Article Text

Abstract
Infliximab is a chimeric anti-tumour necrosis factor α (TNFα) monoclonal antibody with high affinity and binding specificity for human TNFα. Results from several well designed, controlled clinical trials show repeated infusions of infliximab with concomitant methotrexate (MTX) treatment can reduce the signs and symptoms of rheumatoid arthritis (RA). This combination of infliximab and MTX also slows the radiological progression of joint damage, decreases functional disability, and improves qualify of life. These remarkably positive results have led to the investigation of infliximab treatment for other rheumatic diseases. Recently, controlled studies have shown treatment with infliximab can benefit patients with active spondyloarthropathy. TNFα has fast become an important therapeutic target in rheumatology.
- infliximab
- ankylosing spondylitis
- tumour necrosis factor α
- RA, rheumatoid arthritis
- MTX, methotrexate
- TNFα, tumour necrosis factor α
- CRP, C reactive protein
Statistics from Altmetric.com
Infliximab, a tumour necrosis factor α (TNFα) inhibitor, has emerged as a key treatment for rheumatoid arthritis (RA) and other rheumatic diseases. Working at the Kennedy Institute of Rheumatology in London, Ravinder Maini and Marc Feldmann pioneered the early development of infliximab. Since beginning their research together over a decade ago, considerable progress has been made in our understanding of TNFα as an inflammatory mediator and the clinical utility of anti-cytokines as a therapeutic strategy. Infliximab is now widely used throughout the world for the treatment of RA and a growing list of other inflammatory arthropathies. In this article, I will review the clinical and radiological efficacy of infliximab treatment for RA as well as the recent studies using this agent for the treatment of ankylosing spondylitis and psoriatic arthritis.
Infliximab was derived from a murine antibody against human TNFα. However, murine monoclonal antibodies are unattractive as therapeutic agents because of their immunogenicity and unfavourable pharmacokinetics. To decrease immunogenicity and improve the pharmacokinetic profile, the murine antibody was engineered as a chimeric anti-TNFα antibody with a predominance of human amino acid sequences.1 The murine antigen binding regions were retained in the chimeric antibody, but the constant regions from the mouse antibody were replaced with the corresponding parts of a human IgG1 molecule. The chimeric anti-TNF antibody has been shown to bind soluble and transmembrane TNFα with high specificity and affinity (Ka=1010/M), and forms a stable complex preventing association of TNFα with its receptor.
RHEUMATOID ARTHRITIS
Initial studies had shown TNFα as well as other proinflammatory cytokines were abundantly expressed in the synovial tissue of patients with RA. Many investigators were sceptical in the beginning of the anti-TNFα approach, or blocking a lone proinflammatory cytokine. In theory, interleukin 1 and other proinflammatory cytokines could perpetuate the pathological process and compensate for the down regulation of TNFα activity. In 1993, an open label study of infliximab treatment for RA afforded the first inklings TNFα was a viable therapeutic target.2 Next, the results of a randomised, placebo controlled trial provided solid evidence for the beneficial effects of infliximab on RA activity. In this trial, 73 patients with active RA were randomly allocated to receive an infusion of placebo or 1 mg/kg or 10 mg/kg of infliximab.3 Treatment with infliximab produced a rapid and significant reduction in the number of tender and swollen joints and concentrations of serum C reactive protein (CRP). The best responses were obtained with the 10 mg/kg dose. Not unexpectedly, a single infliximab infusion was inadequate to produce a sustained response. Repeated cycles of treatment were later found to maintain clinical improvement if given frequently enough.4 Some patients developed serum antibodies to the foreign antigen binding sequences of infliximab, raising questions about the possible long term efficacy of prolonged treatment.
The clinical efficacy of infliximab treatment for RA was subsequently investigated in a 26 week, double blind placebo controlled, dose ranging study.5 Eligible patients must have been taking methotrexate (MTX) 7.5–15 mg/wk for at least six months before study entry. The dose of MTX was fixed at 7.5 mg/wk for four weeks before randomisation. The 101 patients were randomly assigned in this study to receive placebo or infliximab 1, 3, or 10 mg/kg at weeks 0, 2, 6, and 14, with or without MTX 7.5 mg/week. A control group received placebo infusions and MTX 7.5 mg/week. At a dose of 1 mg/kg, infliximab was more effective with MTX than without MTX treatment, with the former combination producing a higher rate and duration of treatment response. On the other hand, similar response rates were observed for the infliximab 3 and 10 mg/kg dose groups at week 16, with or without MTX. The Paulus response rates approached 60% for all of these groups. By week 26, the responses trended lower for the patients taking infliximab alone compared with those receiving infliximab and MTX.
