
Abstract
Study design:
Survey.
Objectives:
Insight in (1) the changes in participation in vocational and leisure activities and (2) satisfaction with the current participation level of people with spinal cord injuries (SCIs) after reintegration in society.
Design:
Descriptive analysis of data from a questionnaire.
Setting:
Rehabilitation centre with special department for patients with SCIs, Groningen, The Netherlands.
Subjects:
A total of 57 patients with traumatic SCI living in the community, who were admitted to the rehabilitation centre two to 12 years before the current assessment.
Main outcome measures:
Changes in participation in activities; current life satisfaction; support and unmet needs.
Results:
Participation expressed in terms of hours spent on vocational and leisure activities changed to a great extent after the SCI. This was mainly determined by a large reduction of hours spent on paid work. While 60% of the respondents successfully reintegrated in work, many changes took place in the type and extent of the job. Loss of work was partially compensated with domestic and leisure activities. Sports activities were reduced substantially. The change in participation level and compensation for the lost working hours was not significantly associated with the level of SCI-specific health problems and disabilities. As was found in other studies, most respondents were satisfied with their lives. Determinants of a negative life satisfaction several years following SCI were not easily indicated. Reduced quality of life was particularly related to an unsatisfactory work and leisure situation.
Conclusions:
Most people with SCI in this study group were able to resume work and were satisfied with their work and leisure situation.
Similar content being viewed by others

Introduction
Reintegration in work, leisure activities and sports following spinal cord injury (SCI) is considered to be an important goal of rehabilitation. Active involvement in activities and roles is strongly related to health and well being1 and a high level of social activities leads to a better quality of life.2 This study provides insight in the outcomes of vocational and leisure participation of people with SCI several years after their injury, as part of the International Classification of Functioning, Disabilities and Health (ICF).3
From a social point of view, return to work following SCI is regarded as one of the most important outcomes of reintegration in society.4, 5 It gives people a social status and meaning to life, and enables them to be financially independent. From other studies we know that the chances to resume work are restricted for patients with chronic diseases and disabilities.6, 7, 8 Working rates for people with SCI vary from 31 to 48% in recent studies.9, 10, 11, 12, 13 Factors related to the success of vocational reintegration are age, education level, realistic expectations, preinjury type of job, type of lesion and disease-specific problems and disabilities.2, 4, 9, 14, 15, 16
For those people unable to reintegrate in work, participation in nonvocational activities must also be considered as a successful rehabilitation outcome. Very few studies have described the types of postinjury activities and roles other than traditional employment.1, 3, 5, 17 The assessment of these nonvocational outcomes is more difficult, since those activities are more complex to quantify in everyday life. In a Swedish study, the majority of subjects had succeeded in finding new interests and hobbies or adapting preinjury leisure activities to the disability.2 A major shift in time use occurred from time spent on social activities to personal care activities.
Attaining an acceptable quality of life can be seen as the ultimate goal of rehabilitation. Several objective and subjective determinants of quality of life after an SCI have been studied.2, 11, 18, 19, 20, 21, 22, 23, 24 Some authors found that life satisfaction among persons with SCI is relatively good and in a few studies even better than their peers.21, 22 Other findings indicate that people with SCI who live at home report a lower level of satisfaction with life.20, 23 Satisfaction with the vocational situation is usually low.11, 20 For persons who returned to work after the SCI, this can be explained by unrewarding, poor-quality jobs.24 In our previous study on vocational reintegration, a reasonably good job satisfaction was found.14 Information about the satisfaction with nonvocational activities is rare.1, 2
To improve rehabilitation interventions aimed at a satisfactory participation, it is important to know the perspectives of job reintegration, time use and satisfaction. This study presents the changes in time use and actual reintegration in vocational and leisure activities several years after the onset of the SCI. Results of life satisfaction are described, especially regarding the vocational and leisure situation. Personal experiences are analysed regarding the support during the reintegration process.
Methods
Patients
In this study, we focused on patients with traumatic SCI, admitted at the Centre for Rehabilitation Beatrixoord from 1990 until 1998, aged 18–60 years, and living in the community. Of 89 eligible candidates, 14 patients were excluded: four patients deceased, three had serious psychiatric problems, one was discharged to a nursing home and six were foreigners with difficulties with the Dutch language. Two finished their rehabilitation programme in another rehabilitation centre and discharge data were not complete. Of four patients, addresses were not found and they were lost for follow-up. To 69 patients, a questionnaire was sent. The questionnaire was filled in and returned by 57 patients, which means a response of 83%.
