Article Text

Abstract
Background: The survival rate in patients with systemic lupus erythematosus (SLE) has improved dramatically during the past four decades to 96.6% (five year) in the Erlangen cohort, but it is nearly three times as high as in an age and sex matched control population. Reasons for death are mainly cardiovascular diseases (37%) and infections (29%).
Objective: To find risk factors existing at disease onset for a severe outcome in the Erlangen cohort.
Patients and methods: By using a database of 338 patients with SLE from a single centre, documented at least one to 15 years and including Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) damage score data and index (SDI) and an activity score (European Consensus Lupus Activity Measurement (ECLAM)), a retrospective search was made for risk factors for a severe outcome like death, end stage renal disease (ESRD), and thromboembolic events (TE) in SLE. For this purpose, multivariable Cox regression models were analysed using the statistical package SPSS 10.0 for Windows.
Results: The following were defined as risk factors for death at disease onset: male sex (p<0.001, relative risk (RR)=3.5), age >40 at disease onset (p<0.0001, RR=19.9), nephritis (p<0.05, RR=1.6), a reduction of creatinine clearance (p<0.001, RR=1.8), heart disease (p=0.05, RR=1.5), and central nervous system (CNS) disease (p=0.06, RR=1.6). An increase in the SDI of two or more points from the first to the third year of disease was the worst prognostic factor (p<0.0001, RR=7.7). The existence of Ro or nRNP antibodies, or both, was protective (p<0.05, RR =0.1). A low C3 (p<0.01 RR=3.0) and splenomegaly (p<0.01 RR=2.7) at disease onset turned out to be risk factors for ESRD besides a nephritis. In patients with hypertension (p<0.05) and/or high titres of dsDNA antibodies (>70 U/l) (p<0.01) and/or a mean ECLAM score of 4 (p<0.01) in the course of disease, a prevalence of ESRD was recorded in 9% (p<0.05) and 10% (p<0.01), and 8% (p<0.01) v 4% in the whole group. Analysis of risk factors at disease onset for TE identified positive lupus anticoagulant (p=0.17, RR=1.6), cryoglobulins (p<0.05, RR=1.8), and nephritis (p=0.05, RR=1.4), in addition to an age >40 at disease onset.
Conclusions: A subgroup of patients in the Erlangen cohort with a typical clinical and serological phenotype at disease onset that is at high risk for a worse outcome was identified. Identification of these white patients at risk at disease onset will enable treatment to be intensified and thereby possibly prevent or better control late stage manifestations.
- risk factors
- systemic lupus erythematosus
- CNS, central nervous system
- ECLAM, European Consensus Lupus Activity Measurement
- ESRD, end stage renal disease
- RR, relative risk
- SDI, SLICC/ACR damage score data and index
- SLE, systemic lupus erythematosus
- SLICC/ACR, Systemic Lupus International Collaborating Clinics/American College of Rheumatology
- SMR, standardised mortality ratio
- TE, thromboembolic events
Statistics from Altmetric.com
- CNS, central nervous system
- ECLAM, European Consensus Lupus Activity Measurement
- ESRD, end stage renal disease
- RR, relative risk
- SDI, SLICC/ACR damage score data and index
- SLE, systemic lupus erythematosus
- SLICC/ACR, Systemic Lupus International Collaborating Clinics/American College of Rheumatology
- SMR, standardised mortality ratio
- TE, thromboembolic events
Systemic lupus erythematosus (SLE) is the prototype of a systemic autoimmune disorder in which immune complexes or cytotoxic antibodies give rise to tissue damage, often resulting in end organ damage, failure, or death. In the past four decades five year survival in SLE has improved dramatically from <50% to 96.6%, mainly because of more sensitive diagnostic tools, the use of corticosteroids and cytotoxic drugs, especially cyclophosphamide, and better supportive treatments. Standardised mortality ratios (SMRs) for patients with SLE improved from 10.1, as reported in the 1970s to 2.7 in the Erlangen cohort, observed over the past 15 years. This still increased mortality is rarely caused by uncontrolled disease flares, but rather by damage as a consequence of the disease process, side effects of various drugs, and comorbidity. These include chronic vascular disease with atherosclerosis and thromboembolic events, cognitive impairment, osteoporosis with fractures, osteonecrosis, malignancy, and end stage renal disease (ESRD). In addition genetic factors have an increasingly more important role for the frequency and grading of clinical patterns of this complex disease. The negative impact of male sex in SLE as well as HLA associations1 are known, and the importance of Fcγ receptor polymorphisms is becoming evident.2,3 Results from twins and the enormous racial differences in the incidence and course of SLE support the hypothesis of a genetic predisposition.4–6
