Article Text

Abstract
Background: Polymyalgia rheumatica (PMR) may create some difficulties in the differential diagnosis of elderly-onset rheumatoid arthritis (EORA) and of EORA with PMR-like onset (EORA/PMR).
Aim: To investigate possible differences between three groups of patients, with regard to serum levels of inflammatory cytokines and steroidal hormones at baseline and after 1 month of treatment with glucocorticoids (prednisone 7.5–12.5 mg/day).
Patients and methods: 14 patients with PMR, 15 with EORA and 14 with EORA/PMR, as well as 15 healthy, matched controls were analysed. Tumour necrosis factor α (TNFα), interleukin (IL)6, IL1 receptor antagonist (IL1Ra), cortisol, dehydroepiandrosterone sulphate (DHEAS) and 17-hydroxy-progesterone (PRG) were evaluated.
Results: Serum levels of both TNFα and IL6 were significantly higher in all three groups of patients than in controls (p<0.01). Serum IL6 levels were significantly higher in patients with both PMR and EORA/PMR than in patients with EORA (p<0.05). IL1Ra serum levels were significantly higher in patients with EORA than in controls (p<0.001) and in patients with PMR and EORA/PMR (p<0.05). DHEAS was significantly lower in patients with EORA/PMR than in those with EORA (p<0.05). PRG was significantly higher in all patient groups (p<0.05). After glucocorticoid treatment, serum TNFα and IL6 levels significantly decreased in all patient groups; IL1Ra significantly increased in patients with PMR and in those with EORA/PMR; cortisol, DHEAS, and PRG significantly decreased in patients with PMR and in those with EORA/PMR (p<0.05).
Conclusions: Different cytokine and steroidal hormone patterns suggest that patients with PMR and those with EORA/PMR seem to be have a more intensive inflammatory reaction and are more efficient responders to glucocorticoid treatment than patients with EORA.
- ACTH, adrenocorticotrophic hormone
- CRP, C reactive protein
- DHEAS, dehydroepiandrosterone sulphate
- EORA, elderly-onset rheumatoid arthritis
- EORA/PMR, EORA with polymyalgia rheumatica-like onset
- ESR, erythrocyte sedimentation rate
- IL1Ra, interleukin 1 receptor antagonist
- PMR, polymyalgia rheumatica
- PRG, 17-hydroxy-progesterone
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
- ACTH, adrenocorticotrophic hormone
- CRP, C reactive protein
- DHEAS, dehydroepiandrosterone sulphate
- EORA, elderly-onset rheumatoid arthritis
- EORA/PMR, EORA with polymyalgia rheumatica-like onset
- ESR, erythrocyte sedimentation rate
- IL1Ra, interleukin 1 receptor antagonist
- PMR, polymyalgia rheumatica
- PRG, 17-hydroxy-progesterone
- TNFα, tumour necrosis factor α
Polymyalgia rheumatica (PMR) is an inflammatory condition of unknown aetiology characterised by pain and stiffness in the shoulder and in the pelvic girdle. PMR occurs in people aged >50 years and usually responds rapidly to low doses of glucocorticoids and has a favourable prognosis.1,2 Genetic causes and polymorphisms of additional genes associated with the initiation and regulation of inflammatory reaction have been considered possible susceptibility factors for PMR.3,4 In particular, polymorphisms of tumour necrosis factor α (TNFα), and interleukin 1 receptor antagonist (IL1Ra) genes are predisposing factors and may be implicated in the pathogenesis of PMR.5–,7 On the other hand, increased production of interleukin (IL)6 is a characteristic finding in patients with PMR, and glucocorticoids rapidly reduce serum levels of IL6.8,9,10 The suppression of the hypothalamic–pituitary–adrenal axis and ageing may contribute to the pathogenesis of PMR. Ageing is accompanied by marked changes in steroid hormone levels, and the age-related increase of cytokines such as IL6 may modulate the endocrine system. Recently, a reduced production of adrenal hormones, such as cortisol and dehydroepiandrosterone sulphate (DHEAS), has been shown in patients with untreated PMR with active disease, as well as an increased 17-hydroxy-progesterone (PRG) production after adrenocorticotropic hormone (ACTH) testing.10,11
