Article Text

Abstract
Objective: To study the prevalence of orthopaedic surgery and to evaluate possible predictive factors for large joint replacements in patients with early rheumatoid arthritis (RA).
Patients and methods: A cohort of 183 patients (116 (63.4%) female) with early RA was monitored for 16–20 years after recruitment during 1985–9. Mean (SD) age of patients 51.4 (12.4) years; mean (SD) duration of symptoms before inclusion 12 (7) months and mean (SD) duration of follow-up 16 (4) years. Occurrence of orthopaedic surgery was recorded continuously. A first prosthesis of a large joint (shoulder, elbow, wrist, hip, knee or ankle) was used as outcome variable in the predictive analyses.
Results: In total, 386 orthopaedic interventions were performed in 106/183 (58%) patients during follow-up and a large joint replacement was performed in 44/183 (24%) patients. Using a Cox regression model, it was shown that Health Assessment Questionnaire, C-reactive protein and erythrocyte sedimentation rate at inclusion, and radiographic changes in small joints after 1 year, were associated with an increased risk of receiving prosthesis of large joints.
Conclusion: In this cohort of patients with RA monitored from early disease stage, orthopaedic surgical procedures were performed in more than half of the patients. This included first large joint replacements in 24% of the cases. Easily available measures were identified as predictors of such joint replacements. This study could serve as a reference for comparison with cohorts of patients with RA recruited today, in which new more efficacious treatments are used.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory disease which leads to varying degrees of functional impairment and disability. The main goals of treatment in arthritis are to reduce the symptoms of inflammation and to prevent joint destruction and disability.1 Early and aggressive usage of disease-modifying antirheumatic drugs (DMARDs ) has been shown to improve long-term outcome in RA.2–4 Furthermore, treatment with biological agents in combination with conventional DMARDs, mostly methotrexate, has been shown to be efficacious in reducing signs and symptoms of RA and in particular in reducing the development of joint damage.5–8
Orthopaedic surgery is an important component in the management of RA. Despite improvements in pharmacological treatment a substantial proportion of patients still need a total joint replacement or other orthopaedic surgery. Previous studies have shown diverging rates of orthopaedic interventions. In a population-based incidence cohort of patients with RA in Rochester, Minnesota, a cumulative incidence for all joint surgery at 30 years was found to be 33.7%. Total joint replacements constituted 17.8% of the surgical interventions.9 Wolfe and Zwillich reported that 33.8% of patients with RA enrolled in a 23-year prospective study underwent some kind of joint surgery, of which 25% were total joint replacements.10 Similar figures for patients included in the Utrecht RA cohort from 1990 until 1998 were 27%, and 10%, respectively.11 Twenty-seven per cent of patients participating in a Finish 25-year follow-up study started in 1973, received prosthesis in at least one large joint.12 In a British inception cohort including patients with early RA followed up for 5 years, orthopaedic interventions were performed in 17% of the patients and 7% of patients needed large joint replacements.13
Large joint replacement is almost exclusively performed in cases of severe joint damage and thereby reflects an unsatisfactory course of disease. It is therefore important to search for predictive factors for this serious outcome. Two previous studies have shown that variables indicated disease activity and severity such as low haemoglobin levels, erythrocyte sedimentation rate (ESR), Health Assessment Questionnaire (HAQ) and early radiographic changes predicted future total joint replacement.10 13
A first objective of this study was to examine the occurrence of orthopaedic surgery associated with rheumatic disease in patients with RA recruited in 1985–9 early after disease onset and prospectively monitored for 16–20 years after diagnosis. A second objective was to identify possible predictive factors for future total large joint replacement surgery (shoulder, elbow, wrist, hip, knee and ankle).
