Article Text

Abstract
Giant cell arteritis (GCA) is the most common form of systemic vasculitis in adults. Patients usually present with headache and visual symptoms, and have an elevated erythrocyte sedimentation rate. It has been reported that 3–4% of patients with GCA develop ischemic events secondary to vertebral artery stenosis or occlusion. The mainstay of therapy of GCA is high dose steroid and/or methotrexate. A case is described of a patient who initially presented with intermittent double vision, mild headache and unremarkable MRI and MR angiography of the head and neck. The patient was diagnosed and treated for ocular myasthenia. The patient was readmitted 2 months later with imbalance and worsening headache, and workup suggested bilateral cerebellar infarction, complete occlusion of the left vertebral artery and a high grade stenosis of the right vertebral artery. Erythrocyte sedimentation rate and C reactive protein were elevated. Temporal artery biopsy demonstrated changes consistent with GCA. During the course of the treatment with corticosteroids and immunosuppressant, the patient developed dysarthria, left facial droop and left hemiplegia, and was found to have complete occlusion of both vertebral arteries. The patient was emergently taken for revascularization of the occluded segment using angioplasty and stent placement. The patient had significant improvement of neurological symptoms within 3 days after the procedure and continued to improve during hospitalization. Endovascular treatment of vasculitis affecting the intracranial vessels is not yet established. Our experience with successful treatment of complete occlusion of the vertebral artery secondary to GCA using endovascular intracranial angioplasty and stent placement is reported.
Statistics from Altmetric.com
Introduction
Giant cell arteritis (GCA) is a granulomatous vasculitis of large and medium sized arteries. It predominantly affects the superficial temporal arteries but other blood vessels, such as the ascending aorta, its branches and the vertebral arteries, may be affected.1–3 Involvement of extradural internal carotid or vertebral arteries is usually responsible for acute ischemic strokes. Ischemic complications are a result of either thrombosis or severe occlusion with subsequent reduction of cerebral blood flow.4 5 The management of GCA mainly involves medical treatment, such as high dose corticosteroids and immunosuppressants like methotrexate, which can be used as a steroid sparing agent.2 6 Endovascular angioplasty has been considered as an alternative or additional treatment in vasculitis such as Takayasu's arteritis and Kawasaki's disease as they involve large sized proximal blood vessels, especially the brachiocephalic artery or subclavian artery.6 7 A favorable outcome after angioplasty and stenting for vasculitis involving peripheral and cerebral arteries secondary to GCA has been reported in only three case reports.8–10
We present a case of a patient who was initially diagnosed with ocular myasthenia, developed progressive bilateral cerebellar infarction and bilateral vertebral artery occlusion despite being on high dose steroid and an immunosuppressant. Due to the acute onset of left hemiplegia, the patient was emergently treated with intracranial angioplasty and stent placement with complete recanalization of the vertebral artery and reversal of the symptoms.