The occurrence of peripheral arthritis, particularly in both hands, may create some difficulties in the differential diagnosis between PMR and elderly-onset rheumatoid arthritis (EORA).12 Symmetrical peripheral involvement, rheumatoid factor seropositivity, development of joint erosions and extra-articular manifestations differentiate rheumatoid arthritis from PMR.1,13,14 Anti-cyclic citrullinated peptide antibodies may also be useful in the differential diagnosis between PMR and EORA.15 However, several patients with seronegative EORA show a relatively mild symmetric synovitis, characterised by a rapid and complete response to glucocorticoids and a non-erosive course.1 Symptoms and signs of both PMR and EORA may alternate during the follow-up of the patients.16 At the beginning of the disease, these patients show a clinical condition different from classic rheumatoid arthritis, which more closely resembles PMR.17–,19 On the other hand, a prospective study on clinical features of PMR and rheumatoid arthritis with PMR-like onset showed that 20% of patients with PMR developed overt rheumatoid arthritis during the follow-up period.20
The aim of our study was to evaluate the possible differences between EORA and PMR, as well as between these clinical conditions and EORA with PMR-like onset (EORA/PMR), with respect to some inflammatory cytokines (TNFα, IL6 and IL1Ra) and steroidal hormones (cortisol, DHEAS and PRG). Serum levels of cytokines and steroids, erythrocyte sedimentation rate (ESR) and the C reactive protein (CRP) level were evaluated at baseline and 1 month after glucocorticoid treatment.
PATIENTS AND METHODS
Patients
Of the 43 patients and 15 controls evaluated, 14 patients had PMR (4 men and 10 women; mean (standard deviation (SD)) age 73 (4) years; mean disease duration 2.8 (2) months), 15 had EORA (4 men and 11 women; mean age 72 (6) years; mean disease duration 3.7 (2.4) months) and 14 patients had EORA/PMR (4 males and 10 females; mean age 70 (7) years; mean disease duration 3.6 (2.2) months). Patients with PMR met the criteria set out by Chuang et al.21 Patients with EORA (disease onset after 60 years of age) had peripheral arthritis and met at least four American College of Rheumatology criteria for rheumatoid arthritis.22 Patients with EORA/PMR had pain and stiffness in both shoulders and in the pelvic girdle, together with peripheral arthritis, and met at least four American College of Rheumatology criteria for rheumatoid arthritis. The patients were diagnosed the first time and they were not treated with corticosteroids before the study. Furthermore, no patient was taking immunosuppressive agents before and during the study. All groups of patients received only prednisone (7.5–12.5 mg/day), and paracetamol was the only additional drug permitted for pain relief during the study (maximum dose 3 g/day). In our clinical practice, the starting prednisone dose in patients with PMR is not higher than 12.5 mg/day, at least in the absence of temporal arteritis. No patient had vasculitic symptoms, and the lower dosage was due to the presence of patients with diabetes mellitus or altered cardiac function. For these reasons, the prednisone dose was between 7.5 and 12.5 mg/day. The controls (4 men and 11 women; mean age 70 (SD 7) years) had osteoarthritis of the knee or hip, and their routine laboratory examination results were normal. All patients and controls gave their informed consent to be enrolled in the study.
Cytokine and hormone assessment
At baseline, fasting blood samples were collected between 08:00 and 09:00 h. All patients were subjected to a further blood analysis 1 month after glucocorticoid treatment. Blood samples were centrifuged 30 min after collection. Tubes containing serum tubes were frozen at −70°C to allow all samples to be tested at the same time.
The following cytokines and hormones were evaluated: IL6, TNFα, IL1Ra, cortisol, DHEAS and PRG.
ELISA was used to measure serum levels of IL1Ra (Beckman Coulter, Marseille, France), IL6 and TNFα (Cayman, Ann Arbor, Minnesota, USA). Each kit specifically measures both natural and recombinant human TNFα, IL6 and IL1Ra, showing no detectable cross-reaction with other cytokines. The detection limit was 1.5 pg/ml for TNFα, 2 pg/ml for IL6 and 30 pg/ml for IL1Ra. Intra-assay and inter-assay coefficients of variance (CVs) were 1.97% and 3.85% for TNFα, 2.34% and 3.86% for IL6, and 4.35% and 8.6% for IL1Ra, respectively. The results were expressed in pg/ml. Serum levels of cortisol and DHEAS were assayed by a chemiluminescent method (DPC, Los Angeles, California, USA, and Nichols Institute of Diagnostics, San Juan Capistrano, California, USA, respectively), with a detection limit of 0.552 nmol/l for cortisol and 0.003 nmol/l for DHEAS. CVs were 6.5% for cortisol and 6.7% for DHEAS. Serum levels of PRG were measured by direct immunoenzymatic method (Mascia Brunelli, Milan, Italy), with a detection limit of 0.150 nmol/l and a CV of 5.4%. The results for hormones were reported in nmol/l. All samples were tested in triplicates.
