Article Text

Abstract
Background: Work disability—a common outcome of rheumatoid arthritis (RA)—is a societal (for example, financial costs) and individual problem (for example, loss of status, income, social support, and distraction from pain and distress). Until now, factors that predict work disability in RA have not been systematically reviewed.
Objective: To determine predictive factors of work disability in RA as reported in the literature.
Methods: A systematic literature search in Cinahl (1988–2004), Embase (1988–2004), and Medline (1989–2004) was followed by the application of two sets of criteria related to: (a) methodological quality, and (b) measurement of the predictive factor. Based on the quality and the consistency of the findings, a rating system was used to assess the level of evidence for each predictive factor.
Results: Nineteen publications (17 cohorts) were identified, of which 13 met the general methodological quality criteria. Results provided strong evidence that physical job demands, low functional capacity, old age, and low education predict work disability in RA. Remarkably, biomedical variables did not consistently predict work disability. Moreover, owing to the lack of high quality studies no evidence was found for personal factors such as coping style, and work environmental factors such as work autonomy, support, work adjustments that are presumed crucial in the work disablement process.
Conclusions: The results indicate that work disability in RA is a biopsychosocially determined misfit between individual capability and work demands.
- DMARD, disease modifying antirheumatic drug
- ICF, International Classification of Functioning, Disability and Health
- RA, rheumatoid arthritis
- RF+, rheumatoid factor positivity
- rheumatoid arthritis
- work disability
- predictive factors
Statistics from Altmetric.com
- DMARD, disease modifying antirheumatic drug
- ICF, International Classification of Functioning, Disability and Health
- RA, rheumatoid arthritis
- RF+, rheumatoid factor positivity
A large number of patients with rheumatoid arthritis (RA) are work disabled.1–4 The lowered RA-induced work ability is a societal5 (for example, financial costs) and individual problem6–10 (for example, loss of status, income, social support, and distraction from pain and distress).
Initially, the relation between RA and work disability was examined from a biomedical perspective. From this perspective, disease activity (that is, inflammation) quantified as erythrocyte sedimentation rate and number of tender or swollen joints results in structural damage (that is, joint damage and deformity). Structural damage, in turn, results in limitations of physical functions, expressed as limited mobility, strength, and manual dexterity. Work disability may occur early owing to inflammatory processes or later in this process owing to joint destruction.