Case report
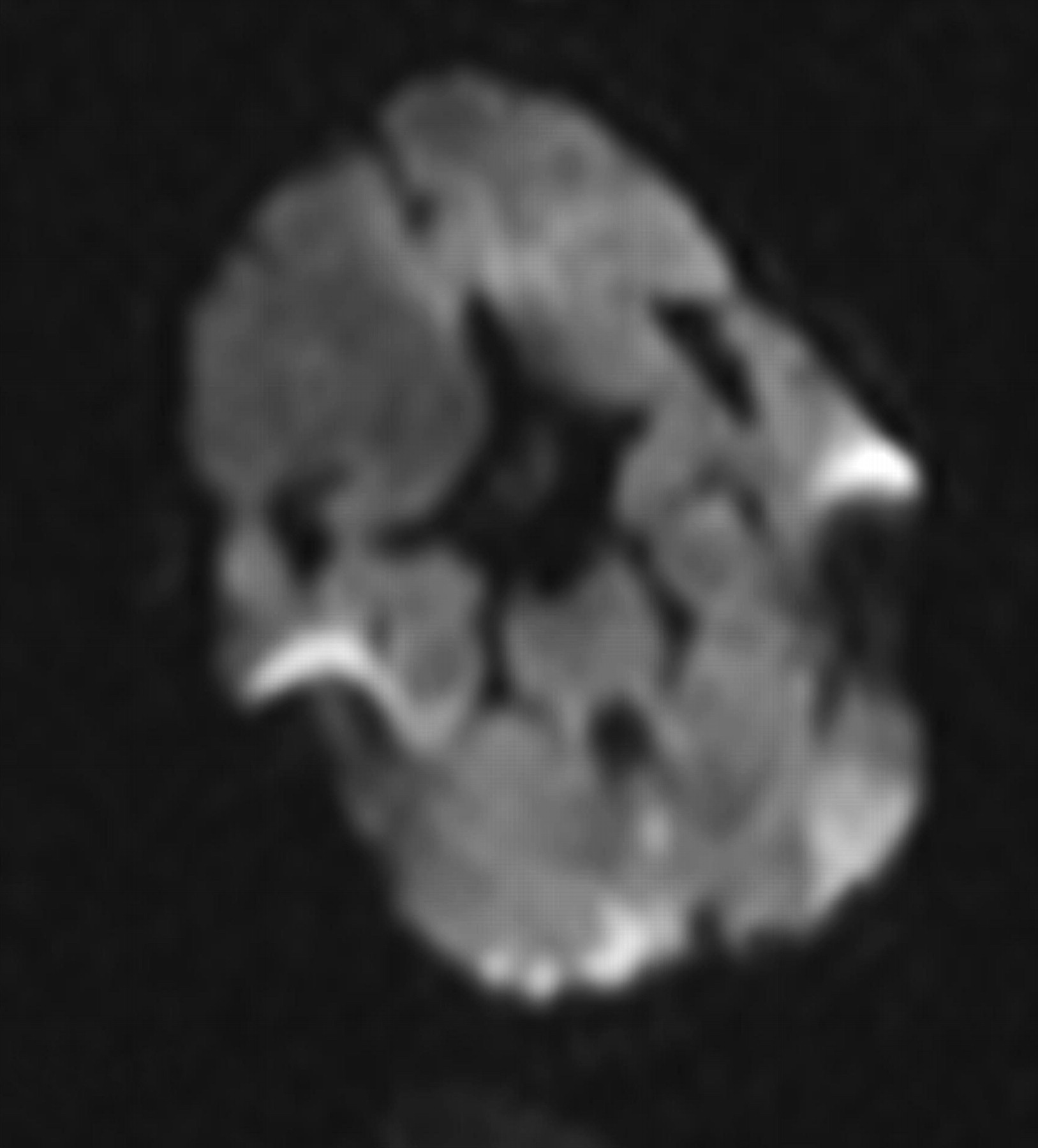
A patient with a past medical history of hypertension, diabetes mellitus type 2, hyperlipidemia and bilateral ptosis of unknown etiology (s/p surgical correction) presented with complaints of intermittent double vision, bilateral eye pain and new onset of mild frontal and temporal headache for 2 months. On admission, laboratory tests were unremarkable except for an erythrocyte sedimentation rate of 42 mm/h and a C reactive protein level of 4 mg/l. An extensive workup, including MRI and MR angiography (MRA) of the head was unremarkable. The patient was diagnosed with ocular myasthenia gravis and was treated with oral prednisone and pyridistigmine. Two months later the patient was admitted for vertical diplopia, headache, lightheadedness and gait imbalance. The patient had tenderness in the bilateral temporal regions. Laboratory tests were consistent with serum sodium of 125 mEq/l, erythrocyte sedimentation rate of 51 mm/h and C reactive protein of 28 mg/l. MRI of the brain was consistent with bilateral acute cerebellar infarctions (figure 1). MRA of the head and neck showed complete occlusion of the left vertebral artery at the V3–V4 junction. There was a high grade stenosis of the right vertebral artery at the V3–V4 junction. There was irregularity throughout the course of the bilateral vertebral arteries. The patient underwent bilateral temporal artery biopsy which showed inflammatory infiltrates, consisting of multinucleate giant cells and lymphocytes in the elastic lamina, consistent with GCA. Diagnostic cerebral angiography revealed high grade (up to 80%) stenosis of the right vertebral artery secondary to vasculitis/arteritis. The patient was treated with pulse dose steroid therapy (solumedrol 1 g intravenous for 3 days) followed by oral prednisone (50 mg daily). The patient was discharged in a stable condition to a rehabilitation center.
