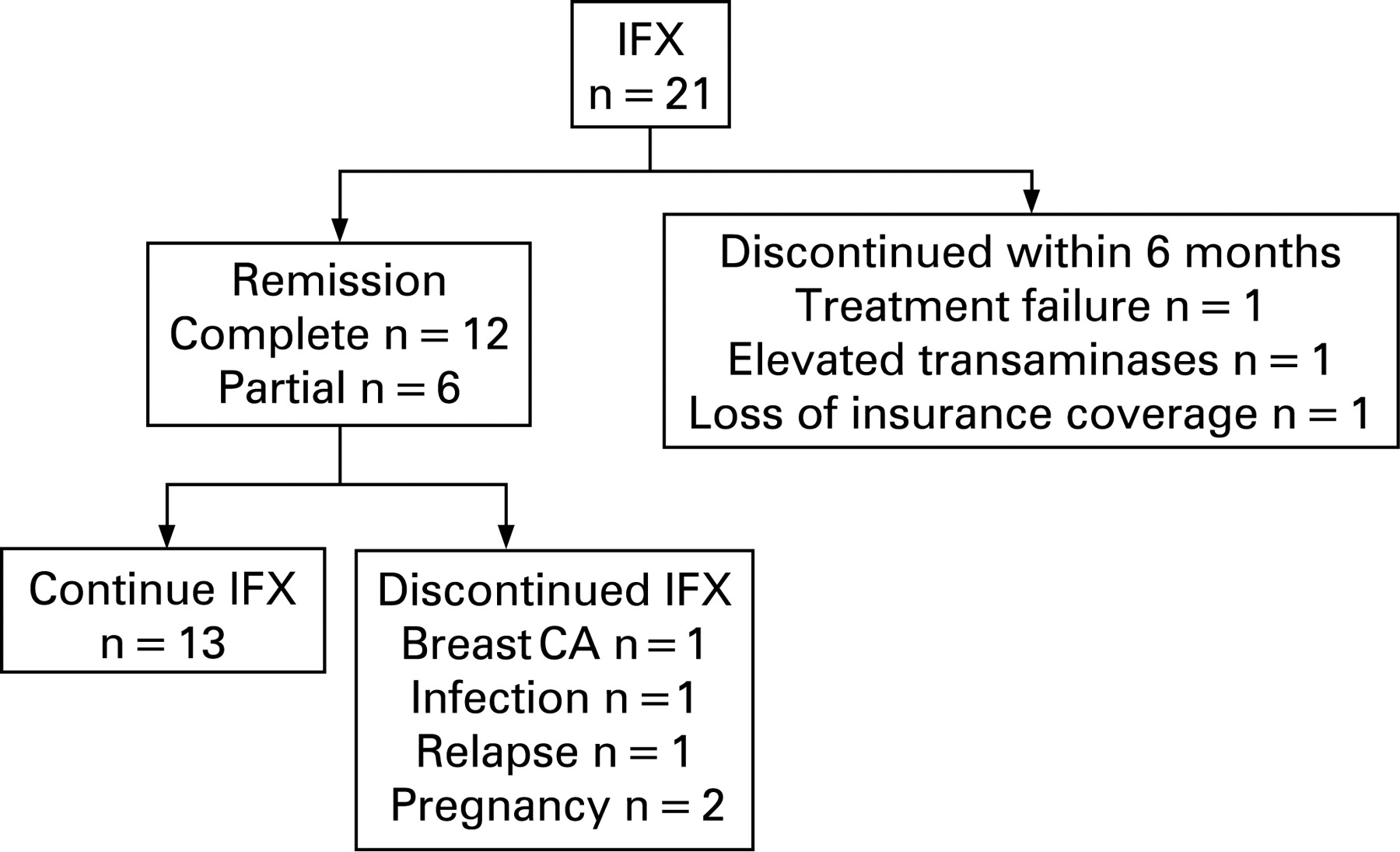
Outcomes of IFX therapy are summarised in fig 2. Median stable IFX dose was 5 mg/kg (range 4–10 mg/kg), administered at a median interval of 6 weekly (range 4–8 weekly). Of the nine patients that either permanently or temporarily discontinued IFX, eight had a disease flare at a median interval of 5 months (range 2–12); two of these patients restarted IFX treatment and again achieved remission.