METHODS
The study group comprised patients with recent onset RA taking part in a longitudinal study initiated in Lund 1985 (Lund early RA cohort).14 The baseline characteristics, clinical and laboratory assessments and also follow-up details have been described in previous reports.15 Briefly, 183 patients with early RA symptoms were included between 1985 and 1989. There were 116 (63.4%) women. Mean (SD) age was 51.4 (12.4) years and mean (SD) duration of symptoms before inclusion was 12 (7) months All patients fulfilled the 1958 American Rheumatism Association diagnostic criteria for RA.16 The patients were monitored annually including clinical and laboratory measures. Disability was evaluated using the validated Swedish version of the HAQ score.17 A visual analogue scale (100 mm) was used for patients’ estimation of their pain. Radiographs of hands and feet were taken yearly for the first 5 years and thereafter every 5 years and scored by the Larsen method.18 The presence of shared epitopes was analysed using PCR as previously described.19 Rheumatoid factors (IgM, IgG and IgA isotypes) were analysed with ELISA using commercial kits (Inova Diagnostics, San Diego, California, USA) as previously described. Levels >6 were considered to be positive.15 Anti-cyclic citrullinated peptide 2 (anti-CCP-2) was determined with ELISA using a commercial kit (Inova Diagnostics). The cut-off point for a positive result was ⩾20.15
Recruitment of patients in this cohort took place between 1985 and 1989 and the approach to pharmacological treatment was conservative compared with current treatment strategies in early RA. No patient had received DMARDs before inclusion. Throughout the study patients with active disease were offered treatment with such drugs. d-Penicillamine and antimalarial drugs were most commonly used in the early years and subsequently methotrexate became the most commonly used DMARD.
During the whole study period a close collaboration with the department of orthopaedic surgery in Lund was maintained and the patients were assessed for their need for surgery by mainly the same surgeons. All surgical interventions associated with RA were continuously recorded from inclusion until 31 December 2005. Also, all medical records were retrospectively reviewed in order to complete any missing data. Only the first total joint replacement surgery of a large joint (shoulder, elbow, wrist, hip, knee and ankle) as a consequence of RA was used as an outcome variable in this study. Large joint replacement surgery performed owing to pathology other than RA—for example, osteoporosis, osteoarthritis or trauma, was not included in the regression analysis.
Statistical analysis
Distribution of continuous variables was calculated as mean (SD) {range}. Differences between groups were analysed using the Mann–Whitney U test or χ2 test when appropriate. Since the follow-up time differed for individual patients the time-dependent Cox regression model was applied to identify possible predictive factors for the first large joint replacement surgery. For patients not monitored until December 2005, the date of the last follow-up visit or death was used. Owing to a high correlation factor between C-reactive protein (CRP) and ESR at inclusion (Spearman’s correlation rs = 0.685) the statistical analysis was done separately for these variables. Furthermore, two separate multivariate Cox regression models were performed owing to high correlation between CRP and the Larsen score at year 1 (rs = 0.416) and CRP and HAQ at inclusion (rs = 0.476). and Survival until the first event was determined using Kaplan–Meier curves for tertiles of CRP and HAQ. A p value <0.05 was considered significant.
RESULTS
In total, 116 of 183 patients from the cohort were followed up until 31 December 2005. Fifty eight (31.7%) patients died during the follow-up and 12 patients left the study owing to their high age, moving from the area or for other personal reasons. The mean (SD) follow-up duration of all patients included in this study was 16 (4) years. Forty-two patients (23%) were followed up for 19–20 years.
Throughout the study, 106 (58%) patients underwent at least one orthopaedic intervention associated with RA. The corresponding numbers of patients with a history of a minimum of two, three or four operations or more were 79 (43%), 51 (28%) and 41 (22%), respectively. A maximum of 24 surgical interventions directly related to RA was registered in one patient.
Altogether, 386 orthopaedic interventions were performed. Synovectomies of shoulder, elbow, wrist and finger joints, followed by tendon transfer surgery and surgery of the forefoot were most frequently done. Table 1 summarises the type and number (%) of surgical interventions.