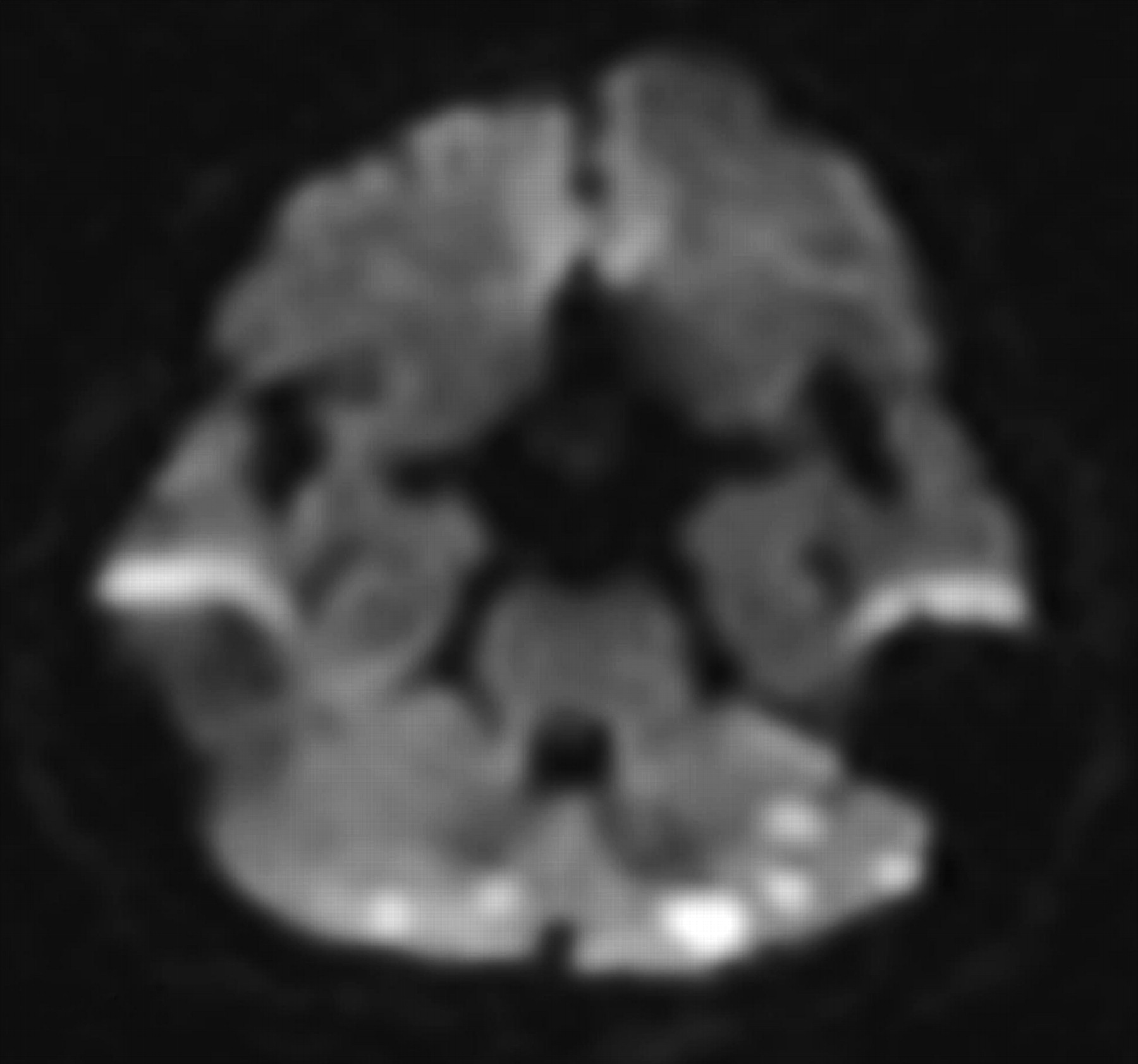
MRI diffusion weighted imaging, showing bilateral cerebellar infarctions.