The study group was divided into four subgroups with different levels of change in participation. It concerned two subgroups currently working, who either kept full-time jobs with 36 h a week or more (A), or changed to part-time jobs (B), and two subgroups without work, who succeeded (C) or failed (D) in compensating for their lost participation activities. The study group consisted six patients (11%) with complete tetraplegia (ASIA A), 17 patients (30%) with incomplete tetraplegia (ASIA B–D), 20 patients (35%) with complete paraplegia (ASIA A) and 14 (24%) with incomplete paraplegia (ASIA B–D).
Questionnaire
Data on participation and satisfaction of the participants and factors that might have influenced these outcomes were gathered using a questionnaire, which was developed for this study. Participation was defined as reintegration in vocational and leisure activities. Vocational participation consisted of activities related to paid and nonpaid work, school and housekeeping. Activities such as hobbies and sports were defined as leisure participation.
To assess the participation in activities pre- and postinjury, the Utrechtse Activiteiten Lijst was used.25 This questionnaire is a Dutch adaptation of the Craig Handicap Assessment Rating Technique,26 and assesses the time spent on activities such as work, study, voluntary work, hobbies and sports in hours per week. In addition, we asked for an estimation of the time needed for self-care in minutes pre- and postinjury.
Our questionnaire consisted of relevant parts of a questionnaire developed by TNO Arbeid (Netherlands Organisation for Applied Scientific Research) as part of the Vocational Handicap Research Programme. TNO Arbeid validated their questionnaire in several research projects and reported good reliability of the test.6, 7 The employment situation was assessed both preinjury and after reintegration. Respondents were asked to report the changes in type of job and working hours, vocational retraining, job modifications, contacts with work professionals, income and their opinion on the working conditions and social atmosphere. The TNO assessment includes an educational level scale (score 1–8). Changes in the type of hobbies and sports were also assessed, as was the support of the rehabilitation team in developing new leisure activities.
Life satisfaction was considered as a second main outcome measure and assessed by the Fugl-Meyer Life Satisfaction Questionnaire (LSQ).27 The LSQ measures general life satisfaction and satisfaction on eight life domains: self-care ability, leisure situation, vocational situation, financial situation, sexual life, partnership relations, family life and contacts with friends. The Dutch version of the scale was used, translated and validated by Post et al.11, 23 LSQ item scores range from 1 (=very dissatisfying) up to 6 (=very satisfying) and mean item scores were used. As in the work of Fugl–Meyer, the scores of the general life satisfaction were dichotomized into ‘satisfied’ (grades 5–6) and ‘not satisfied’ (grades 1–4).27, 28
Several factors were studied for their relationship to change in participation and satisfaction. A validated scale with eight health problems related to SCI was used, experienced in the last 4 weeks before assessment:21 respiratory problems, pain, spasms, contractures, excessive sweating, oedema, pressure sores and urinary tract infections. A health problem score of 0–8 was obtained by counting all the ‘yes’ answers on a two-point scale.
The TNO assessment also includes a scale regarding 18 work-related disabilities with response choices ‘able’, ‘able with difficulty’ and ‘not able’ (TNO scores 0–54) and six items regarding dependence on help with response choices ‘independent’, ‘partially dependent’ and ‘dependent’ (TNO weighted score 0–42). The ability to walk functionally with or without devices, and the level of continence for urine with or without bladder management techniques were both assessed on a three-point scale (able, able with difficulty, not able). An estimation was asked for of the time in minutes per day used for self-care pre- and postinjury and the extra time currently needed was calculated.
Systematic assessment of expectations of all patients with SCI began in 1988 in our department. It concerned expectations of patients and the team regarding functional outcome in several domains. For this study, the question about coping was selected: ‘Do you expect to cope with the handicap?’ Possible answers were ‘yes’, ‘no’ and ‘uncertain’. We used the data of the final assessment before discharge from the rehabilitation centre.
Analysis
Descriptive statistics were performed using the Statistical package for social sciences (SPSS) version 10.0. The hours spent on several vocational and leisure activities before the SCI and at the moment of assessment were compared with a paired t-test. Analysis of variance and multiple comparisons with Bonferroni corrections were used to compare the subgroups with different levels of change in participation.
Differences between satisfied and not satisfied groups regarding satisfaction on eight life domains were tested using independent sample t-test. Regarding personal, SCI-specific and work-related variables, the differences were tested using a logistic regression analysis and presented by odds ratios. The significance level was chosen as P<0.05.