In total, 44/183 patients (24%) underwent primary large joint replacement surgery. The hip joint was most often replaced, followed by the knee joint. Table 2 shows numbers (%) and type of these interventions. Altogether, 20/44 (45%) patients with a history of an arthroplasty underwent an additional arthroplasty of a large joint. Eleven patients underwent three or more large joint arthroplasties. No partial joint arthroplasty was performed in this cohort.
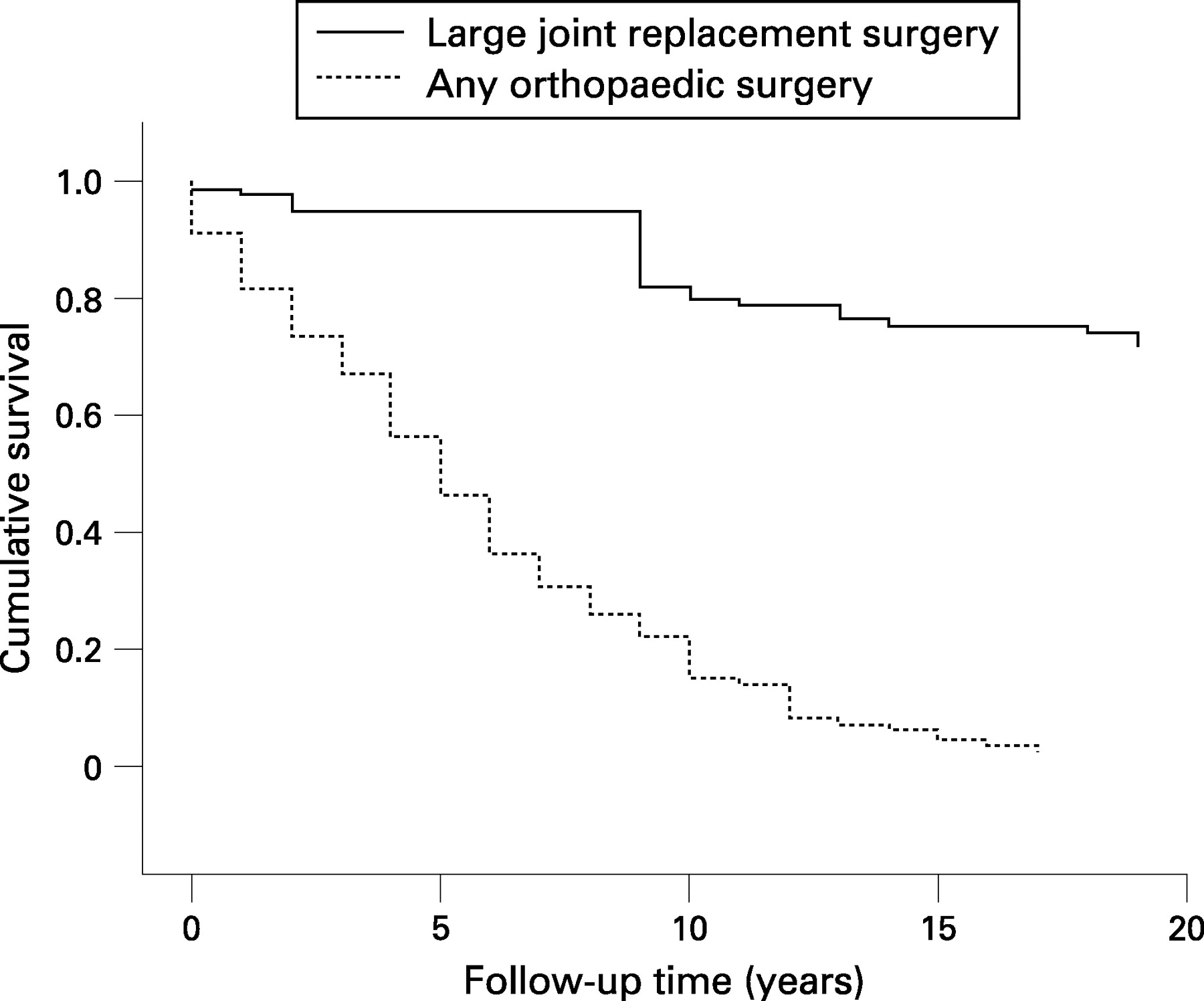
Figure 1 shows cumulative survivals (Kaplan–Meier curves) until the first orthopaedic surgery and the first large joint replacement surgery.