Three weeks later, the patient presented with worsening balance and a fall. MRI of the head showed progression of cerebellar infarctions (figure 2). MRA showed complete occlusion of the bilateral vertebral arteries. The patient was started on azathioprine (50 mg daily) and prednisone (50 mg daily) was continued.
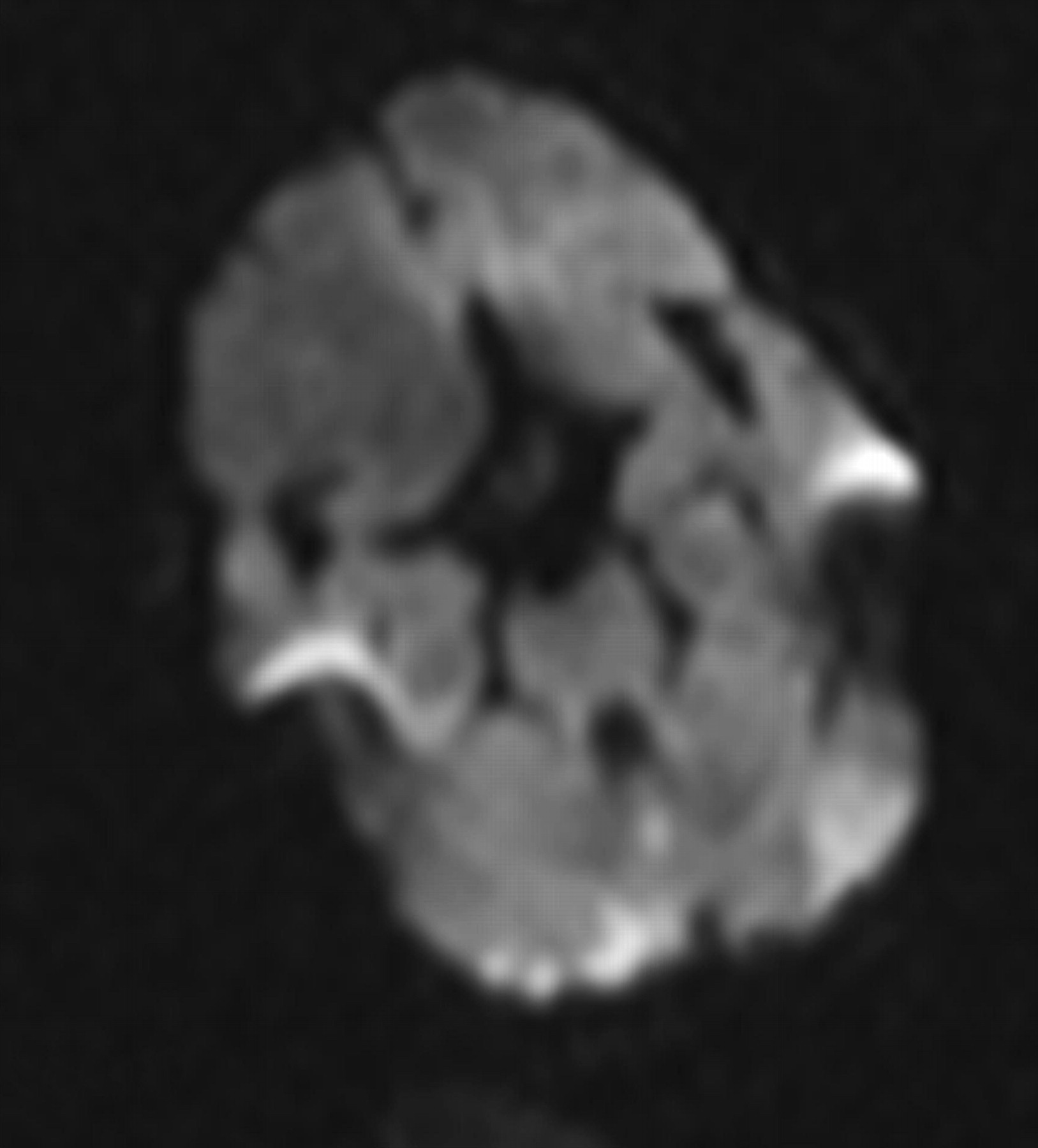
MRI diffusion weighted imaging, 3 weeks apart, demonstrating progression of bilateral cerebellar infarctions.
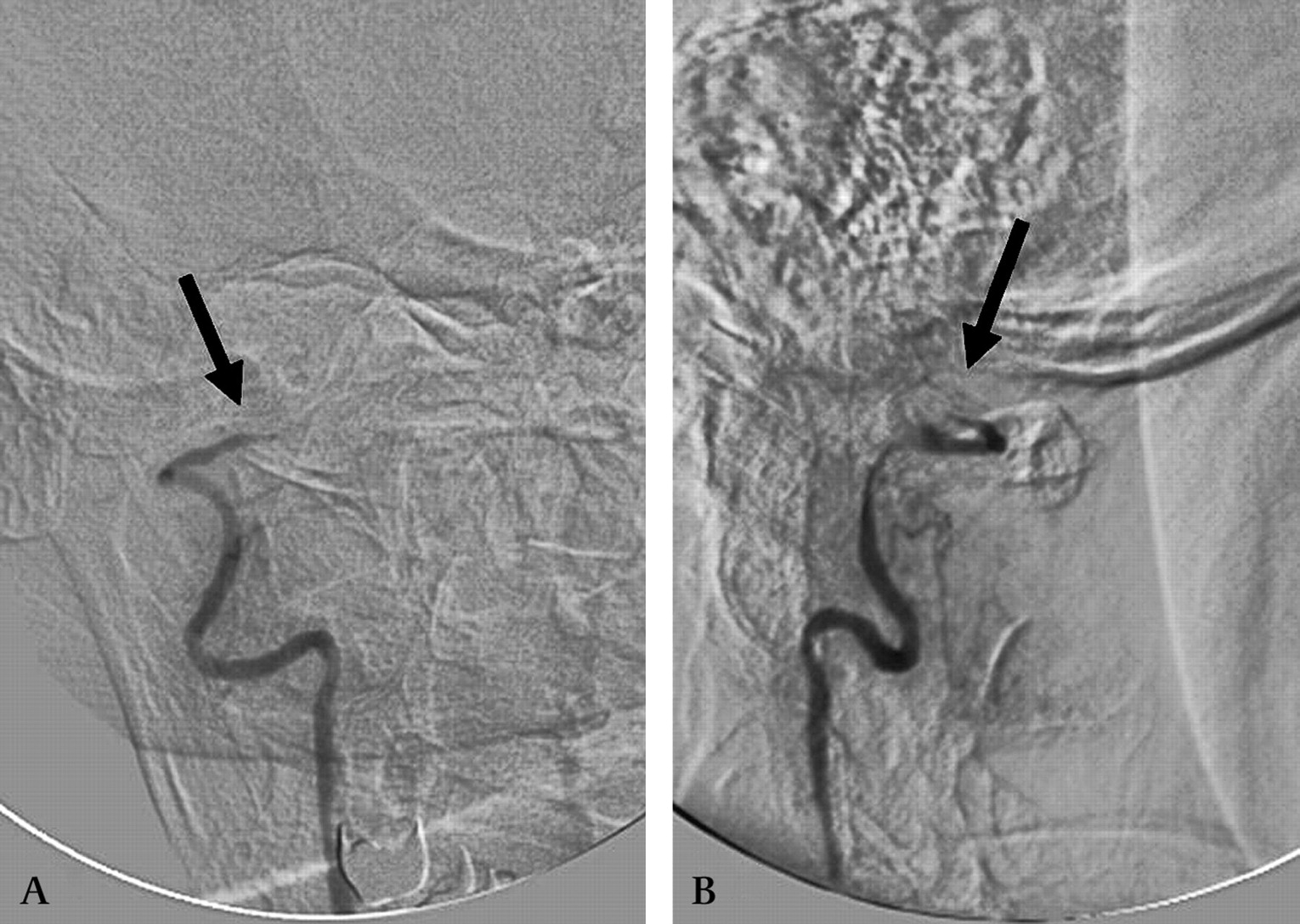
The patient underwent cerebral angiography which confirmed the findings of the MRA (figure 3A,B). In addition, angiography also demonstrated retrograde filling of the basilar artery up to the mid-segment from the bilateral posterior communicating arteries (figure 4). Within 24 h, the patient developed an acute onset of dysarthria, left facial droop and left hemiplegia (National Institutes of Health Stroke Scale 13). Systolic blood pressure was 120–130 mm Hg. Blood pressure was then induced up to 180 mm Hg, which stabilized her symptoms. Clopidogrel (Plavix) 300 mg and aspirin 325 mg were given.