CRP was evaluated by routine nephelometric examination and values were expressed in mg/l. ESR was assessed routinely by Westergren method (mm at the end of the first hour).
Statistical analysis
Data were analysed using non-parametric Wilcoxon signed rank test to compare the median levels of both cytokines and hormones at different times, and Mann–Whitney U test to compare the median levels of both cytokines and hormones between the different groups of patients. Spearman’s rank correlation test was used to assess possible correlations between variables. A p value <0.05 was considered significant.
RESULTS
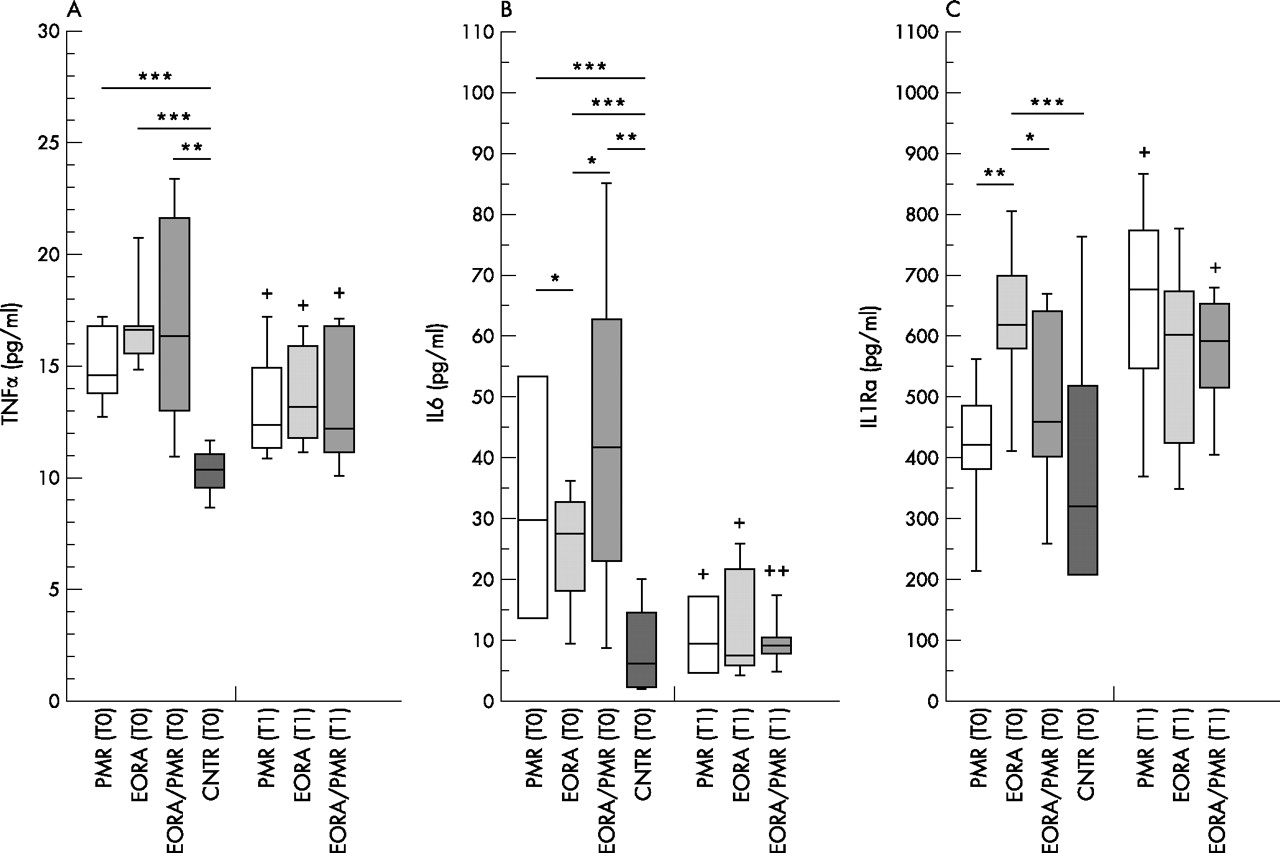
No significant difference was found between the groups with regard to age of participants and disease duration in patients. Serum TNFα levels were significantly higher in all three groups of patients, but there was no statistically significant difference for serum TNFα levels between the three groups of patients (fig 1A⇓). Serum IL6 levels were significantly higher in patients with PMR, EORA/PMR, and EORA, than in controls. Furthermore, serum IL6 levels were significantly higher in patients with PMR and those with EORA/PMR than in patients with EORA (fig 1B⇓).