In this same study, serum antibodies to infliximab were detected in 17.4% of all infliximab treated patients.5 However, higher doses of infliximab and concomitant MTX treatment were associated with lower incidences of serum antibodies to infliximab. In fact, serum antibodies to infliximab were undetectable in the infliximab 10 mg/kg plus MTX group. Pharmacokinetic analysis showed blood concentrations of infliximab decreased more rapidly in the 1 mg/kg group than the 3 mg/kg and 10 mg/kg groups. At the lowest dose, the clearance of infliximab may have been speeded by circulating antibodies to infliximab determinants. These studies identified 3 mg/kg and 10 mg/kg as potentially the most effective doses and suggested infliximab treatment would be more effective in combination with MTX than alone. Findings from another randomised, placebo controlled trial of infliximab tended to support these conclusions.6
The clinical and radiological efficacy of repeated infusions of infliximab was further evaluated in the Anti-TNF Trial in RA with Concomitant Therapy (ATTRACT).7,8 To be eligible, patients must have had active RA despite taking at least 12.5 mg/wk of MTX treatment. The study enrolled 428 eligible patients who were randomly allocated to placebo or 3 mg/kg or 10 mg/kg of infliximab every four or eight weeks. All patients received infusions of placebo or infliximab at week 0, 2, and 6 followed by infusions every four or eight weeks. The MTX dose was kept constant during the trial unless it had to be reduced for possible MTX toxicity. The study population had advanced disease, as evidenced by a mean duration of disease ranging from 9–12 years across the five treatment groups. Infliximab treatment was efficacious at all doses compared with placebo.7 The ACR20 response rates rose quickly and reached 50%–60% by the 30 week end point. Significantly more patients in the infliximab treatment groups also achieved ACR50 (26%–31% v 5%) or ACR70 (8%–18% v 0%) responses than those in the MTX-placebo group. The tender and swollen joint counts, pain scores, and serum concentrations of CRP improved by comparable values. The ACR response rates were generally sustained through one year of treatment.8 However, at week 54, the ACR50 response rate for the 3 mg/kg every eight week group was only 21%. While this lowest dose group had a significantly higher ACR50 response rate than the placebo group (8%), it had notably less clinical efficacy than the other infliximab doses with ACR50 response rates of 34%, 38%, and 39%.
In the midst of ATTRACT, a decision was made to extend the trial from 54 to 102 weeks. As a result, some of the patients in the study had a several month gap in their experimental treatment at this midway point. During the second year, the trial was unblinded after analysis of the radiographic data from week 54 had shown infliximab treatment significantly protected against the development of joint damage. Therefore, some of the patients did not complete the study under conditions of blinding.
The radiologicial analysis was performed using rigorous methodology. The amount of joint damage was determined using the van der Heijde modification of the Sharp score.10 This method quantifies the extent of bone erosions and joint space narrowing for 44 and 40 joints, respectively. Total scores with this scoring system range from 0–440, with higher scores denoting greater damage. Two experienced readers scored each radiograph and were blinded to the order of the films. At baseline, the total Sharp scores were 67–82 across treatment groups, indicative of moderately severe joint damage.
In the MTX plus placebo control group, the total Sharp score increased from baseline to week 54 by a mean (SD) of 7.0 (10.3). Thus, partial responders to MTX treatment accumulated joint damage over time. All doses of infliximab significantly decreased the radiological progression of joint damage after one year of treatment (54%).8 The mean (SD) change in the total Sharp score for the 3 mg/kg every 8 week, 3 mg/kg every 4 week, 10 mg/kg every 8 week, and 10 mg/kg every 4 week groups, were 1.3 (6.0), 1.6 (8.5), 0.2 (3.6), and −0.7 (3.8), respectively. Significant improvements were noted for the erosion and joint space narrowing components of the total score, implying infliximab treatment slows the progression of both subchondral bone and cartilage injury. In a subgroup analysis, infliximab treatment arms seemed to decrease radiological progression of joint damage for both ACR20 responders and non-responders. Although this finding suggests a TNFα inhibitor such as infliximab can inhibit joint damage independently of its anti-inflammatory effects, at least some of the non-responders by ACR20 criteria have been found to improve in some clinical aspects. Regardless, the results from this trial imply an important role for TNFα in mediating cartilage and bone destruction. Preliminary analysis of data from the 102 week end point also has shown that infliximab treatment produces significant improvements in functional disability and quality of life.9 The potential immunogenicity of chronic infliximab treatment remains a subject of investigation, but thus far has not been shown to impact clinical efficacy in a significant way.