Table 3 shows the demographic and disease characteristics and treatment characteristics at year 1 and last follow-up visit in patients who subsequently underwent large joint replacement surgery and in patients without a history of such surgery.
There were no significant differences in age, gender, duration of symptoms before diagnosis or follow-up duration between the groups. The patients with history of large joint replacement had significantly higher levels of CRP and ESR and tended to have higher HAQ score at inclusion (p = 0.07). Larsen score at inclusion did not differ between the groups but Larsen scores at both year 1 and 2 were significantly higher in patients with a history of large joint replacement.
The presence of one copy of shared epitope did not differ between the groups but there was a tendency for patients subsequently receiving a large joint prosthesis to have double copies of shared epitope (p = 0.06). The presence of rheumatoid factors (RFs) (any isotype) and anti-CCP antibodies at inclusion was similar in the two groups.
Both oral prednisolone and DMARDs were more frequently used in the group of patients with a history of large joint replacement at year 1. However, a similar proportion of patients in both groups was treated with methotrexate, other DMARDs, oral prednisolone or biological agents at the last follow-up. Mean disease duration at initiation of the first biological treatment was not significantly different in patients with a history of large joint replacement from those without history of such surgery. A comparison between different biological agents was not performed owing to the limited number of treatments.
Since the patients were followed up for different time periods, further analysis of possible predictive factors was performed using multivariate Cox regression models. Table 4 presents the results of these analyses.
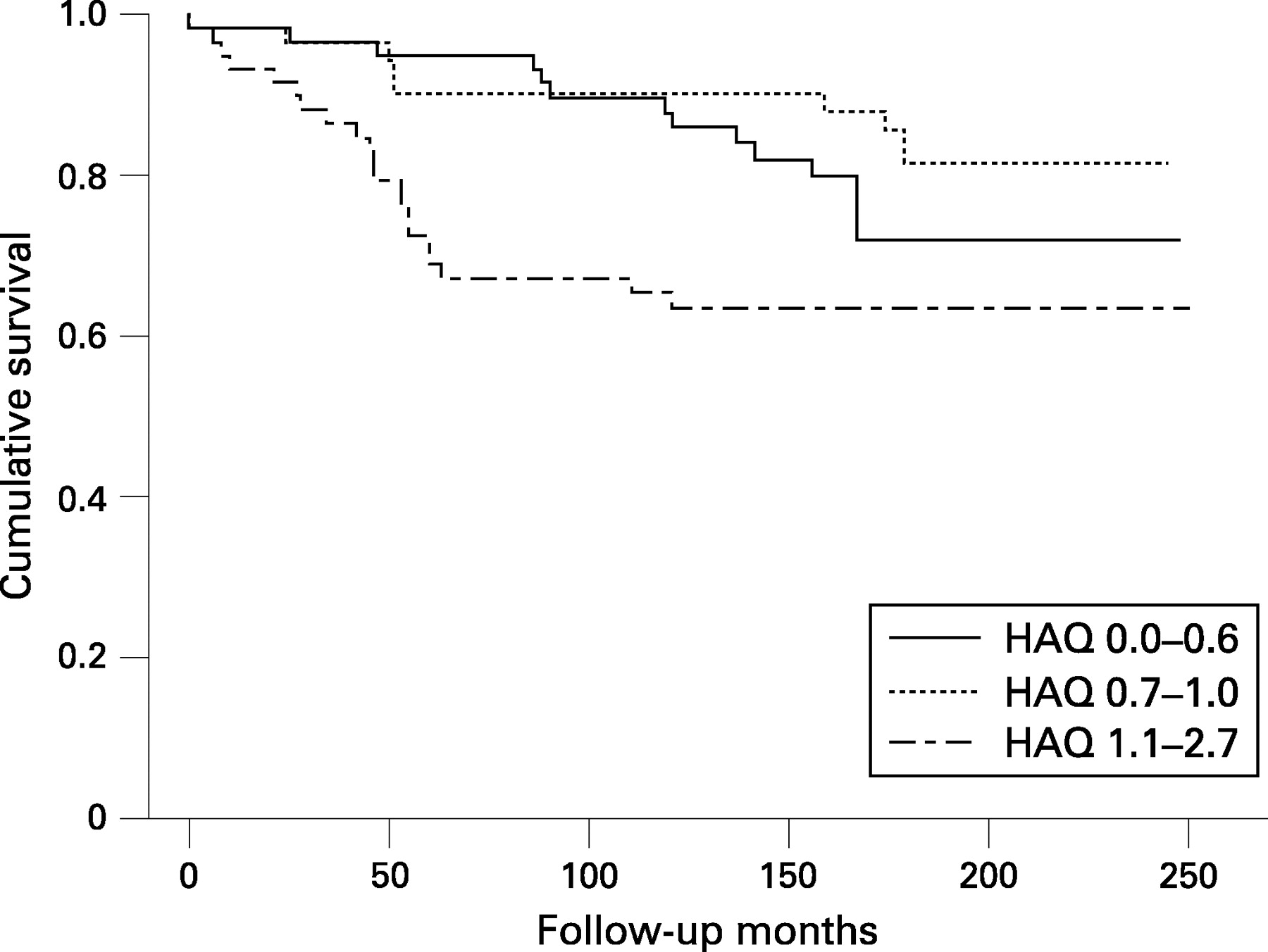
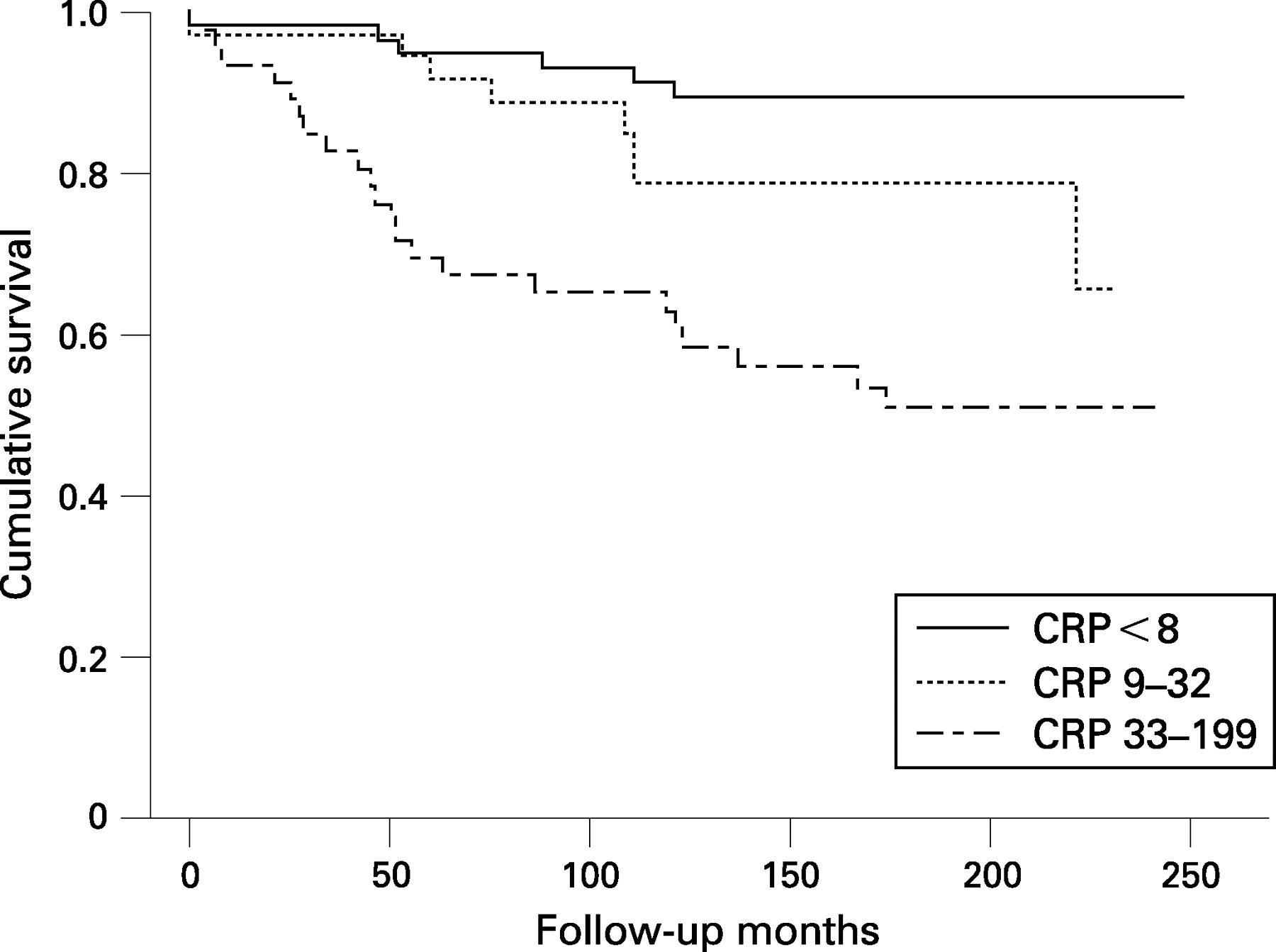
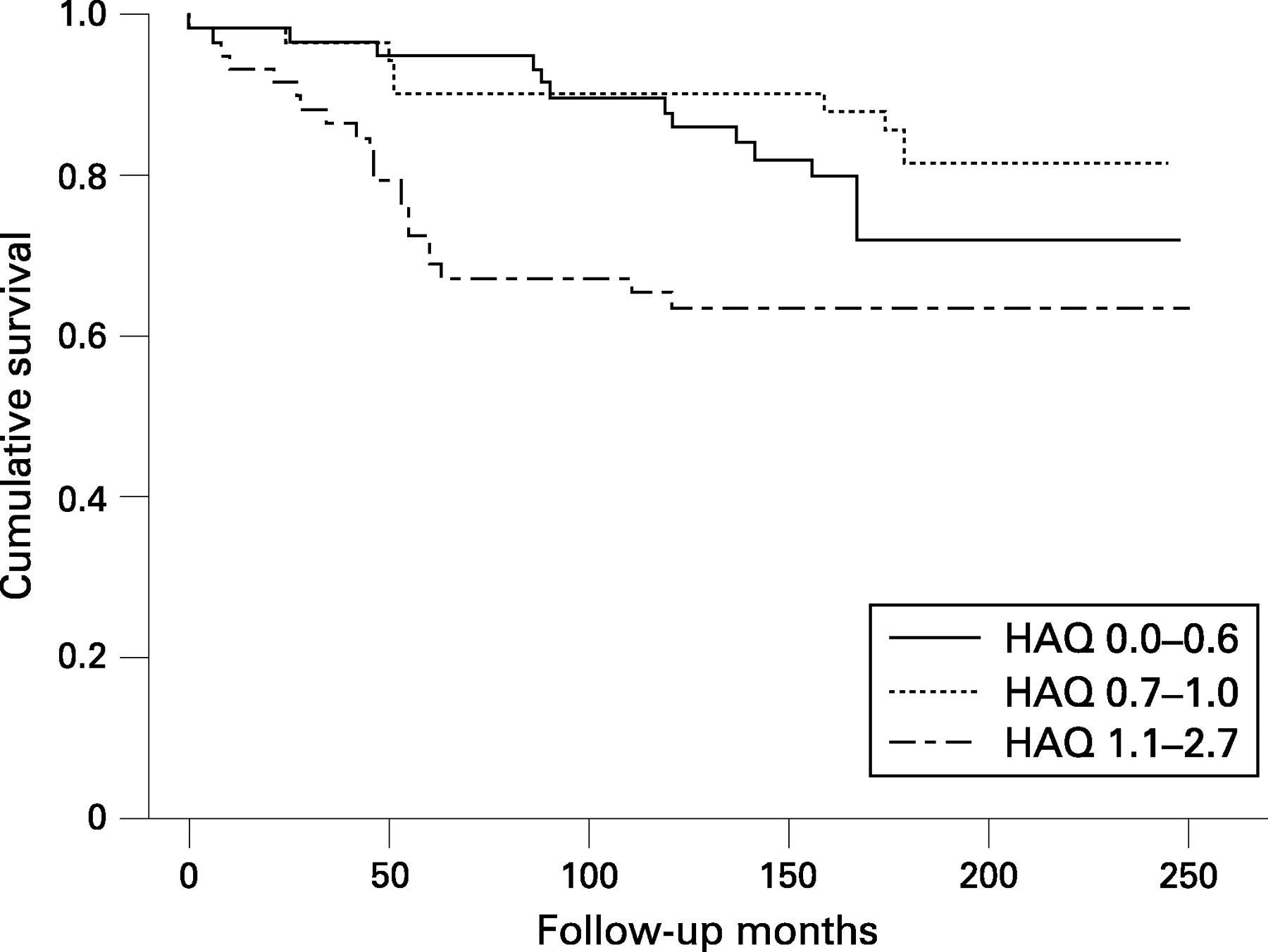
The Larsen score at year 1 and simple clinical measures such as CRP or, alternatively, ESR and HAQ scores at inclusion, were identified as positive predictive factors for subsequent large joint replacements in the regression models. Figures 2 and 3 