Serum levels of tumour necrosis factor α (TNFα) (A), interleukin-6 (IL6) (B) and interleukin-1 receptor antagonist (IL1Ra) (C) in patients with polymyalgia rheumatica (PMR), elderly-onset rheumatoid arthritis (EORA), EORA with polymyalgia-like clinical onset (EORA/PMR) and controls (CNTR) at baseline (T0) and 1 month after glucocorticoid treatment (T1). Data are given as box plots with 5th, 10th, 50th (median), 90th and 95th centiles. *p<0.05; **p<0.01; ***p<0.001 between groups. +p<0.05; ++p<0.01 T1 v T0.
On the contrary, IL1Ra serum levels were significantly higher in patients with EORA than in controls, as well as in patients with PMR and those with EORA/PMR. We found no significant difference regarding serum IL1Ra levels between patients with PMR and those with EORA/PMR. In addition, we found no statistically significant difference regarding serum IL1Ra levels between controls and patients with PMR and those with EORA/PMR; however, IL1Ra levels were lower in controls (fig 1C⇑).
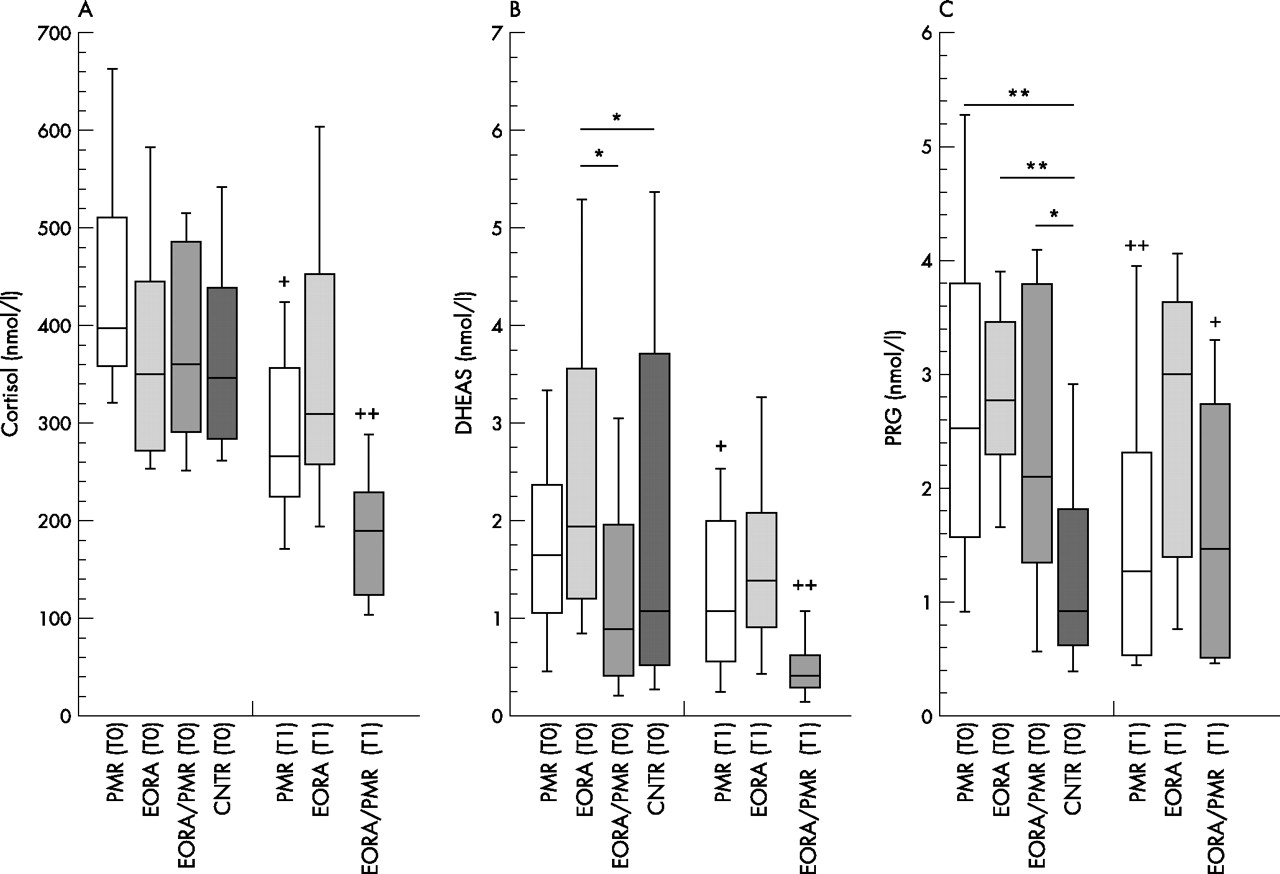
We found no statistically significant difference regarding cortisol serum levels between the four groups of participants. However, cortisol level was slightly higher in patients with PMR than in other groups (fig 2A⇓). DHEAS was markedly lower in patients with EORA/PMR than in those with EORA. We observed no statistically significant difference regarding DHEAS between patients with PMR and other groups (fig 2B⇓). PRG levels were significantly higher in all three groups of patients than in controls, whereas no statistically significant difference was found for PRG levels between the three groups of patients (fig 