Until now, only few prognostic factors influencing the course of SLE were identified. By using a database of 338 patients with SLE, documented for at least one to 15 years and including SLICC/ACR damage score data and index (SDI), a validated system for the measurement of chronic damage, starting from disease onset,7 and an activity score8,9 (ECLAM) we were able to identify new risk factors for a severe outcome in SLE, as defined by death, ESRD, and thromboembolic events (TE). Therefore early aggressive treatment might improve the course of disease in patients who have these risk factors, probably preventing or at least controlling late stage manifestations of SLE.
PATIENTS AND METHODS
Study group
Three hundred and thirty eight well documented white German patients with SLE (291 female, 47 male, female:male ratio of 6.2:1), followed up at the Department of Medicine III, University Erlangen-Nuremberg from 1985 to 1999, were selected without respect to disease severity or the stage of disease. All patients fulfilled the 1982 and 1997 revised criteria of the American College of Rheumatology (ACR) for the diagnosis of SLE.10,11 A median of seven visits was recorded for each patient, varying from one to 46 and a maximum of three visits/year. About one third of the patients were part of a consultation group where the diagnosis was made before the first visit.
Demographic, clinical, and laboratory characteristics
Demographic data of each patient were obtained from the official medical record at the time of the first visit until September 1999 and included sex, age, and age at the time of diagnosis. Frequent clinical manifestations (according to Hahn12), haematological and immunological parameters, as well as an activity score (ECLAM)8 and a damage index (SDI)7 were documented for each patient. The presented SDIs are median values at fixed times after 1, 3, 5, . . .years and before death. The major organ involvements were defined according to the criteria of the ACR.11 All abnormalities due to SLE were documented at the time of the first appearance either under our care or from a well documented history and over the entire follow up period.
Statistical analysis
Data analysis was performed with the statistical package SPSS 10.0 for Windows. Median and range were calculated for age at diagnosis and specific variables observed over time, like the ECLAM and SLICC score, because no parametric distribution can be assumed for these variables. Kaplan-Meier curves were estimated for time until death, ESRD, and TE in subgroups defined by potential prognostic factors.13,14 Differences between subgroup-specific Kaplan-Meier estimates were assessed using the log rank test.15 To test the null hypothesis that categorial variables such as clinical and serological parameters are equally distributed between patients with and without the outcome variables as death, ESRD, and TE, a two tailed Pearson's χ2 test was applied. A p value <0.05 resulting from any of these statistical tests was considered significant. Multivariable Cox regression models were analysed to scrutinise the possible role of demographic, genetic, and clinical measures of SLE for the outcome criteria death, ESRD, and TE. Sex and age at disease onset were forced into all models, while the other parameters were sequentially added to and removed from the model depending on their p value being <0.1. The strength of the association between these prognostic variables and the outcomes of interest (death, ESRD, and TE) was estimated by the adjusted rate ratios (RR; RR>1: positive association; RR=1: no influence; RR<1: protective) derived from the final model.16
RESULTS
Median age at first diagnosis was 32.6 years, median disease duration 7.8 years, and median observation period 5.4 years. The median ECLAM score was 3.1, the median SDI 2 after one and five years and 3 after 10 and 15 years of disease. Skin manifestations, including malar rash, discoid rash, photosensitivity, and oral ulcers, were recognised in 67%, 44%, 72%, and 33% of our SLE cohort in the course of disease; arthritis was seen in 71%, serositis in 30%, nephritis in 42%, neurological disorder in 21%, haematological and immunological abnormalities in 97% and 96% respectively, and antinuclear antibodies were present in 96% of our patients in the course of disease.