(A) Anteroposterior view of the right vertebral artery. There is complete occlusion of the distal right vertebral artery (arrow) before the origin of the right posterior inferior cerebellar artery with no filling of the basilar artery. (B) A lateral view of the right vertebral artery. There is complete occlusion of the distal right vertebral artery (arrow).
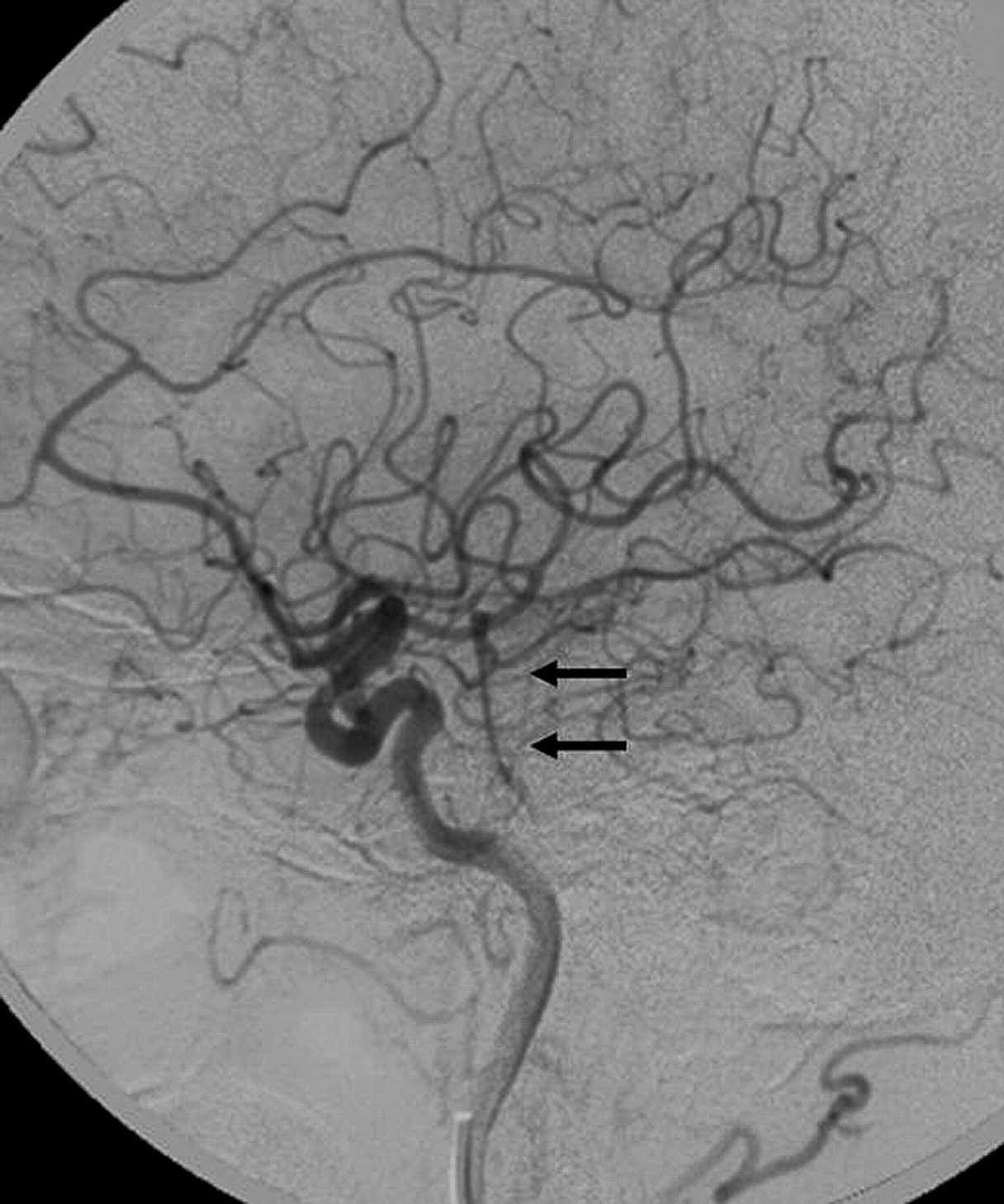
A lateral projection of the left internal carotid artery. There is normal filling of the anterior circulation with retrograde filling of the basilar artery (arrows) through the posterior communicating artery.
The patient was emergently taken to the angiography suite to revascularize the occluded segment. A femoral approach was used and by using a micro puncture needle, access was achieved through the right femoral artery. A 6 French sheath was placed, and through the sheath, a 6 French Envoy guide catheter (Cordis Endovascular, Miami Lakes, Florida, USA) was advanced and positioned at the origin of the right vertebral artery. Through the guide catheter, an Excelsior SL-10 microcatheter (Boston Scientific, Natick, Massachusetts, USA) was first advanced over a Transcend 0.014 inch microwire (Boston Scientific) and