2C⇓). As regards to sex selection, all groups had a similar sex ratio of patients (four male patients in each group), and the limited number of patients enrolled into the study did not allow for any statistical analysis on hormone levels in both sexes in each group.
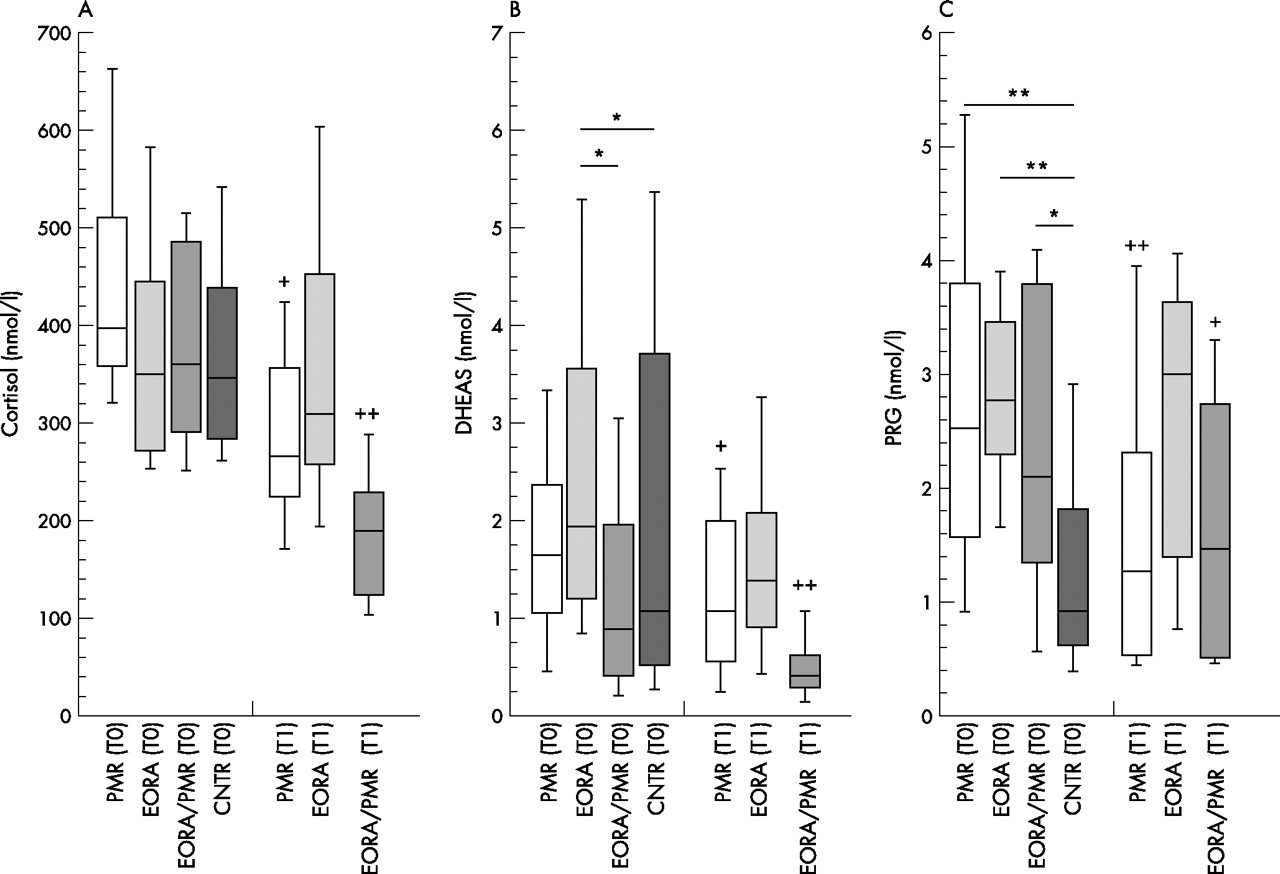
Cortisol (A), dehydroepiandrosterone sulphate (DHEAS) (B), and progesterone (PRG) (C) serum levels in patients with polymyalgia rheumatica (PMR), elderly-onset rheumatoid arthritis with polymyalgia rheumatica-like onset (EORA/PMR) and controls (CNTR) at baseline (T0) and 1 month after glucocorticoid treatment (T1). Data are given as box plots with the 5th, 10th, 50th (median), 90th and 95th centiles. *p<0.05; **p<0.01 between groups. +p<0.05; ++p<0.01 T1 v T0.
Interestingly, ESR and CRP values were significantly higher in patients with PMR and those with EORA/PMR than in patients with EORA (fig 3⇓).

{kind=link}
{kind=link}
{kind=link}
Erythrocyte sedimentation rate (ESR) (A) and C reactive protein (CRP) (B) in patients with polymyalgia rheumatica (PMR), elderly-onset rheumatoid arthritis with polymyalgia rheumatica-like onset (EORA/PMR) at baseline (T0) and 1 month after glucocorticoid treatment (T1). Data are given as box plots with the 5th, 10th, 50th (median), 90th and 95th centiles. *p<0.05 between groups. +p<0.05; ++p<0.01 T1 v T0.
After 1 month of glucocorticoid treatment, several statistically significant variations were observed. Serum TNFα and IL6 levels decreased considerably in all groups of patients (fig 1A⇑,B). IL1Ra increased markedly in patients with PMR and those with EORA/PMR, whereas no statistically significant