Article Text

Abstract
Background: Ankylosing spondylitis (AS) and its early form account for up to 5% of all patients with chronic back pain. Interest has recently focused on shortening the delay of 5–10 years between the appearance of first symptoms and the diagnosis of AS, particularly because effective treatments have now become available. Referral parameters that are easy for doctors in primary care to apply to patients presenting with possible AS could contribute to earlier diagnosis.
Methods: Orthopaedists and primary-care doctors were requested to refer patients with (1) chronic low back pain (duration >3 months) and (2) onset of back pain before <45 years of age to a specialist rheumatology outpatient clinic for further diagnostic investigation if at least one of the following screening parameters was present: (1) inflammatory back pain, (2) positive human leucocyte antigen B27, and (3) sacroiliitis detected by imaging. The final diagnosis was made according to expert opinion.
Results: In total, 350 referred cases were analysed. A diagnosis of definite axial spondyloarthritis (axial SpA), comprising established AS and pre-radiographic axial SpA, could be made in 45.4% of all referred patients (of which 50.3% were classified as AS and 49.7% as preradiographic axial SpA), whereas 45.4% were classified as non-SpA and 9.1% as possible SpA. A diagnosis of definite axial SpA could be made in 34.2% if only one referral parameter was positive, and in 62.6% if there was >1 positive referral parameter.
Conclusions: The proposed referral parameters have proven useful when applied in primary care in identifying patients with AS/pre-radiographic axial SpA among young to middle-aged patients with chronic low back pain.
- ankylosing spondylitis
- spondyloarthritis
- pre-radiographic
- screening
- early diagnosis
Statistics from Altmetric.com
Ankylosing spondylitis (AS) is a chronic inflammatory disease with a prevalence of 0.2–1.0%.1 2 AS and other axial spondyloarthritides account for up to 5% of patients with chronic back pain in primary care.3 In about 80% of patients with AS, the disease starts before the age of 30 years, and up to 30% of patients show a course with constantly high disease activity over 1 year as judged by a high Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and/or elevated C-reactive protein (CRP).4 Until recently, the greatest problem in the management of the disease was the lack of effective treatments. This has changed in recent years, as non-steroidal anti-inflammatory drugs (NSAIDs) and tumour necrosis factor (TNF) blockers have been shown to have good efficacy in the treatment of AS.5 Shortening the long delay between the occurrence of the first symptoms and the final diagnosis of AS, which has been reported in several studies to be 5–10 years or even higher,6 has now become an important goal.
An early diagnosis is important in AS for several reasons: (1) it avoids unnecessary diagnostic procedures and inappropriate treatments; (2) patients in the early course of the disease (including patients without radiographic sacroiliits) have at least the same level of disease activity and pain as patients in the later stages;7 (3) treatment with NSAIDs should be started and continued in symptomatic patients once the diagnosis is made, thus early diagnosis facilitates early treatment;8 and (4), patients with AS refractory to conventional treatment respond very well to TNF blockers,9–11 probably even better early in the course of the disease.12 13
There are two major reasons why a diagnosis is delayed in patients with AS. First, radiographic sacroiliitis is normally detectable only several years after the first symptoms, which delays the diagnosis if the modified New York criteria are applied, as is the usual procedure.14 For these criteria, demonstration of radiographic sacroiliitis grade 2 bilaterally or grade 3 or 4 unilaterally is mandatory.15 In recent years, particularly with the detection of acute sacroiliitis and spondylitis by MRI,16 it has become obvious that there is a continuum in inflammation from a pre-radiographic to a radiographic stage.14 17 We have argued recently that the pre-radiographic and radiographic stages of predominant axial spondyloarthritis (SpA), a term recently proposed by us,14 18 should be treated as one disease, that radiological sacroiliitis should not be an essential diagnostic parameter but rather a parameter for severity or chronicity, and that a diagnosis in the pre-radiographic stage can be made reliably if a combination of clinical, laboratory and imaging (especially MRI) parameters are applied.14 18 The second factor, of similar importance, is that there is a low awareness of AS among non-rheumatologists, and it is a major challenge for any doctor in primary care to identify this small group (around 5%) of patients3 with inflammatory spine disease within the large population of patients who present with chronic back pain. Thus, strategies to assist primary-care doctors in identifying inflammatory spine disease in patients with chronic back pain and indicate when to refer these patients to a rheumatologist for a final diagnosis are important.
We recently suggested screening parameters for early referral of patients with AS by primary-care doctors.19 In this paper, we report that the proposed referral parameters performed well in daily clinical practice and allowed identification of patients with axial SpA from among a large group of patients with chronic back pain.