At the end of the observation period 35/338 patients had died. The SMR was 2.7, five year survival was 96.6% (fig 1). The most common reasons for death were cardiovascular (37%) and infectious diseases (29%). The proportion of men who died was 23% compared with 8% of women (table 1). Twenty per cent of patients with late onset lupus (>40 years) died compared with 2% in the group aged <25 years (table 1). A population based control of age and sex adjusted SMR reconfirmed a higher mortality rate in this subgroup of patients.
Older age at first diagnosis and male sex as risk factors for a higher mortality
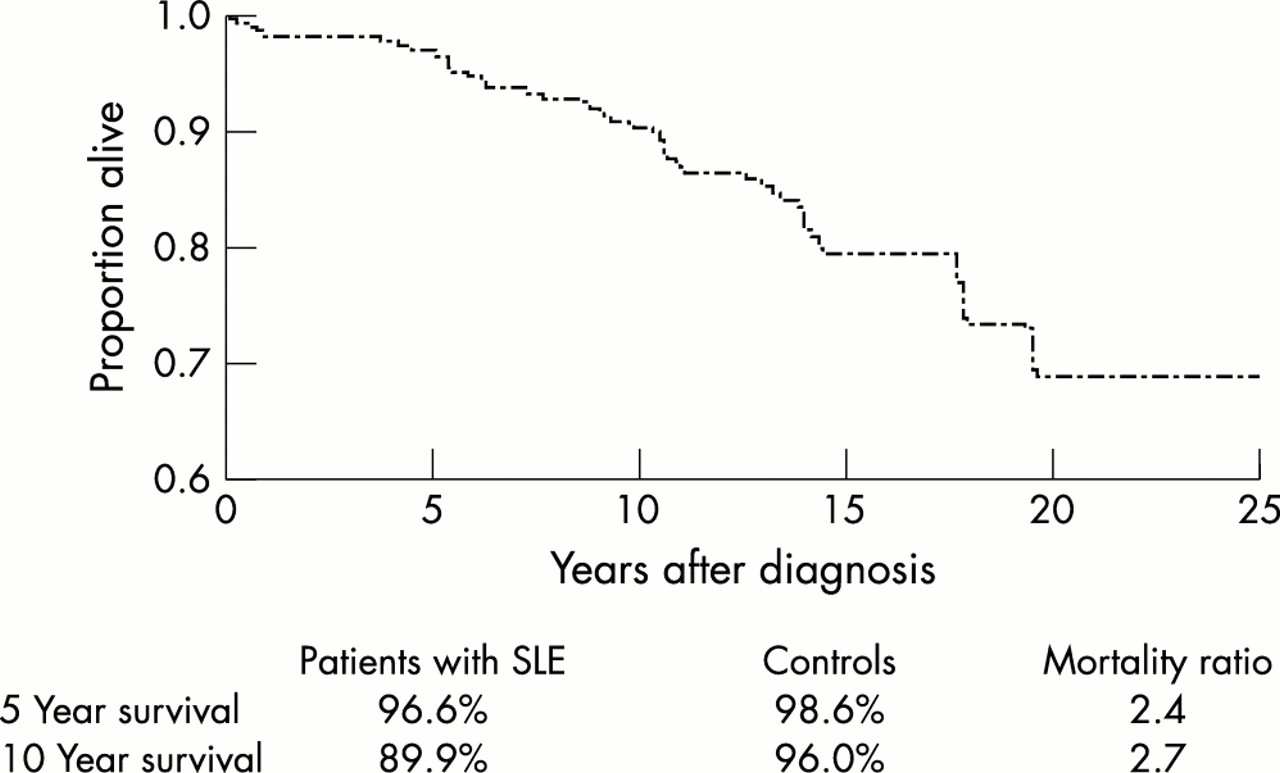
Survival in 338 patients with SLE from the Erlangen cohort. Standardised mortality ratio (SMR) as compared with the German population (SMR: ratio of lupus patients who had died divided by the ratio of the German control population who had died, age and sex adjusted).