As alluded to above, a comparison of response rates across infliximab treatment groups in ATTRACT suggests a dose response at the lower end of the dosing range. In clinical practice, infliximab treatment is usually begun at a dose of 3 mg/kg every eight weeks. However, the product labelling does allow for dosing flexibility within the 3 mg/kg–10 mg/kg every four to eight week range. Anecdotal observations indicate some patients receiving infliximab at a dose of 3 mg/kg every eight weeks experience a disease flare at the end of the eight week interval, prompting empirical boosts in the infliximab dose to improve treatment response. There have been no controlled studies testing if such an incremental dosing strategy is more effective than keeping the dose stable at 3 mg/kg every eight weeks.
A post hoc analysis of data from ATTRACT has provided evidence for a significant relation between the extent of clinical improvement and trough serum concentrations of infliximab.11 For some patients, optimal suppression of disease activity may require sustained inhibition of TNFα activity. About 25% of patients in the 3 mg/kg every eight week group had no detectable infliximab in their serum immediately before the next dose. This group tended to have a lower proportion of ACR20 responders compared with patients with detectable trough serum concentrations of infliximab. However, for the individual patient, a trough level would not probably be a reliable guide for making a dosage adjustment because of the imprecise relation between trough serum levels and the extent of clinical response. In contrast, pharmacokinetic modelling can provide valuable information for empiric dosing changes. Based on the ATTRACT data, models predict that shortening the interval between infusions from eight to six weeks produces higher trough serum concentrations of infliximab than increasing the dose by 100 mg (for example, the amount in a vial of drug).11 For the patient with a suboptimal response, the preferred strategy may be to shorten the treatment interval rather than increasing the infliximab dose.
Additional studies are in progress to learn more about the role of infliximab treatment in this setting. Will patients with early disease benefit from starting infliximab treatment (or other TNFα inhibitor) with MTX soon after disease onset? Will treatment effectiveness wane over time because of the production of antibodies to infliximab? Can sustained infliximab treatment lead to healing of bone erosions? Future research promises to shed light on the most appropriate niche for infliximab treatment in this setting.
Ankylosing spondylitis and psoriatic arthritis
Like for RA, infliximab has been shown in several studies to potently reduce the signs and symptoms of ankylosing spondylitis. New treatments for ankylosing spondylitis are sorely needed because of the limited options at present. The potential clinical efficacy of infliximab therapy for ankylosing spondylitis was examined in an open label study of 21 patients with active spondyloarthropathy (ankylosing spondylitis, 10; psoriatic arthritis, 9; undifferentiated spondyloarthropathy, 2). The study showed that infliximab 5 mg/kg given at weeks 0, 2, and 6 could produced substantial improvements in several different measures of disease activity.12 Moreover, a maintenance regimen of 5 mg/kg every 14 weeks was able to maintain improvement in some cases, although many patients developed recurrent symptoms before their next treatment.13 These findings were confirmed in a 12 week, randomised, double blind, placebo controlled trial of infliximab involving 40 patients with active spondyloarthropathy.14 Eligible patients were randomly allocated in this trial to receive placebo or infliximab 5 mg/kg at week 0, 2, and 6. The study population included 19 patients with ankylosing spondylitis, 18 patients with psoriatic arthritis, and 3 patients with an undifferentiated spondyloarthropathy. Improvements were noted in global assessments for pain, number of tender joints, axial assessments for pain and mobility, and functional disability.