METHODS
Ethics approval from the local ethics committee of Charité University Medicine, Berlin was obtained, and all participants gave informed consent. This study aimed at evaluating our proposed screening parameters to detect patients with axial SpA among patients with low back pain in primary care, and was performed between July 2004 and December 2005. Within this time period, 400 orthopaedists in the Berlin area, covering a population of about 4 million people, were contacted 3 times by letter and asked to refer patients with suspected axial SpA following our parameters. In May 2005 we expanded our project by also contacting 2200 primary-care doctors in the same area, who were contacted twice.
The doctors were asked to refer patients with low back pain (duration >3 months) and onset of back pain before the age <45 years to the rheumatology outpatient clinic of the Charité Campus Benjamin Franklin in Berlin, if at least one of the following screening parameters was present:19 (1) inflammatory back pain (IBP), defined as morning stiffness of >30 minutes, pain at night or in the early morning and improvement by exercise (we did not give any specific instructions about how many of these IBP parameters should be positive); (2) positive testing for HLA-B27 or (3) sacroiliitis detected by and imaging method (however, imaging was not recommended as an initial screening parameter). The referring doctors were asked to document which of those parameters were present.
The diagnostic investigations in the rheumatology clinic included x rays of the sacroiliac joints (SIJ) in all cases if not already provided by the patient, MRI of the SIJ or spine if regarded as necessary by the investigating doctor, and laboratory tests, including testing for HLA-B27 and CRP. A thorough medical history was taken, with particular emphasis on presence of inflammatory back pain and other typical SpA features such as family history, current or previous evidence of heel enthesitis, dactylitis, peripheral arthritis, uveitis, psoriasis, inflammatory bowel disease or reactive arthritis. The time from onset of chronic back pain until a diagnosis was made by us was recorded.
Response to NSAIDs was assessed by measuring the improvement of back pain after a full dose of NSAIDs using a 4-point rating scale (1, no back pain at all; 2, very good improvement of back pain; 3, little improvement; or 4, no improvement).
A diagnosis of ankylosing spondylitis (radiographic axial SpA) was made according to the modified New York criteria15 and a diagnosis of pre-radiographic (undifferentiated) axial SpA made according to expert opinion, but normally at least 3–4 clinical, laboratory or imaging (including knowledge of the MRI results) parameters had to be present.18 A diagnosis of possible axial SpA was made when axial SpA could not be clearly diagnosed but could also not be excluded in the expert’s opinion.
The collected data were entered into a databank and analysed.
RESULTS
Up to January 2006, 114 of 400 (28.5%) orthopaedists and 130 of 2200 (5.9%) primary-care doctors participated in the study by referring patients after applying our screening parameters. In total, 350 patients were referred: 214 by orthopaedists and 136 by primary-care doctors.
Patient characteristics
The mean age of all patients was 40 (range 16–75) years, and 48.6% were male. In total, 46% of patients were referred with only one positive parameter (n = 161/350): HLA-B27 was positive in 35.4% (n = 57) (table 1), IBP was positive in 36.6% (n = 59), 18.6% (n = 30) presented with any sacroiliitis by imaging, and 9.3% (n = 15) were referred for other reasons, such as uveitis or family history.
In 46.6% (n = 163/350) of all patients referred, >1 parameter was positive: 35% (n = 57) were positive for HLA-B27 and IBP, 20.2% (n = 33) for HLA-B27 and for sacroiliitis by imaging, 16% (n = 26) for IBP and for sacroiliitis by imaging, and 20.9% (n = 34) for HLA-B27 and IBP and for sacroiliitis by imaging. For 7.4% of referred patients (26/350), there was no information about these parameters available.
Inflammatory back pain as referral parameter
From the 185 patients sent because the referring doctor had evidence of the presence of inflammatory back pain, this back pain was also interpreted by the expert as inflammatory in 76.8%, possibly inflammatory in 13%, and non-inflammatory in 10.3% of patients.
Diagnosis of axial SpA
In total, 45.4% (n = 159/350) of all referred patients were diagnosed with definite axial SpA, 9.1% (n = 32/350) with possible SpA and 45.4% (n = 159/350) as non-SpA (fig 1, table 1). There was no significant difference between patients referred by orthopaedists and those referred by general practitioners (fig 2), therefore both groups were subsequently treated as one group.


Of the 159 patients diagnosed with axial SpA, 50.3% were classified with AS according to the modified New York criteria (radiographic axial SpA), and 49.7% were diagnosed with pre-radiographic axial SpA (fig 1, table 1).