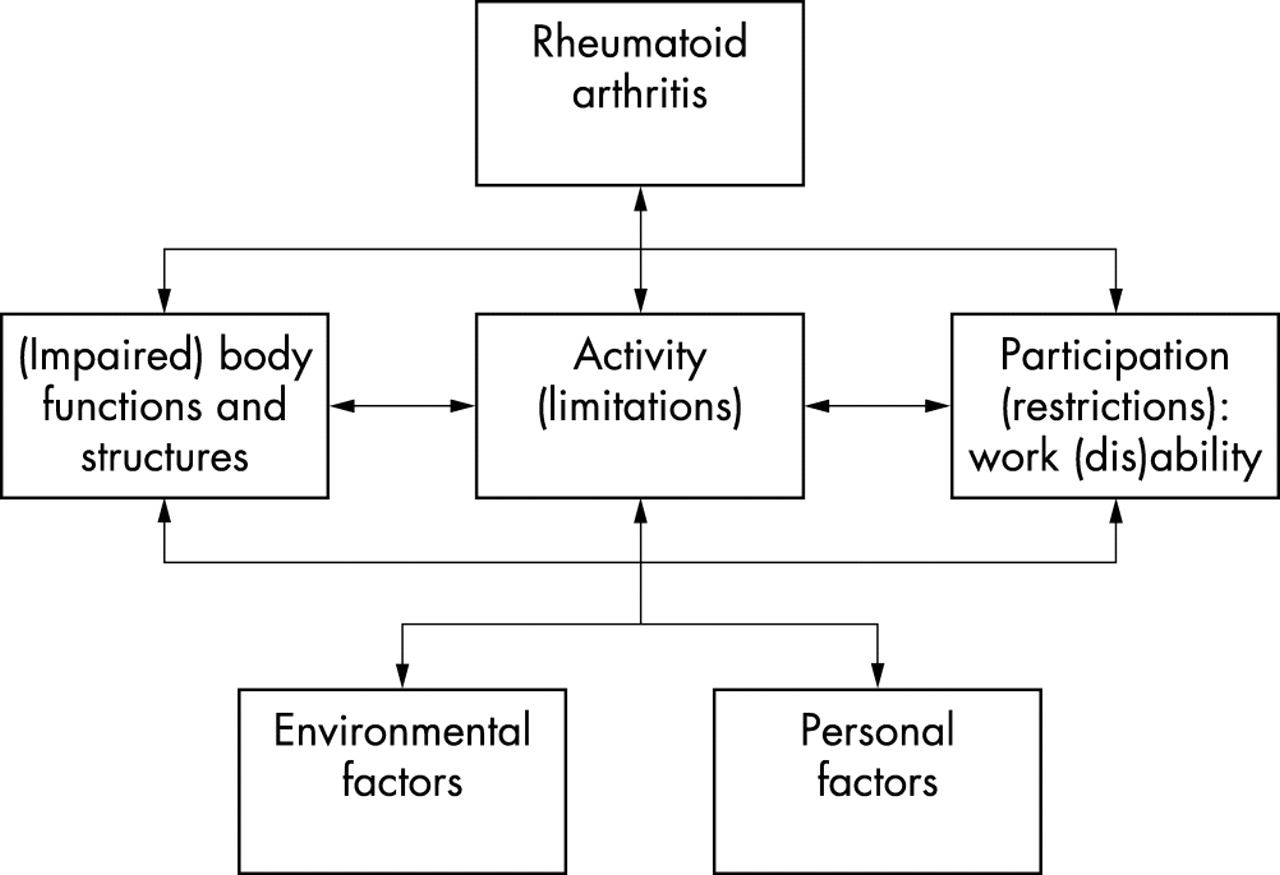
The awareness that work disability is a misfit between functional capability and work environmental demands11 has instigated researchers to use models that explain work disability from a biopsychosocial perspective.12–15 Promising in this respect,16 is the International Classification of Functioning, Disability and Health (ICF).17 The ICF organises information into (a) (impaired) body functions or structures—disease activity and structural damage; (b) activity (limitations); and (c) participation (restrictions) such as work disability. In addition, contextual variables—namely, (d) environmental and (e) personal variables are included (fig 1).

{kind=link}
ICF model applied to work disability in RA.
With the recognition of work disability as a biopsychosocial phenomenon, multidisciplinary programmes aimed at the vocational rehabilitation of subjects with RA have been introduced. De Buck et al showed that evidence of the effectiveness of these programmes is limited.18 Owing to methodological flaws, inadequate descriptions, and late initiation, it remains uncertain at which factors these programmes should be directed to promote work ability of subjects with RA.
The lack of research which evaluates treatment early in the RA work disablement process is reflected in a review by Steultjens et al.19 This review showed that of the 37 studies that evaluated occupational treatment in RA—facilitation of performance of daily living activities—none had included work disability as an outcome. Hence, the recognition that prevention of work disability is preferable to rehabilitation is not mirrored in an equal amount of research attention.
The scarcity of work disability prevention research is in contrast with the many studies on predictive factors of work disability.3,20–24 This article describes a systematic and critical evidence synthesis of these studies.
METHODS
Search strategy
A search in March 2004 in (a) Cinahl (1988–2004), (b) Embase (1988–2004), and (c) Medline (1988–2004) with the following free text words in the title and abstract was performed:
-
rheumatoid arthritis
-
work ∪ working ∪ worker ∪ workers ∪ occupation ∪ occupations ∪ occupational ∪ vocation ∪ vocational ∪ labor ∪ labour ∪ job ∪ jobs ∪ employ ∪ employment
-
ability ∪ abilities ∪ able ∪ disablement ∪ disabled ∪ unable ∪ disability ∪ disabilities ∪ capability ∪ capabilities ∪ capable ∪ incapable ∪ functioning ∪ performance ∪ dysfunction ∪ capacity ∪ participation
Combination of these words (1 ∩ 2 ∩ 3) resulted in 765 hits of which only English publications that described empirical research or reviews were retained. This resulted in 391 publications to be included in subsequent selection steps.