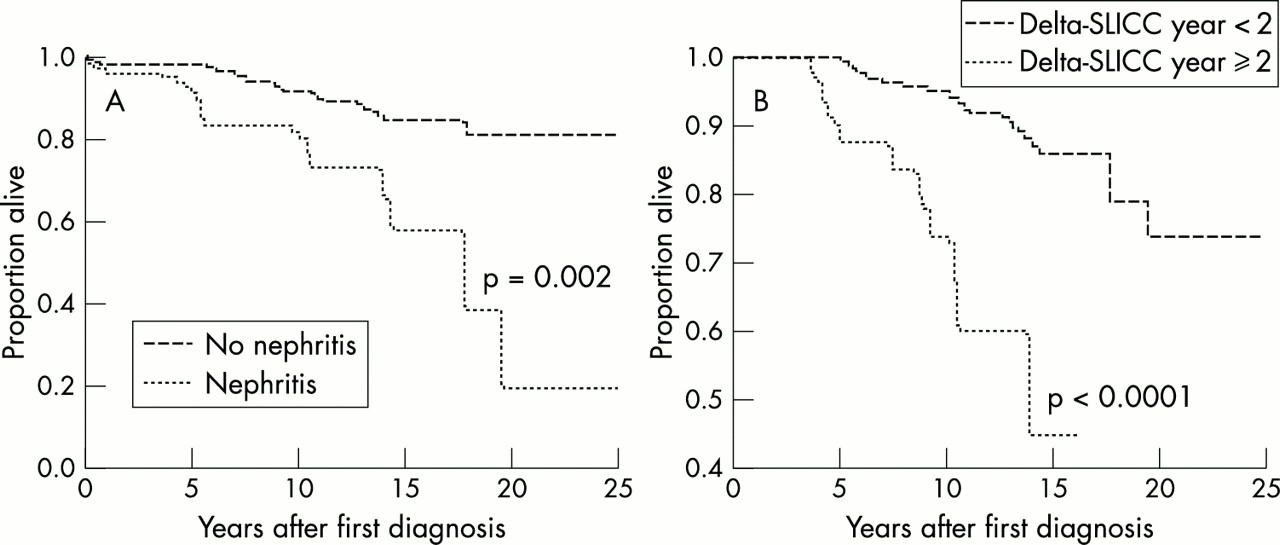
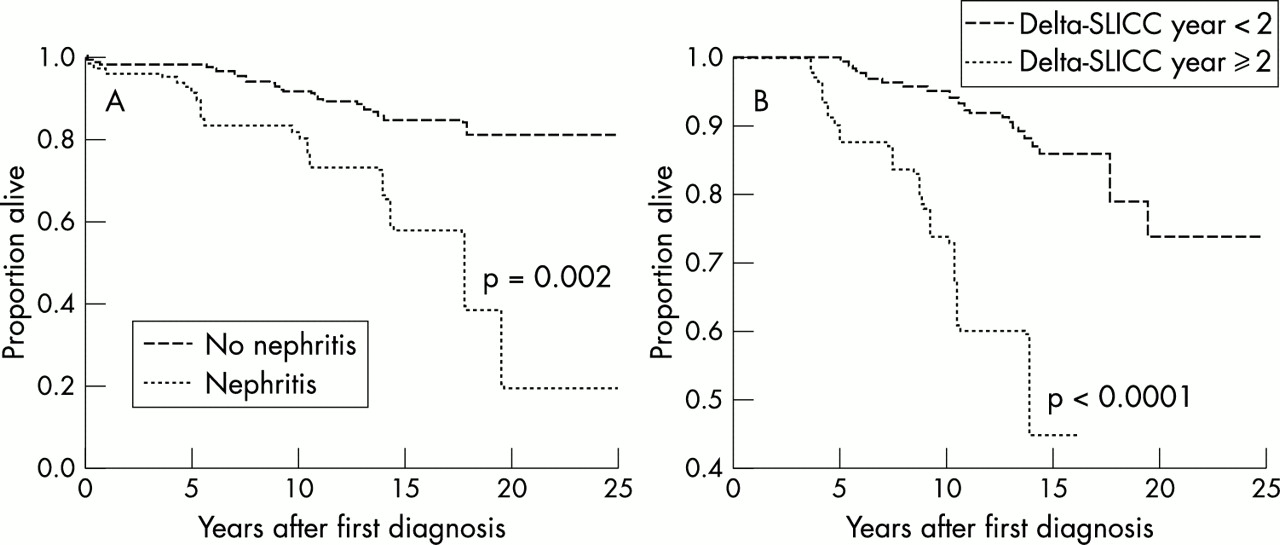
The most important risk factors existing at disease onset were, besides male sex and older age, a reduced creatinine clearance (RR=1.8), nephritis (RR=1.6), heart disease (RR=1.5), and central nervous system (CNS) disease (RR=1.6) (table 2, fig 2A). In a stepwise approach, including the SDI in this multivariable analysis, an increase of two or more points of SDI from the first to the third year of disease turned out to be another important prognostic factor for mortality (RR=7.7, 95% CI 3.3 to 18.6, p<0.0001) (fig 2B). None of 38 and 32 patients with positive Ro or nRNP antibodies at disease onset died during the observation period (p<0.05). Thus Ro or nRNP antibodies may be protective.
Risk factors at disease onset for a higher mortality in patients with SLE
{kind=link}
{kind=link}
Kaplan-Meier analysis of mortality in SLE in association with (A) nephritis at disease onset and (B) an increase in SDI of two or more points between year 1 and 3 after disease onset. The difference between the groups was statistically assessed by the log rank test; p value indicates level of significance.