Results
The study group of 57 respondents consisted of 52 male (91%) and five female subjects. Their age at the moment of the SCI ranged from 18 to 59 years with a mean of 33 years (SD 11). The time elapsed since injury varied from 29 to 140 months with a mean of 84 months (SD 29). A total of 23 SCIs (40%) were caused by traffic accidents, 13 (23%) by industrial accidents and 21 (37%) by sports and private accidents.
The group of patients who returned the questionnaire (n=57) was compared to the group who gave no response (n=12). There were no significant differences regarding age, gender and type of SCI. The most remarkable difference between the group of respondents and nonrespondents was the percentage of patients working preinjury. In the group of respondents, 49 (86%) worked at the moment of SCI versus 5 (42%) in the group of nonresponders. In the group of nonresponders, the time elapsed since the SCI was on average longer than in the group of responders.
Changes in participation
The results on the Utrechtse activiteitenlijst preinjury and now are presented in Table 1. Hours spent on paid work form a substantial part of the total time use. The most remarkable change was found in the average working hours with a decrease of more than 20 h a week. Hours spent on sports also significantly diminished. The total vocational and leisure participation of the study group was reduced by 40%. The variance in time use after the SCI was more pronounced than preinjury. Significantly more time was spent on self-care activities, which changed from about half an hour a day preinjury to a mean of 70 min a day.
At the time of injury, 49 of the 57 respondents (86%) had a job and most of them worked fulltime (median 40 h/week). In all, 30% were self-employed and worked on average 60 h a week. Five persons (male), with a mean age of 21 years, went to school. Three persons (male) were out of work for a long time. Of the group of 49 preinjury workers, 33 (67%) successfully returned to paid work. Four persons stopped working several years later. Of 29 workers, 18 (62%) currently worked fewer hours than before the SCI. The group that changed to a different employer lost the least number of working hours. All five students graduated in the mean time, so study hours diminished on the whole. Two respondents were currently active in vocational training. At the assessment 34 respondents (60%) had a job, including 29 preinjury working persons and all five students. The number of persons doing voluntary work did not change, but the time they spent on it slightly increased.
Most of the respondents needed help with domestic activities after the SCI, at least partially, and especially with heavy work and shopping. However, one-third of the study group spent more hours on housekeeping than preinjury and 17 respondents became active in a role as homemaker for more than 8 h a week, versus 13 preinjury. A total of 72% of respondents reported loss of hobbies. Handicraft and several kinds of sports like football, skating and cycling were mentioned most often. About half of the study population found new hobbies, varying from personal computer activities and archery to hobbies adapted to the handicap, such as wheelchair dancing or wheeling. A total of 21 persons (37%) were currently active in sports versus 60% prior to the injury, with a mean of 3 h per week now versus 5 h preinjury. Two-thirds participated in types of sports different from those they had been involved in prior to their injury.
Factors related to changes in participation
Respondents in subgroup A (n=18) with full-time jobs currently worked on average 45 h a week (SD 10, range 36–70), and worked on average 51 h (SD 21) a week preinjury. Persons in subgroup B (n=16) with part-time jobs worked on average 17 h (SD 9, range 4–35) versus 46 h (SD 13) preinjury. The total hours spent on vocational and leisure activities per week hardly changed in subgroup A: from an average of 67 (SD 16) to 63 h (SD 14) a week. However, it was halved in subgroup B: from an average of 63 (SD 9) to 33 (SD 17) hours a week. Persons in subgroup C (n=10) compensated their lost working hours with one or more specific other activities, like significant involvement in the housekeeping, leisure activities or voluntary work. They currently spent a mean of 38 h (SD 12) on participation activities a week versus 75 h (SD 13) preinjury. Respondents in subgroup D (n=13) lost participation in all activities and were active for 16 h (SD 15) a week versus 60 h (SD 29) preinjury. The proportion of leisure hours of the total hours spent on vocational and leisure activities of subgroups A–D was, respectively, 12, 25, 32 and 44%.
Comparison of the subgroups regarding several personal and SCI-related variables is shown in Table 2. The level of change in participation was not associated with any variable other than age (F=3.3, P<0.05). Full-time workers (A) were significantly younger than those who compensated for their lost jobs (C).