Selection
The first reviewer (EdC) made a selection of the identified papers. To check the reproducibility, the second reviewer (JKS) repeated the selection in a random sample (n = 50) from the papers identified initially. In cases of doubt (<4%), consensus was reached. Firstly, studies were included on the basis of title and abstract. For this purpose two inclusion criteria were formulated: (a) the study population consists of subjects with RA, and (b) the study examines work (dis)ability or equivalent concepts as the outcome. Thereafter, studies with a prospective, retrospective cohort, or case-control design were included on the basis of the abstract or full report.
Methodological quality assessment
Firstly, based on eight criteria25 (table 1) studies were classified as high (>6 criteria), medium (4–5 criteria), or low quality (<4 criteria). Low quality studies were excluded from the review. Thereafter, the studies remaining had to ascertain that (a) the instruments that were used were (psycho)metrically sound and (b) the predictive factor chronologically preceded work disability.
Information on design, sample size, duration of follow up, disease duration, and quality criteria of the 17 studies
Best evidence synthesis
The information was synthesised into four evidence levels: (a) no evidence: ⩽1 study available; (b) weak evidence: 2 studies available that find a significant association in the same direction or 3 studies available, of which 2 find a significant association in the same direction and the third study finds no significant association; (c) strong evidence: 3 studies available that find an association in the same direction or >4 studies available, of which >66% find a significant association in the same direction and no more than 25% find an opposite association; and (d) inconsistent evidence: remaining cases. Finally, weak or strong evidence for “no association” is provided when >4 studies are available, of which >75% and >85%, respectively, find no association.
RESULTS
Selection and methodological quality assessment
The search resulted in 391 citations. Application of the inclusion criteria resulted in 19 papers that presented 17 studies. Three papers described baseline,7 5 year,26 and 10 year27 follow up results of the same sample. Only the 10 year follow up article27 was included. All papers provided valuable information on work disability in RA, but varied in the scores on the quality criteria formulated for the purpose of this study. In particular, six, seven, and four studies were rated as high, medium, and low quality, respectively (table 1). This review is based on the 13 high or medium quality studies.
Definition and measurement of work disability
Two studies did not embody RA or ill health as a reason for work termination in the work disability definition (criterion 6).27,34 Six studies did not include an external criterion for the work disability measurement (criterion 7).1,3,4,27,31,34 Five studies1,4,13,32,33 asked work disabled subjects with RA to recall whether work disability occurred before or after disease onset (criterion 8).
Predictive factors of work disability
Factors that mirror RA directly
Rheumatoid factor positivity (RF+)
Two prospective studies1,30 found a positive and two prospective studies2,3 found no association between RF+ and work disability. Two studies13,31 measured RF+ after work disability, and, therefore, were not taken into account. Therefore, the evidence that patients with RA with RF+ have an increased chance of work disability is inconsistent.
Disease duration
Eight studies1,2,4,13,27,30,32,33 reported an association between disease duration and work disability. Three studies were not taken into account because they were conducted among patients with early RA in the same stage of the disease.2,4,30 (see table 1 for information on disease duration for each study). Of the five remaining studies, three13,32,33 found a positive and two1,27 found no association. Thus the evidence that employed patients with RA with long disease duration have an increased chance of work disability is inconsistent.
Impaired body function or body structure
Variables of disease activity
Nine studies1,2,4,13,27,28,30,31,34 examined the association between variables of disease activity and work disability. Studies that quantified variables of disease activity averaged over time or after work disability occurred were not taken into account in the analyses (shown between brackets in table 2). Synthesis of the remaining evidence discloses inconsistent evidence that subjects with RA with high disease activity have an increased chance of becoming work disabled.