Information about the presence or absence of chronic (duration >3 months) back pain was available for 348 of the 350. Duration of back pain was >3 months in 90.5% and <3 months in 9.5% (n = 33). In the patients with shorter symptom duration, a diagnosis of pre-radiographic axial SpA was made in 27.3% (n = 9), of AS in 27.3% (n = 9) (a total of 54.6%), of possible SpA in 15.2% and of non-SpA in 30.3%.
As can be seen from table 1 the characteristics of the patients were very similar in both groups; only function (Bath Ankylosing Spondylitis Functional Index; BASFI) was better in the pre-radiographic group than in the AS group (table 1).
Value of MRI in diagnosing axial SpA and assessing acute inflammation
MRI was performed for 75.9% (n = 60/79) of the pre-radiographic axial SpA patients: 38 had MRI of the SIJ only, 2 had MRI of the spine only and 20 had MRI of both the SIJ and the spine. In 87.9% (n = 51/58) of MRI scans of the SIJ but in only 40.9% (9/22) spinal scans, acute inflammatory lesions were detected. One patient had acute inflammatory lesions in the spine but not in the SIJ and no acute lesions were present in the scans of the two patients with MRI of the spine only. In the six patients with MRI scans showing no acute inflammation in SIJ or spine, a diagnosis of pre-radiographic axial SpA was made on the basis of expert opinion, requiring positivity for HLA-B27 plus presence of IBP and at least two further typical SpA features. This was also true for the 19 patients diagnosed with axial pre-radiographic SpA without MRI.
MRI scans were available for 50% (n = 40/80) of patients with AS: 23 had MRI of the SIJ only, 7 of the spine only and 9 of the SIJ and spine. Acute inflammatory lesions were detected in 87.5% (n = 28/32) of MRI scans of the SIJ and in 50.0% (n = 8/16) of MRI scans of the spine.
MRI scans were also available for 57.9% (92/159) of patients who were diagnosed diagnosed as non-SpA. Only 1.5% (1/68) of MRI scans of the SIJ in this group showed active inflammation.
Diagnosing axial SpA according to the number of positive referral parameters
If only one referral parameter was positive, a diagnosis of definite axial SpA, comprising AS and pre-radiographic axial SpA, was made in 34.2% (n = 55/161) compared with 62.6% (n = 102/163) if >1 parameter was positive (fig 2). HLA-B27 was the best-performing single screening parameter (fig 3A).