then over a Synchro 2, 0.014 inch microwire (Boston Scientfic). There was difficulty in crossing the occlusion through the microwire, the wire was removed and through the microcatheter nicardipine 2 mg (Cardene; PDL Pharma, Nevada, USA) was infused. An attempt was made to pass the microwire again through the occlusion and this time the wire passed successfully. The microcatheter was then advanced and positioned in the left posterior cerebral artery. A Synchro 2, 0.014 inch exchange length microwire was then advanced and positioned in the posterior cerebral artery. The microcatheter was then exchanged for a Gateway 1.5 mm×9 mm (Boston Scientific) angioplasty balloon which was placed across the V3–V4 junction of the vertebral artery and inflated at two different points. Post-angioplasty angiographic images demonstrated recanalization of the vertebral artery. The balloon catheter was then removed and a Wingspan 3 mm×20 mm stent (Boston Scientific) was positioned and deployed. Because of the irregularity noted not only in the V3–V4 segment but also there was progressive narrowing in the V2 and V1 segment, a second Wingspan stent 3.5 mm×20 mm stent was placed in the V2–V3 junction and deployed. A third Wingspan stent 4.0 mm×20 mm was positioned in the V2 segment and deployed. A final Wingspan stent 4.5 mm×15 mm was deployed at the origin of the vertebral artery. Multiple injections after deployment of the stent showed the patency of the stent (figure 5A,B). The patient had significant improvement of neurological symptoms within 3 days after the procedure and continued to improve during hospitalization. The patient was started on cyclophosphamide, and azathioprine was discontinued. The patient's neurological examination after 1 month showed antigravity strength in the left upper and lower extremities, normal sensory examination and mild dysarthia (National Institutes of Health Stroke Scale 3). CT scan of the head demonstrated a small right pontine infarction and stable bilateral cerebellar infarctions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Anteroposterior view of the right vertebral artery after angioplasty and stent placement at the distal right vertebral artery (arrows). (B) Anteroposterior view of the right vertebral artery after stent placement along the course of the vertebral artery.