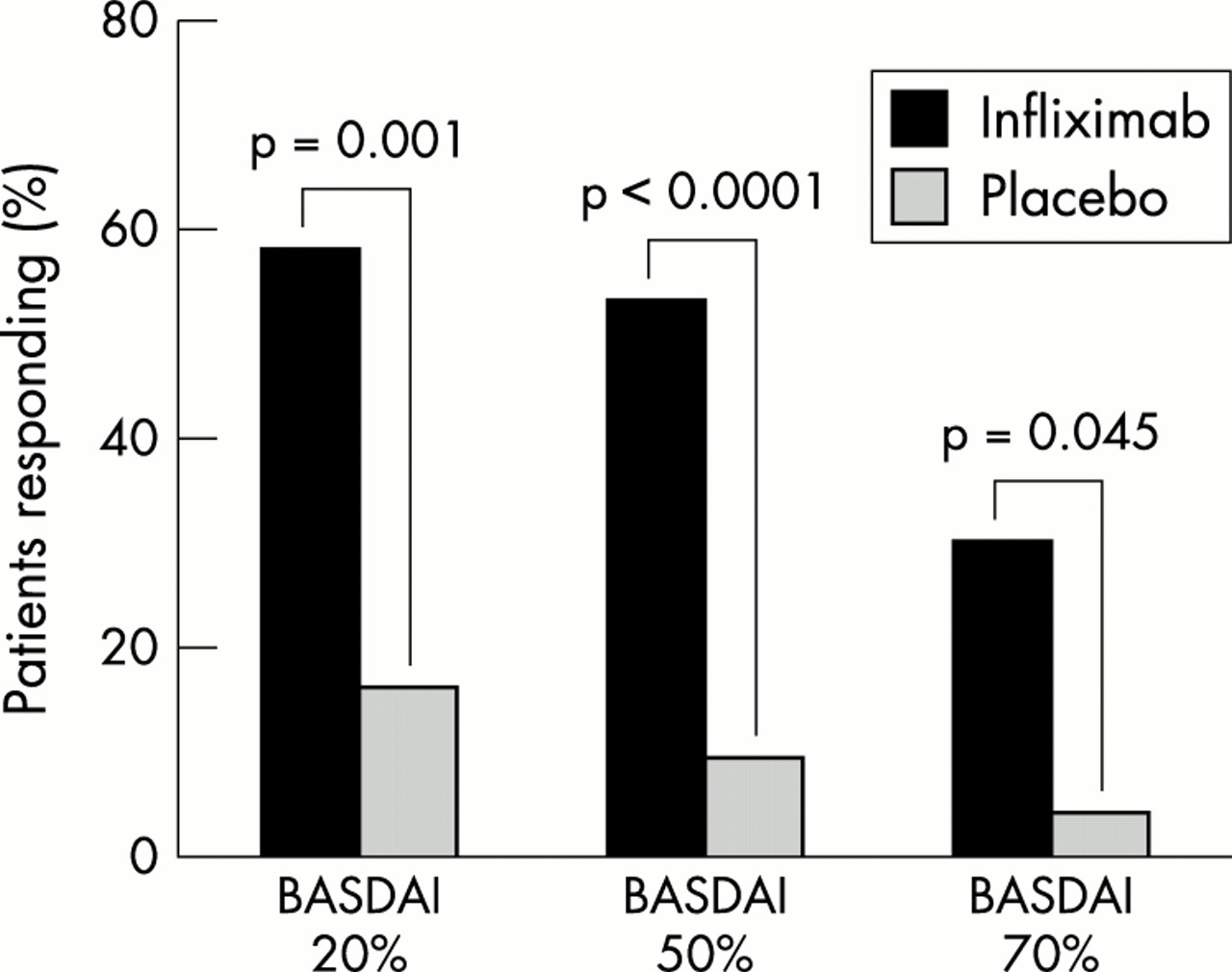
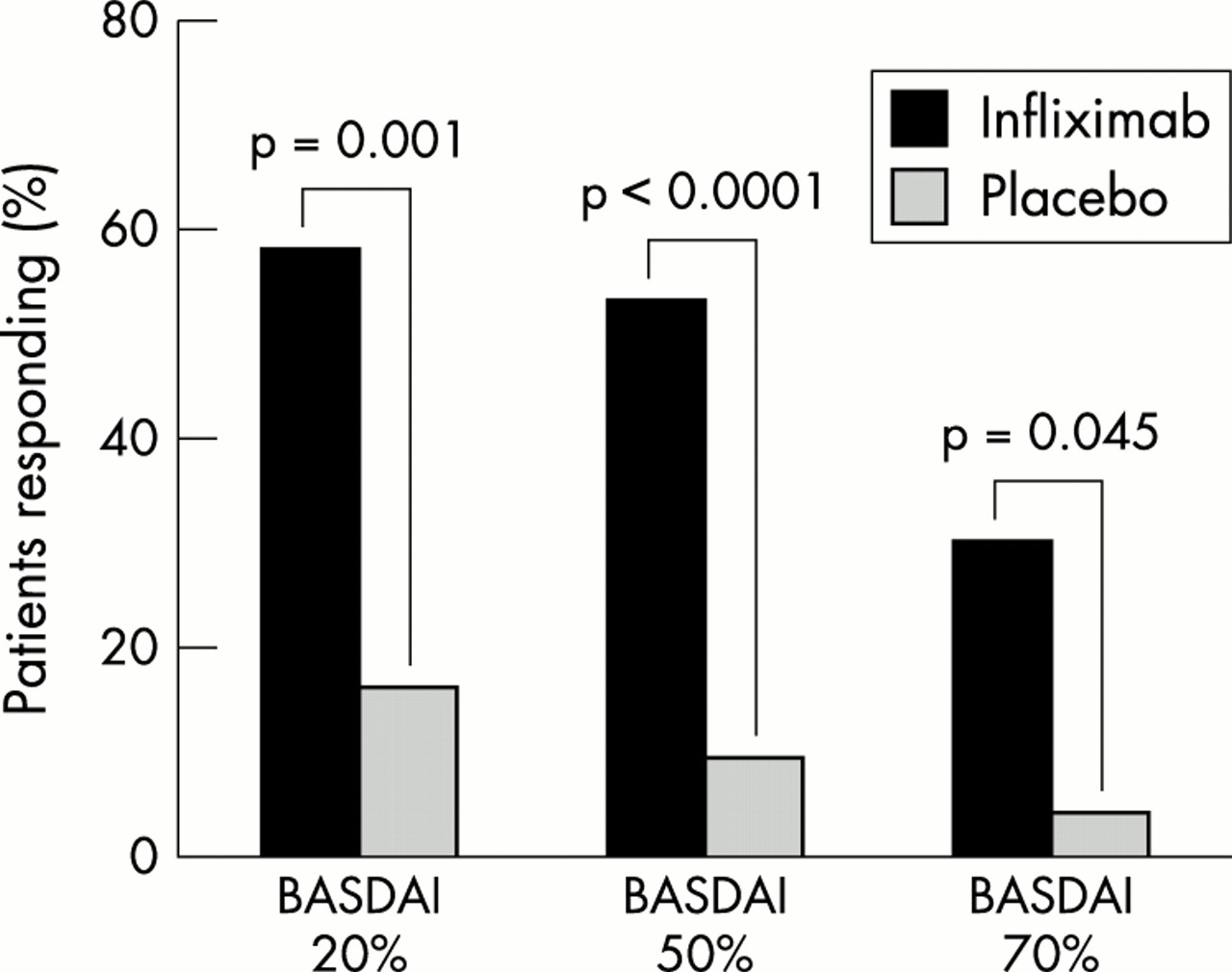
After encouraging results from an open label study,15 Braun and coworkers16 performed a similar 12 week, randomised, double blind, placebo controlled trial of infliximab treatment for patients with ankylosing spondylitis. In this trial, 70 eligible patients were randomised to receive either placebo or infliximab 5 mg/kg at weeks 0, 2, and 6. Disease activity was evaluated using validated measures recommended by the ankylosing spondylitis working group.17 An important measure of disease activity is the Bath ankylosing spondylitis disease activity index (BASDAI), a questionnaire evaluating disease activity related to fatigue, spinal pain, peripheral arthritis, enthesitis, and morning stiffness. Other measures included the Bath ankylosing spondylitis functional index (BASFI), and the Bath ankylosing spondylitis metrology index (BASMI), which assesses the mobility of the spine and hip. Predetermined criteria were set in this study to define 20%, 50%, and 70% levels of improvement.16 Infliximab treatment was associated with significant improvement in all disease measures compared with placebo (fig 1). Together, these two controlled studies show infliximab therapy provides substantial short-term clinical benefit for patients with ankylosing spondylitis. Studies are in progress to determine the long term efficacy of infliximab treatment for this indication.
{kind=link}