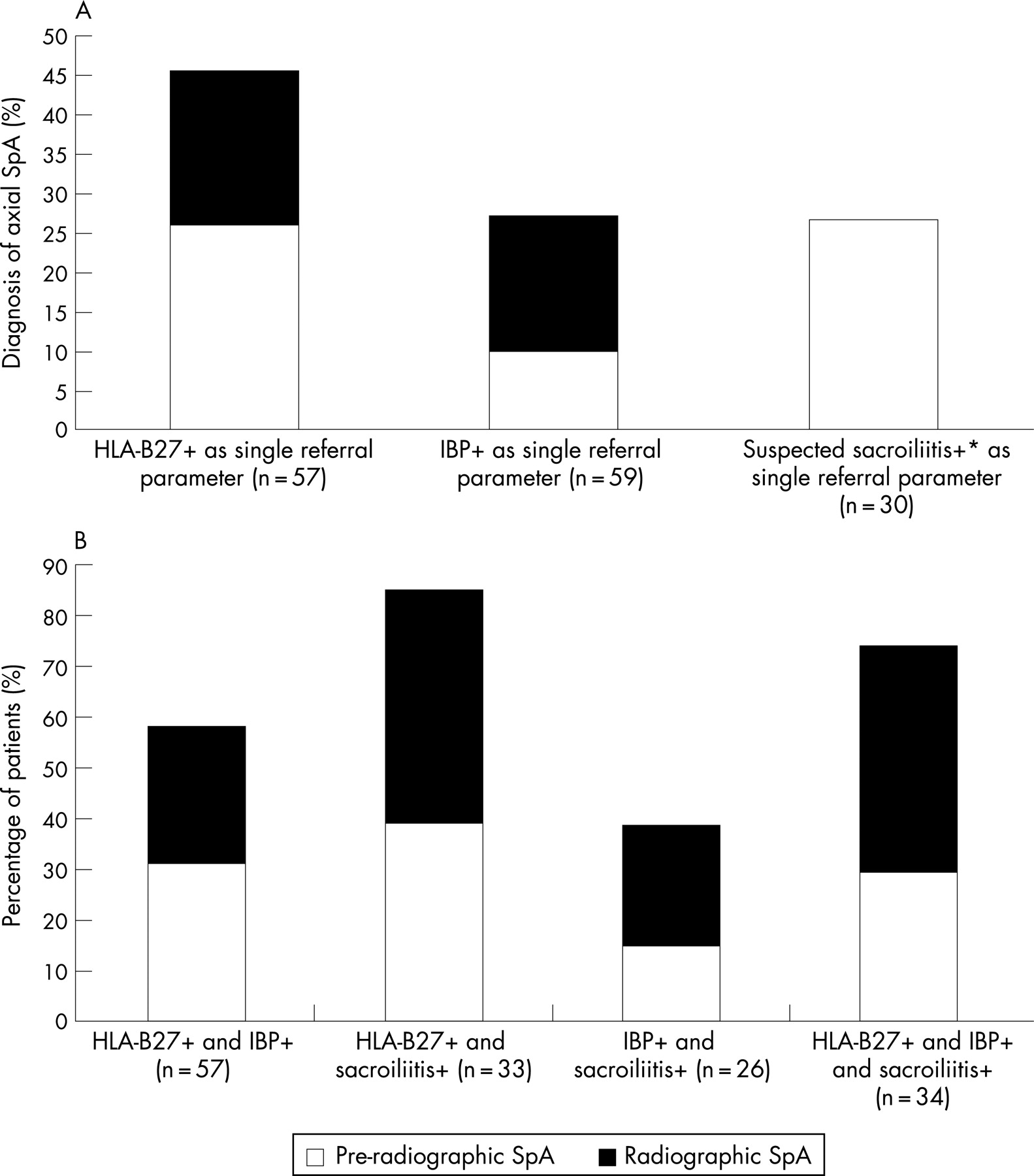
The largest number of diagnoses of axial SpA resulted from a combination ofHLA-B27 positivity and the presence of sacroiliitis by imaging (84.8%, n = 28/33), followed by the combination of HLA-B27 and IBP (57.9%, n = 33/57) and the combination of IBP and sacroiliitis by imaging (38.5%, n = 10/26) (fig 3B).
Presence of further SpA manifestations in patient subgroups
In 56.3% of newly diagnosed patients with AS and 67.1% of pre-radiographic axial SpA patients, at least one further SpA-typical feature18 could be detected, but also in 53.1% in patients with possible SpA and 31% in patients diagnosed as non-SpA.
Interestingly, suspicious sacroiliitis (grade 1 or grade 2 unilaterally) as shown by x rays were present in 68% and normal SIJ in 32% of patients with pre-radiographic axial SpA in comparison to 17% and 83%, respectively, in patients diagnosed as non-SpA. However, the percentage of patients positive for HLA-B27, acute lesions as shown by MRI, or the presence of additional SpA features were similar in pre-radiographic patients with either suspicious or no sacroiliitis, suggesting that suspicious radiographic sacroiliitis is not of major diagnostic value.
Time between first symptoms and making a diagnosis of axial SpA
The mean symptom duration from onset of back pain to the time diagnosis of SpA was made was 7.7 (range 0.1–45, median 5) years for definite axial SpA, 10.7 (range 0.3–45, median 8) years for AS and 4.6 (range 0.1–35, median 2) years for pre-radiographic axial SpA. The mean symptom duration for patients diagnosed with possible SpA was 6.6 (range 0.1–20, median 6) years and 10.1 (range 0.1–50, median 7) years for patients diagnosed as non-SpA (fig 4A). Figure 4B shows the disease duration at different timepoints in the subgroups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
In this study, analysing a relatively large cohort of 350 patients, we show that applying simple screening parameters (presence of inflammatory back pain, positive HLA-B27, or evidence of sacroiliitis by imaging) by primary-care doctors or orthopaedists resulted in a diagnosis of axial SpA by a rheumatologist in about 45% of patients with chronic low back pain. In Germany, patients with chronic low back pain are generally seen by both orthopaedists and primary-care doctors. Interestingly, the screening parameters performed similarly well in both groups.