We found no significant sex differences in 4% of patients with ESRD in the whole SLE cohort, however, a low C3 (RR=3.0, 95% CI 1.5 to 6.0, p<0.01) and splenomegaly (RR=2.7, 95% CI 1.3 to 5.5, p<0.01) at disease onset turned out to be risk factors besides a nephritis in multivariable analyses, manifesting in the first year of disease (table 3). In patients with hypertension or high titres of dsDNA antibodies (>70 U/l) or a mean ECLAM score of 4 in the course of disease a prevalence of ESRD was recorded in 9%, 10% (p<0.01), and 8% (p<0.01) v 4% in the whole group.
Risk factors at disease onset for ESRD
Men had a slightly increased risk for TE (RR=1.5,0.7–3.1, p=0.06), which occurred in 26.0% of the Erlangen cohort. The group aged <25 years at disease onset had more TE in than the middle aged group, but less than the patients aged >40 at disease onset, who had a significantly increased risk for TE (RR=2.2, 95% CI 1.1 to 4.6, p<0.05). Analysing additional risk factors for TE in multivariable analyses, we found that 57% of patients with a positive lupus anticoagulant at disease onset had a TE (RR=1.6, 95% CI 0.8 to 3.1, p=0.17), 43% of patients with cryoglobulins (RR=1.8, 95% CI 1.1 to 3.0, p<0.05), and 34% of patients with nephritis (RR=1.4, 95% CI 1.0 to 2.0, p=0.05). In these cohorts TE occurred earlier than in the whole SLE cohort (table 4).