Results of the best evidence synthesis
Pain and emotional functions
Eight studies examined the association between pain and work disability.1,2,13,27,28,31,33,34 Five studies were not taken into account because they only reported on the cross sectional association or on the association between joint pain over time and work disability (shown between brackets in table 2). Synthesis of the three remaining studies demonstrates inconsistent evidence that subjects who experience high pain are more likely to become work disabled. Four studies1,28,33,34 investigated the role of emotional functions (that is, psychological distress, helplessness, depression, and anxiety) in the work disablement process. One retrospective study33 assessed emotional functions—namely, helplessness, after work disability, and, therefore, was not included in the evidence synthesis. Combination of the three remaining prospective studies resulted in weak evidence that patients with RA with emotional problems run an increased work disability risk.
Structural damage
Six studies2,13,27,30,31,34 inspected the relationship between structural damage and work disability. Two studies13,34 reported on the cross sectional association between the two variables and, therefore, were not taken into account. Analyses of the four other studies provided inconsistent evidence that structural damage predicts work disability.
Activity limitations
Six prospective1–3,28,31,34 and four retrospective studies4,13,32,33 demonstrated a positive association between low functional capacity, assessed by the (modified) Health Assessment Questionnaire (HAQ-disability)39 and work disability. Because the retrospective studies measured HAQ-disability in subjects with RA who were already work disabled, they were not taken into account in the evidence synthesis. In conclusion, there is strong evidence that patients with RA with many activity limitations, expressed as high HAQ-disability, have an increased chance of becoming work disabled.
(Work) environmental factors
All studies except that of Doeglas et al4 investigated at least one environmental work disability predictor. Studies that (a) reported cross sectional associations; (b) did not provide psychometric information on the questionnaires; or (c) asked patients with RA to recall subjective work related information (for example, working hours before work disability occurred) were not taken into account in the evidence synthesis (displayed between brackets in table 2). Synthesis of the remaining evidence shows (a) there is inconsistent evidence that patients with RA who supervise others have a lowered chance of work disability; (b) there is strong evidence that patients with RA employed in physically demanding occupations have an increased chance of becoming work disabled; (c) there is weak evidence that patients with RA with a part-time job (that is, small number of working hours) have an increased chance of work disability; and (d) there is inconsistent evidence for an association between the financial situation of the patients with RA and the occurrence of work disability.
Personal factors
Personal factors that are stable over time (that is, age, sex, marital status, educational level, and race) were frequently examined as predictive factors of work disability. Synthesis of these studies shows that (a) there is strong evidence that older patients with RA have an increased chance of becoming work disabled; (b) there is inconsistent evidence that women with RA have an increased chance of work disability; (c) there is strong evidence for no association between marital status and work disability; (d) there is strong evidence that less educated patients with RA are more likely to become work disabled; and (e) there is weak evidence that non-white patients with RA have an increased risk of work disability.
Remaining variables
Owing to lack of information for several variables “no” evidence was found. Table 2 displays these variables, which include, among others, morning stiffness, grip strength, and absenteeism (indicators of activity limitations), work autonomy, job satisfaction, support at work, the impact of RA on family roles, car/stair deprivation (environmental variables), desire for paid work, the presence of comorbid conditions, and behavioural coping styles (personal variables).
DISCUSSION
This review shows that physical job demands and HAQ-disability—a correlate of structural damage, disease activity, pain, and psychological factors40,41—predict work disability. Contrarily, this review failed to supply consistent evidence for the direct effect of (bio)medical variables on work disability. This indicates that reliance on biomedical models is insufficient to explain work disability.11–14,16,42 It confirms that work disability is a biopsychosocially determined misfit between work environmental demands and individual capability.
Other reviews3,20–24 have also concluded that physical job demands, HAQ-disability, old age, and low education predict work disability. Conversely, the lack of evidence for biomedical variables as work disability predictors contradicts one review.23 Our reliance on studies which ascertained that the predictive factor under study preceded work disability may explain this discrepancy. The studies that did not ascertain this sequential association found a significant positive association more frequently. Presumably, as noted by Wolfe and Hawley,1 compared with subjects with RA who remain employed, disease progression is less favourable among subjects who become work disabled. Also, work disability itself may stimulate disease progression7,8,43 because of the loss of psychosocial, financial, and medical benefits (for example, esteem, social support, distraction, income, insurance, and medical care).