{kind=link}
{kind=link}
Overall, prednisone was discontinued in 15/25 patients (60%) and tapered below 10 mg/day in an additional 7/25 (28%). Median prednisone doses before and after anti-TNF therapy were 19 mg (range 5–50) and 0 mg (range 0–30), respectively. Of the 15 patients that entered complete remission with anti-TNF therapy, prednisone (median dose 20 mg/day, range 5–30) was discontinued after a median interval of 10 months (range 0–72), and prednisone-free remission has been subsequently maintained for a median duration of 30 months (range 6–82). Of 18 patients treated with other immunosuppressive agents concurrent with anti-TNF therapy, 9 (50%) were able to taper (n = 5) or discontinue (n = 4) these additional immunosuppressive agents.
Relapse during anti-TNF therapy
Relapses were experienced by three of the six patients that initially achieved remission on ETA. Two of these patients regained disease control with an increase in dose of ETA to 50 mg twice weekly; one also required addition of prednisone. Of the 18 patients that initially achieved remission with IFX, 12 had relapses. In six patients, minor relapses were treated with either increased dose or reduced dosing interval of IFX alone, without addition of prednisone or other therapy. Four patients with minor relapses required prednisone treatment in addition to adjustment of the IFX treatment protocol.
Four patients had a major disease relapse while on anti-TNF therapy (two IFX, two ETA). Of these, all four had concurrent clinical features of active disease and three had abnormalities of acute phase reactants. In all four of these patients, new stenotic lesions developed in previously uninvolved vascular territories. One patient developed coronary stenosis during a period of poor compliance with ETA, another acquired common hepatic and splenic artery stenoses after tapering methotrexate after initial remission with IFX. Another patient on IFX sustained a major relapse during an interruption of therapy because of loss of insurance coverage. Three of the four patients subsequently achieved sustained remission on higher doses of anti-TNF therapy.
Adverse events
One patient discontinued ETA due to nausea, diarrhoea and hypertension, another temporarily discontinued ETA because of a viral illness. Whether these adverse events were due to ETA was uncertain. The adverse events necessitating discontinuation of IFX were abnormal liver function tests in one patient, primary histoplasmosis after two infusions in a patient that travelled to an endemic region and breast cancer in a 52-year-old woman after 41 months of IFX therapy. These events were judged to possibly be related to IFX.
DISCUSSION
The results of this study extend our prior findings and those of subsequently published case reports,7–11 and suggest that anti-TNF therapy may lead to durable remission or improvement with lower glucocorticoid requirements in most patients with TAK refractory to other immunosuppressive therapies. However, it is clear that anti-TNF therapy merely controls rather than cures TAK. Most patients who discontinued anti-TNF therapy, either temporarily or permanently, relapsed within months. Many patients required dose escalation of anti-TNF therapy. This study echoes the findings of previous studies demonstrating that for many patients, TAK is a chronic, relapsing disease,1 2 and that the concept of TAK as a monophasic illness should be regarded as the exception rather than the rule.
Key limitations of this study include the retrospective nature of the analysis, the small numbers of patients and the lack of a control group. While three of four patients that suboptimally responded to ETA were subsequently able to achieve sustained remission with IFX, the small number of patients involved precludes definitive assessment of the relative efficacy of IFX and ETA.
In conclusion, this study suggests that anti-TNF therapy may lead to durable remission and reduction in glucocorticoid requirements in most patients with refractory TAK. However, this study also provides a reminder of the possible toxicities of anti-TNF therapy. A randomised controlled trial is required to substantiate the findings of this study.
REFERENCES
Footnotes
Funding: ESM is funded by the Vasculitis Foundation, RJ Fasenmeyer Center for Clinical Immunology and the Cleveland Clinic Center for Vasculitis Care and Research.
Competing interests: None.
Ethics approval: Ethics approval was obtained from the Cleveland Clinic Institutional Review Board.