Risk factors at disease onset for thromboembolic events
DISCUSSION
Based on an improved survival in SLE due to earlier diagnosis and improved treatments,17–19 we are witnessing increasing numbers of patients with late stage lupus with a high comorbidity, related in part to treatment. Studies from the 1990s report 10 year survival rates of over 90%,20,21 89.9% (Erlangen cohort), and 83%.22 Despite this high life expectancy, the SMR in the Erlangen cohort was 2.7, which is comparable with the SMR of 3.3 in the Pittsburgh cohort17 and slightly better than the 4.6 from Denmark in 1999.23
Reasons for death are rarely due to uncontrolled episodes of SLE but rather attributable to treatment and comorbidity, like an accelerated atherosclerosis.22,24 Thus, for example, 37.1% in the Erlangen cohort, 45.7% in a Hungarian cohort, and 26.2% in a Danish cohort died from cardiovascular complications.23,25 These observations are underlined by epidemiological data that demonstrate a fivefold increased risk for myocardial infarction in SLE which reaches a 52-fold increased risk in female patients with SLE below the age of 45.26,27 Ten of our 13 German patients who died from cardiovascular reasons were above 40 years when the diagnosis was established, similar to observations made in Hungary.25 In contrast with these European observations, a cohort from Southern China and Korea did not have a single death as a consequence of a cardiovascular event,28,29 again demonstrating the great ethnic differences in the course of the disease. Sixty per cent of deaths in the Erlangen cohort occurred during the first 10 years of disease. Therefore risk factors and protective factors for severe outcome criteria like death, ESRD, or thromboembolic events, are highly important for determining the course of disease.
As a genetic risk factor for a higher mortality we identified the male sex (RR=3.5), similar to the Hungarian cohort (RR=2.5) and other reports.25,30–34 The higher mortality in men as seen in this German cohort might be related to a higher age at first diagnosis and a higher prevalence of factors that negatively influence the outcome in SLE—for example, a nephritis (51.1% v 37.4%), heart disease (29.8 v 14.8%), and CNS disease (34.0 v 24.0%).30 When the complete cohort of our patients with SLE was analysed, renal (RR=1.6), heart (RR=1.5) or CNS involvement (RR=1.6) at disease onset could be defined as risk factors for a higher mortality both in the Erlangen group and a Spanish cohort,31 and the European working party on SLE which reported a reduced five year survival of 92% in patients with SLE with nephritis at disease onset.35 In a report from Denmark, azotaemia, CNS involvement, and myocarditis in the course of disease were risk factors for death.36 These data are not confirmed in a Hungarian cohort of patients with SLE25; again genetic differences may account for the different clinical observations. A higher age at first diagnosis was associated with a higher mortality (RR= 7.4–19.9) in the Erlangen cohort, although a late stage lupus is usually less aggressive25,34,37 and the prevalence of nephritis is lower (45.8 v 36.4% in patients above 40 years of age). Obviously, naturally increasing mortality and accumulated damage, a higher incidence of complications, and a multimodal therapeutic regimen may be at least some of the reasons for a higher mortality in this specific subgroup of patients of the Erlangen cohort.