Clinical improvement of ankylosing spondylitis with infliximab treatment. Results from a randomised, double blind, placebo controlled trial. Eligible patients were treated with either infusions of placebo or infliximab 5 mg/kg at week 0, 2, and 6. The primary outcomes were determined at week 12. See text for description of the BASDAI outcome measure. Statistical differences in response rates between treatment groups were determined by Fisher’s exact test. Data from Braun et al.16
The experience with infliximab treatment for psoriatic arthritis has been relatively limited in comparison with that for ankylosing spondylitis. In a small pilot study, treatment with infliximab was associated with improvement in both the joint and skin manifestations.18 Also, in a small, randomised, placebo controlled trial, infliximab 5 mg/kg and 10 mg/kg given at weeks 0, 2, and 6 each produced significant clearing of psoriatic skin lesions compared with placebo, with a median time to response of four weeks.19 As etanercept treatment is beneficial for psoriatic arthritis,20 infliximab will probably show similar favourable effects in the treatment of this condition.
CONCLUSIONS
The clinical success of infliximab treatment for RA and certain other rheumatic diseases validates TNFα as a crucial mediator of inflammatory disease mechanisms. However, the answer is not so simple because more than one quarter of patients with RA do not respond adequately to TNFα block. The reasons behind this differential response are of interest. A possible explanation is the heterogeneity of RA created by a vast array of intermingling genetic and environmental factors. Future research will aim at dissecting these factors and their relative contribution to individual expression of disease and response to treatment.