Importantly, about half of these newly diagnosed patients were diagnosed with pre-radiographic axial SpA14 18 and the other half with established AS with radiographic changes of the SIJ according to the modified New York criteria.15 This also underlines the clinical relevance of the pre-radiographic axial SpA group. Similarity in the percentage of male patients (60% vs 50.6%), in the age at onset of first symptoms (29.5 vs 29.2 years), and in the percentage of patients positive for HLA-B27 (87.5% vs 83.5%) in both the AS and pre-radiographic axial SpA groups, respectively, confirm that this is the same disease, merely diagnosed at different stages in the course of the disease. Interestingly, there were nearly as many female as male patients among the group with axial SpA in our study, supporting the already previously described shift from a predominantly male disease to a disease that now affects both sexes similarly.20
Furthermore, around 20% of patients in both groups had such active disease, as judged by a BASDAI ⩾4 and positive expert opinion, that, despite treatment with NSAIDs, they would have been candidates for treatment with TNF blockers21 if radiographic sacroiliitis were not seen as obligatory for such treatment. Only function, as measured by the BASFI, was better in the pre-radiographic group, reflecting the shorter disease duration and the lack of chronic changes.
There has been an ongoing debate about the importance of diagnosing patients with axial SpA earlier and how to make a reliable diagnosis early. We have argued recently that at least three or four clinical, imaging or laboratory parameters should be positive to make a diagnosis in the pre-radiographic phase.14 18 In this study, a diagnosis was made according to expert opinion. However, in many cases and in all doubtful cases, patients were discussed and a decision was made within our rheumatology group in the presence of at least one senior rheumatologist (MR or JS). Thus, although this process was not formalised, a diagnosis was normally made using our recent suggestions.14 18
Although the clinical symptom of inflammatory back pain is easy to apply as a screening parameter, some clinical experience is necessary for interpretation. In our screening letter, we offered a simple description of IBP. Our study shows that this is a feasible approach because the presence of IBP could be confirmed by the expert in 76.8% of these patients, a very good result in our opinion.
We have discussed recently that HLA-B27 is a suitable screening parameter because of its high sensitivity and specificity and because there is an unequivocal positive or negative result. This was confirmed in this study. However, it has to be stressed that for diagnosis HLA-B27 can only be used in combination with other clinical or laboratory parameters.19
There was a good sensitivity of 87.9% for acute lesions of the SIJ as detected by MRI. Because the disease normally starts in the SIJ,22 it is not surprising that the sensitivity for acute lesions of the spine by MRI (40.9%) was lower than those of the SIJ in pre-radiographic axial SpA. Thus, for a diagnostic approach of early axial SpA, it is probably sufficient to concentrate on MRI of the SIJ. The fact that MRI was an important part of the diagnostic procedure could also contribute to our findings of good sensitivity and specificity.
If ⩾2 of our suggested screening parameters were positive, a diagnosis of axial SpA could be made in 60–80% of patients, a figure that is close to our previous calculation.19 Thus, based on our results, a rheumatologist can make a final diagnosis of axial SpA in 1 out of 2–3 patients referred from non-specialists if our screening approach is applied. In cases where patients were only referred if at least two of the three screening parameters were positive, such a diagnosis could even be made in two out of three patients. However, more patients would be missed with a diagnosis of axial SpA if the presence of two positive parameters were to be considered obligatory for referral.
The relatively high percentage of HLA-B27 positivity (36.5%) and other typical SpA features (31%) in the non-SpA group is not surprising because both were important reasons for referral. Nonetheless, a diagnosis of SpA was excluded in a substantial proportion of patients despite the presence of these features.
The gap of 7.7 years between the occurrence of the first symptoms and making a diagnosis for the whole group of axial SpA is disappointing. This delay is even worse for patients with AS (10.7), but even for patients with pre-radiographic axial SpA, there was an unacceptably delay of 4.6 years. These figures underline the need to develop strategies to identify these patients more accurately and earlier and to confirm our previously discussed assumption that in a substantial proportion of patients the appearance of radiological sacroiliitis is a rather late feature in the course of the disease.14
In conclusion, a combined effort is necessary to make a diagnosis early and in a larger proportion of patients with axial SpA. The approach presented and evaluated here seems to be a useful contribution to achieve this aim.
REFERENCES
Footnotes
The study was partly supported by unrestricted grants from Essex Pharma GmbH, Germany and Wyeth Pharma GmbH, Germany.
- Abbreviations:
- AS
- ankylosing spondylitis
- BASDAI
- Bath Ankylosing Spondylitis Disease Activity Index
- BASFI
- Bath Ankylosing Spondylitis Functional Index
- CRP
- C-reactive protein
- HLA
- human leucocyte antigen
- IBP
- inflammatory back pain
- NSAIDs
- non-steroidal anti-inflammatory drugs
- SIJ
- sacroiliac joints
- SpA
- spondyloarthritis
- TNF
- tumour necrosis factor