The increasingly observed chronic and irreversible damage in longstanding SLE can be identified for the individual patient by the SDI.1 In our cohort, symptoms like thromboembolic events, neuropathies, cognitive impairment, cataract, premature gonadal failure, osteonecrosis, osteoporosis with fractures, and neoplasms strongly influenced the prognosis of the individual patient. Similar results were published by Swaak et al in a multicentric cohort of 110 patients with SLE with a disease duration of more than 10 years.38
When a subgroup of the Erlangen cohort with an increase in the SDI of two or more points between the first and the third year of disease was examined, it was found that this increase was associated with a higher mortality. In this specific subgroup 21% died as compared with 10% in the whole cohort. Ten year survival was 73% compared with 90% in the whole cohort (p<0.0001, RR=7.7), which was similar in a multicentric, multiethnic heterogeneous group of patients with SLE from America.39 A study from Great Britain showed the predictive value of pulmonary damage for a higher 10 year mortality.40
When the prevalence of nephritis in the course of the disease was examined it was found that 42% of the Erlangen cohort had a kidney disease, which is in accord with the results from other European groups (30%41 and 38%42); the high prevalence of nephritis in patients with SLE underlines the importance of this particular organ involvement in SLE as a prognostic marker. Of our male patients, 51% had a nephritis compared with a 37% prevalence in women, a tendency which was also observed by Ward and Studenski.30
In our cohort the prevalence of ESRD was found to be 4% as compared with 13% in patients with lupus nephritis at the onset of disease. Nephritis was defined according to the ACR criteria; renal biopsies were only done in a subgroup of patients. ESRD was found by Derksen et al in 14.3% of patients with biopsy proven lupus nephritis.43 Stone reported about 10% of ESRD within all patients with SLE.44 Derksen et al reported a higher prevalence of ESRD in men with lupus nephritis but not in men of the whole SLE cohort,43 as we also found. It is noteworthy, however, that the factor “male sex”, adjusted for age, remains a risk factor to develop ESRD besides hypertension, cardiac disease, and high titre (>70 U/l) dsDNA antibodies in the course of disease in our subgroup of patients with lupus nephritis. Abraham et al, also, identified hypertension and a extensive proteinuria in the course of disease as risk factors for the development of ESRD in 29 patients with SLE with diffuse proliferative glomerulonephritis. None of the other patients without hypertension or proteinuria developed an ESRD (p<0.001).45 An ECLAM score of 4 was a strong predictor for an ESRD (RR=9.5), as was proteinuria lasting for more than six months (RR=3.2) and an active urinary sediment (RR=3.5). These data are in accord with the results of 94 Danish patients with lupus nephritis.46 We looked at the incidence of splenomegaly and low C3 at disease onset in the Erlangen cohort, and defined both variables as predictive for the development of an ESRD (RR=2.7, RR=3.0), similar to a report of Chinese patients.47
Thromboembolic events are highly important for morbidity and mortality in SLE. In our cohort, 7% had a myocardial infarction, 10% a stroke, 4% pulmonary embolism, and 22% a deep vein thrombosis after a disease duration of 10 years or more. These events were slightly more common in male patients (RR=1.5) and patients above 40 years than in patients below 25 years at first diagnosis (RR=2.2), findings which are in accordance with data published by Petri.48 In addition, Petri found that antiphospholipid antibodies, renal insufficiency, and raised levels of homocysteine were risk factors for coronary artery disease; homocysteine was not tested routinely in all our patients. However, the most important risk factors at disease onset for developing a TE in the Erlangen cohort were again nephritis (RR=1.4), cryoglobulins (RR=1.8), and a positive lupus anticoagulant (RR=1.6); the last of these has been shown to be a more important predictor for TE compared with other assays measuring antiphospholipid antibodies.49
The importance of cardiovascular disease in patients with SLE becomes evident. As mentioned above, heart disease in the first year after diagnosis is one of the most important risk factors for a higher mortality in multivariable analyses. In the Erlangen cohort 17% had angina after ≥10 years of SLE, 7% had a myocardial infarction. Patients of the Hopkins cohort and a European cohort did show evidence for a coronary artery disease in 9% and 8%, respectively.38,48 We found that hypertension was a very important risk factor for cardiovascular events in 21% of patients after five years and 44% after 10 years of disease, comparable with the results of Swaak et al.38 Eighteen per cent of our patients are smokers, 15% have raised levels of cholesterol, all known risk factors for the development of cardiovascular diseases. As a potential additional factor for a premature atherosclerosis, 14% of the Erlangen cohort have a gonadal failure before the age of 40. Mok et al identified age >30 years and a cumulative dosage of cyclophosphamide as risk factors for a premature ovarian failure.50
The data reported from the Erlangen cohort may help to improve the possibility of identifying white patients with SLE who will have a severe outcome of the disease. By these means we can better stratify individual patients and provide the best therapeutic regimen, including early aggressive immunosuppressive drugs.
Acknowledgments
KM received a “Grant for Women in Science (HSP III)” from the University Erlangen-Nuremberg.