variation was observed for IL1Ra in patients with EORA (fig 1C⇑). Cortisol, DHEAS and PRG decreased noticeably in patients with PMR and in those with EORA/PMR (fig 2A⇑–C). Finally, ESR and CRP decreased markedly in patients with EORA/PMR after CG treatment when compared with basal time values (fig 3A⇑,B).
DISCUSSION
With regard to the laboratory markers of inflammation, the present study suggests that patients with PMR and those with EORA/PMR are affected by a stronger inflammatory involvement than patients with EORA, as shown by their significantly higher values of ESR, CRP and IL6. On the contrary, IL1Ra was found to be significantly higher in patients with EORA than in those with EORA/PMR. As IL1Ra wields a protective effect on bone damage, the higher serum IL1Ra levels observed in patients with EORA may support the low erosive activity typical of the elderly subset of rheumatoid arthritis.23,24
Regarding patients with EORA/PMR and those with PMR, IL6, IL1Ra and ESR values, showed a similar behaviour in the patients with EORA at the time of the basal analysis. However, at that time, all the analysed cytokines were considerably higher in the three groups of patients than in the control group.
After glucocorticoid treatment, the decrease in the inflammatory markers was more evident in patients with PMR, as well as in those with EORA/PMR, than in patients with EORA.
In particular, the decrease in TNFα, IL6, ESR and CRP was markedly higher in patients with EORA/PMR, whereas IL1Ra increased considerably only in patients with EORA/PMR and those with PMR, and no statistically significant variation was observed for patients with EORA.