Discussion
GCA is the most common form of systemic vasculitis in adults.11 The incidence of GCA varies widely in different populations, from less than 0.1 per 100 000 to 33 per 100 000 persons aged 50 years and older.12–14 It is an inflammatory disease of large and medium sized arteries that affects the internal elastic lamina through activation of CD4+ Th cells to an unknown antigen. It has tropism to arteries with well developed elastic membrane.6 Most commonly it affects the aorta and its main extracranial branches but in some cases it affects intracranial arteries, such as vertebral, basilar and anterior cerebral arteries.14 Intracranial vasculitis, responsible for acute ischemic stroke in patients with GCA, most commonly presents as vertebral artery narrowing and occasionally complete occlusion. The inflammatory process mostly involves the extradural part of the vertebral artery (V2–V3 segment) but there have been a few case reports of involvement of intradural portion (V3–V4 junction).4 5
Even though corticosteroid and immunosuppressive therapies, such as methotrexate, are the mainstay of treatment of GCA, cerebral arteritis has been reported to be refractory to medical therapy in most cases. Out of eight cases found in the literature, only two had a favorable outcome.2 3 Endovascular treatment is not widely used to relieve the symptoms associated with vasculitis in GCA. Angioplasty has been successfully used only as an alternative treatment in the management of ischemic complications secondary to axillary arteritis in two patients with GCA9 10; both had a favorable outcome.
We report the second known case of angioplasty and stent placement for the treatment of vertebral artery occlusion in a patient with GCA. Our patient developed complete occlusion of the bilateral vertebral arteries with cerebellar infarction despite being on aggressive medical treatment which improved after balloon angioplasty and stent placement. The first reported case demonstrated the utilization of endovascular therapy for pre-occlusive internal carotid artery stenosis.8 There are two cases reported of vasculitis secondary to GCA in which angioplasty and stenting were utilized to treat refractory limb ischemic symptoms. In the first case, balloon angioplasty of the axillary artery was performed to relieve ischemic symptoms in the upper extremities.9 In the second case, balloon angioplasty of the superior mesenteric artery relieved the symptoms of abdominal angina that were persistent after prednisone and cyclophosphamide treatment.10 Acute ischemic events secondary to vertebral artery stenosis/occlusion have been reported in 3–4% of patients with GCA.3 5 In most cases, GCA involving the vertebral arteries has been refractory to medical treatment and has had a fatal outcome. Endovascular intracranial angioplasty and stent placement is a potential alternative treatment option in such cases.
Conclusion
Endovascular intracranial angioplasty and stent placement is an alternative method of treatment for ischemic cerebral complications secondary to GCA involving the vertebral arteries refractory to medical treatment.
References
Footnotes
Competing interests None.
Patient consent Not obtained.
Provenance and peer review Not commissioned; externally peer reviewed.