show the impact of different levels of CRP levels or HAQ scores on survival to the first orthopaedic intervention. Patients having high CRP level (third tertile—ie, ⩾33 mg/l) had significantly shorter survival to the first event than those with lower CRP levels (first and intermediate tertile—ie, <33 mg/l) (p<0.001; log-rank test) (fig 2). The survival to the first event was significantly shorter in patients with high baseline levels of HAQ (third tertile—ie, ⩾1.1) than in those with lower levels (first and intermediate tertile —ie, 0–1.0) (p = 0.006, log-rank test) (fig 3).

{kind=link}
{kind=link}
{kind=link}
Patients carrying two copies of shared epitope tended to have an increase risk of large joint prosthesis, also after adjustment for differences in age at inclusion and gender in the Cox regression model ((p = 0.063; OR = 1.8; 95% CI 0.97 to 3.33). However, anti-CCP positivity was not found to be associated with increased risk of such surgery ((p = 0.557; HR = 1.28; 95% CI 0.561 to 2.922); univariate regression analysis).
DISCUSSION
More than half of the patients (58%) in this cohort of patients with RA needed at least one orthopaedic intervention and about one quarter (24%) underwent at least one large joint replacement during the mean follow-up of 16 years. A main finding was that simple clinical measures such as CRP or ESR and HAQ at inclusion and early radiological changes were identified as predictors of future need of large joint replacements.
The prevalence of all kinds of orthopaedic surgery as a consequence of RA is higher in this study than previously reported.9–11 All our patients had short duration of symptoms and were recruited at diagnosis. Differences in follow-up time and disease duration at study initiation might contribute to the divergent results. An additional explanation may be that indications for orthopaedic surgery or availability of orthopaedic surgery, or both, may vary between the countries. The current study is a single-centre study including outpatients at a university centre where early assessment by orthopaedic surgeons with a special focus on rheumatic conditions was part of the follow-up programme.15 It may be speculated that this has increased the likelihood of surgical interventions.