No statistically significant differences were observed with regard to cortisol levels between the three groups of patients and the controls. The results of this study confirm the findings of recent research showing a reduced production of adrenal hormones (cortisol, DHEAS) at baseline in patients with active and untreated PMR.11 The defect seemed mainly related to altered adrenal responsiveness to ACTH stimulation (ie, increased PRG), at least in untreated patients, and 1 month of glucocorticoid treatment reduced the production of inflammatory mediators (ie, IL6) in a stable manner, an effect which persisted after glucocorticoid tapering.11 Therefore, PMR may be considered a hypothalamic–pituitary–adrenal axis-driven disease.10,25 Interestingly, in the present study, the decrease in serum cortisol levels induced after 1 month of glucocorticoid treatment was more evident in patients with PMR and those with EORA/PMR, suggesting higher hypothalamic–pituitary–adrenal axis responsiveness than in patients with EORA. However, the frequent observation of reduced cortisol and adrenal androgen secretion during testing in patients with rheumatoid arthritis not treated with glucocorticoids should clearly be regarded as an “adrenal insufficiency” in the setting of a sustained inflammatory process, as shown by high serum IL6 levels. In other words, the production of adrenal hormones (cortisol and DHEAS) in patients with PMR was found to be lower than IL6 or TNFα levels.26,27
Similarly, DHEAS levels were markedly lower in patients with EORA/PMR than in controls, whereas in our study, no statistically significant difference was detectable in patients with PMR. The reduction in DHEAS is a general feature of chronic inflammatory diseases.28–,31 In the biosynthesis of steroids, the enzyme 17,20-lyase (P450c17) is suppressed both during ageing and in response to inflammatory stimuli, such as IL1 and transcription growth factor type β1.32–,36 Therefore, during ageing and under conditions of systemic inflammation (such as PMR), the suppression may be due to an inhibition of the adrenal 17,20-lyase, as cortisol under the same circumstances is increased in relation to DHEAS. Furthermore, the cytokine-induced inhibition of the sulphatase reaction (DHEA/DHEAS) may also be considered.37,38
A marked increase in PRG levels in both basal condition and after ACTH stimulation was described in patients with recent-onset untreated PMR compared with age-matched controls. Our results have confirmed this even in other groups of patients (EORA and EORA/PMR).11 As PRG represents a precursor of cortisol biosynthesis at the adrenal level, a possible partial impairment of the enzyme 21α-hydroxylase (P450c21) may lead to accumulation of the precursor PRG. The reasons for a functional 21α-hydroxylase impairment in PMR may include genetic defects, an age-related increase of serum TNF level in healthy women, or raised serum IL6 and TNFα levels during chronic systemic inflammatory stimuli (ie, PMR).10 TNFα was shown to inhibit 21α-hydroxylase in adrenal cell cultures, and high concentrations of IL6 and TNFα have been shown to interfere with enzymes associated with peripheral steroid hormone metabolism.38,39 Furthermore, TNFα may be a blocker of the 17,20-lyase, altering the biosynthesis of steroids and inducing the increase in PRG levels.38
The quite similar hormonal changes observed in patients with PMR and those with EORA/PMR may reflect a more severe interference of the inflammatory cytokines on the steroid hormone metabolism than in patients with EORA. The hormonal differences may be related to the different severity of inflammation. It seems that lower hormonal levels, as observed in patients with EORA/PMR and those with PMR, are negatively related to a higher inflammatory reaction that distinguishes EORA/PMR and PMR from EORA. Therefore, these results indicate that patients having clinical characteristics of EORA and PMR as well should be treated as patients with PMR, at least at the beginning of the disease. In addition, the effects of the glucocorticoid treatment, acting as a replacement for the reduced endogenous cortisol production, seems again more efficient in patients with PMR and those with EORA/PMR (ie, marked decrease in serum IL6 and PRG), than in patients with EORA, at least in a short time (1 month).
In conclusion, patients with PMR and those with EORA/PMR seem to be characterised by a more intensive inflammatory reaction and seem to respond better to the glucocorticoid treatment than patients with EORA. These results further support a recent study suggesting that no routine laboratory marker of inflammation allows for early differentiation between patients with EORA/PMR and those with persisting PMR.20
REFERENCES
Footnotes
Published Online First 2 June 2006
Competing interests: None declared.