Five other aspects of this review warrant comment. Firstly, it should be noted that we used the term “predictive factor” to describe a statistical and not, necessarily, an aetiological association between the predictive factor under study and work disability.
Secondly, although work disability increases during the course of the disease,1,6,34,44 we did not find consistent evidence that disease duration predicts work disability. The different effect of RA on work disability during the course of the disease may explain this inconsistency. Disease activity may affect work disability most dramatically in early disease,45 whereas structural damage and illness factors may become more important in late disease.27,45 Unfortunately, we could not gain a clear understanding of work disability predictors in early, compared with late, disease because only three studies28,30,46 examined predictors in the first 5 years of the disease.
Thirdly, studies that examined drug treatment were not included in the synthesis. Given the beneficial effects on structural damage and functional capacity of treatment with biological agents and combination of disease modifying antirheumatic drugs (DMARDs),47,48 such treatment may influence work disability substantially. Recent studies support this presumed beneficial effect.28,49–51 Borg et al, for instance, found that early treatment with a DMARD (namely, auranofin) delayed work disability.28 Bresnihan et al showed that early treatment with a biological agent (that is, anakinra) increased the number of productive days.51 Furthermore, Yelin and colleagues showed that early DMARD treatment (with etanercept) was associated with longer weekly working hours.49 Finally, Puolakka et al demonstrated that early DMARD combination treatment decreased sickness absence in comparison with single DMARD treatment.50 Although more research is required, the results, so far, indicate that in addition to non-medical interventions,52 medical treatment in early RA may prevent work disability.
Fourthly, because the synthesis took only statistically significant associations into account, our conclusions are on the safe side. Particularly, clinically significant, but statistically non-significant effects in studies with few patients with RA might have reached statistical significance with larger sample sizes. Consequently, it may be argued that in some instances we have wrongly concluded that no clinically relevant effect exists. However, considering the number of patients in each study—which was at least 73—the statistical power of each study seems sufficient to demonstrate clinically relevant effects.
Fifthly, this review showed that old and less educated subjects with RA are more likely to become work disabled. Presumably, these subjects are comparatively unhealthy, are more often employed in physically demanding occupations, and are less likely to find alternative employment or to have high socioeconomic status.1 These characteristics, in turn, predict work disability.
The role of other personal factors was examined also. Reisine et al disproved the suggestion that work disability results from a low desire for paid work.27 Furthermore, work disabled subjects with RA were found to more frequently report emotional problems, adverse coping styles, a lack of work adjustment, job training, and support at work28,32,33 than working subjects with RA. These studies are important in highlighting work disability factors that are responsive to intervention.
The studies about work environmental variables are important for the same reason. However, these studies have tended to use invalidated instruments or occupational title as a proxy for the work characteristic under study. Studies that used invalidated instruments were not taken into account in the evidence synthesis. Studies that used the occupational title53 were taken into account, but may not give a precise representation of the work setting.54 Preferably, as noted by Shanahan et al,55 studies on work demands estimate specific tasks—for instance, repetitive movements of the hand, by the use of validated self report scales and trained observers.
Following on from this, the challenge is to examine how work disability predictors influence this phenomenon. For this purpose, more research is needed that examines variables such as employability, lifestyle, physical work tasks, and coping styles that mediate or moderate the effect of known work disability precursors such as age, education, occupation, and HAQ-disability. This research may provide more concrete cues for work disability prevention.
Based on the present results, interventions aimed at work disability prevention should reduce physical job demands and slow down functional disability. Reduction of physical job demands may be brought about through job accommodation56 or by encouraging and assisting subjects with RA in physically demanding jobs to move to physically less demanding jobs. Obviously, the success of these interventions depends on employability, alternative employment availability, and re-education opportunities. Because low functional disability (HAQ-disability) integrates structural damage, disease activity, pain, and psychological factors,40 interventions that slow functional disability require treatment of the disease,57 and related problems.