In our cohort, large joint replacements were performed in almost one quarter of patients (24%). A confounder might be that orthopaedic surgery in some patients was performed for pathologies other than RA—for example, osteoporosis, osteoarthritis or trauma. However, the majority of patients who had undergone large joint surgery in our study subsequently underwent one or more additional orthopaedic interventions as a consequence of RA. This supports the statement that the predominant pathology was RA.
The occurrence of large joint replacement surgery found in our study is in accordance with previous investigations with comparable follow-up time.10 12 Hip joint replacements were the most commonly performed replacements in our cohort (52%). Similar rates were reported by others.9 12 13
Easily available measures such as CRP or ESR and HAQ at inclusion and early radiological changes were identified as predictors of large joint surgery. These results are in line with those reported from several other studies also including patients with different follow-up times.9–13
The presence of one copy of shared epitope was not a risk factor for large joint replacement in our study. However, patients carrying two copies of the shared epitope tended to have an increased risk. These findings are consistent with our previous reports on 5- and 10-year outcomes.15 19 Patients in the joint replacement group were significantly more often treated with DMARDs and oral corticosteroids at year 1, reflecting more severe disease with higher initial disease activity. This is in line with previous findings.10
We have previously reported RF (IgA isotype) and anti-CCP positivity as laboratory markers of joint damage in the same patient cohort as assessed by radiography of hands and feet (Larsen score).18 However, the presence of RF (any isotype) was not identified as a predictor of large joint replacement, which is in accordance with findings in other studies.10 11 Neither was anti-CCP positivity identified as a risk factor of this severe outcome. Anti-CCP is a risk factor for damage of small joints and there is indeed a known association between small and large joint damage. However, one might speculate that patients eventually having total destruction of a large joint might have partly different disease characteristics not captured by anti-CCP.
Recently, a long-term, population-based study reported a decline in the use of orthopaedic surgery, including joint replacement surgery in patients with RA diagnosed after 1985.9 Likewise, the overall number of RA-related surgical procedures of the lower limbs in Swedish patients was found to decrease between 1987 and 2001.20 The need for orthopaedic surgery in RA is still considerable but seems to be declining. Explanations include a possible trend towards a milder course of disease, early and aggressive approach to treatment and the availability of new effective treatments. Use of DMARDs early in the course of disease has been shown to retard development of joint damage in the short term1–4 and should have a positive impact on the subsequent need for joint replacement surgery. Indeed, early treatment with DMARDs and response to treatment were found to reduce the need for surgery in patients with recent onset of RA.11 An intriguing question is whether the early intervention with biological agents in combination with conventional DMARDs can reduce the need for orthopaedic surgery. Results from our study could serve as a reference for comparison with studies including patients with RA in which such aggressive treatment strategies are applied.
In summary, a substantial proportion of patients with RA still require joint surgery. One quarter of patients in this closely monitored early RA cohort needed at least one large joint replacement during 16–20 years after diagnosis. We identified simple clinical measures such as CRP or ESR at diagnosis and HAQ score and radiographic damage of hands and feet early in the course of disease as important predictors of this severe outcome. The identification of factors associated with large joint arthroplasty can lead to better tailored pharmacological treatment to maintain function and prevent the disability of individual patients.
Acknowledgments
This study was supported by grants from the Swedish Rheumatism Association, the Swedish Research Council, the Medical Faculty of the University of Lund, Alfred Österlunds Foundation, the Crafoord Foundation, Greta and Johan Kocks Foundation, the King Gustaf V Foundation and Lund University Hospital.
REFERENCES
Footnotes
Funding: This study was supported by grants from the Swedish Rheumatism Association, the Swedish Research Council, the Medical Faculty of the University of Lund, Alfred Österlunds Foundation, the Crafoord Foundation, Greta and Johan Kocks Foundation, the King Gustaf V Foundation and Lund University Hospital.
Competing interests: None.
Ethics approval: Ethics committee approval obtained.