Satisfaction with the vocational and leisure situation
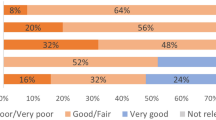
A total of 38 respondents (67%) reported being ‘satisfied’ (grades 5 and 6) with their lives in general, according to the LSQ. Retrospectively, seven (18%) of those 38 satisfied respondents were even more satisfied than before the SCI. All 19 respondents who were ‘not satisfied’ with their lives (grades 1–4) experienced a decline of satisfaction in comparison with preinjury. For details regarding satisfaction within the different domains according to the LSQ see Table 3.
Leisure situation and social roles showed the highest mean item scores of satisfaction. Comparison of the subgroups with persons who were satisfied and not satisfied with their lives (t-test for groups) revealed a significantly lower satisfaction with the work and leisure situation of the dissatisfied group. Of 19 respondents less satisfied with their life, 14 (74%) had a dissatisfying work of leisure situation, and nine (47%) were less satisfied with both their vocational and leisure participation. The level of change in participation was associated with satisfaction with the vocational situation (F=9.4, P<0.05). Multiple comparisons showed that participants in subgroup C were significantly less satisfied with the vocational situation. Satisfaction with the leisure situation (F=0.8, P=0.501) and general life satisfaction (F=0.6, P=0.643) did not show any difference between the subgroups.
Factors related to life satisfaction
For indicators of life satisfaction, see Table 4. At discharge from the rehabilitation centre, 81% of the patients expected to learn to cope with their physical limitations. Significant indicators of life satisfaction were not found. Being employed was not associated with more general life satisfaction.
Support and unmet needs
Information about the support and professional interventions during the rehabilitation process and the period thereafter was collected. In total, 16 persons (28%) reported help from the rehabilitation team in finding new hobbies or sports. The occupational therapist, physical therapist and leisure therapist were the main professionals who supported the uptake of new leisure activities. Most vocational reintegration activities took place after the rehabilitation period. Of those 49 with a job preinjury, 16 respondents (33%) reported participation in vocational retraining. In all, 13 (81%) of them were satisfied with the training. Of the 34 working respondents, 13 (38%) returned to paid work without supplementary benefits and 62% worked with benefit from the Dutch Work Disability Act (WDA). The respondents not working at the time of assessment all received social security benefits, most of them full benefit from the WDA.
In 74% of the 34 present work situations, job modifications took place. Adaptations included personal aids and adapted furniture or toilet facilities. Personal time management (planning your own working day) was often mentioned. Half of the working respondents recently had contacts with professionals regarding their health at work. Three of them still received support from the rehabilitation team. In total, 14 respondents (25%) reported wanting more contacts with reintegration professionals, and half of them needed more support from the rehabilitation team. The 19 persons, who judged the quality of life as dissatisfying, reported relatively more unmet needs regarding retraining, job modifications and contacts with reintegration professionals than the satisfied respondents.
Discussion
The most important goal of rehabilitation is enabling disabled persons to return to independent and satisfactory lives in their community. In order to provide successful rehabilitation programmes based on realistic goals, insight is needed in outcome of participation and satisfaction following SCI. Most participants were able to return to work or to compensate the time formerly spent on work with other activities. Their participation level, expressed in terms of hours spent on vocational and leisure activities, changed to a great extent following SCI, which is mainly explained by reduction of working hours. Most respondents were satisfied with their lives. However, a reduced quality of life was particularly associated with an unsatisfactory vocational and leisure situation and more unmet needs regarding support from reintegration professionals. Attention to participation issues has the potential to improve life satisfaction following SCI.
The cohort under study completed a standard multidisciplinary rehabilitation programme including education, training and counseling, based on goals set by the rehabilitation team in agreement with the patient.29 In comparing the study with other research on this subject, a high standard of care and support in the Netherlands has to be taken into account. The results are based on patient report, which make them obviously subjective. Owing to the small numbers, we included all types of SCI. Some factors might have flattered the results of the study group: the small group of nonrespondents had less vocational potential preinjury, and patients who did not speak Dutch were excluded. A limitation of the study is that socioeconomic and cultural differences within the Netherlands were not analysed.
Nearly 60% of our study population was working at the time of assessment, which is higher than in comparable studies carried out in the last decade.9, 10, 11, 12, 13 Preceding their SCI, this study group was very active and spent on average more than 40 working hours a week preinjury. It concerned a relatively high number of self-employed workers and persons who extended their regular jobs with jobs on the side in evening hours. Increasing the proportion of persons in gainful employment seems the most realistic option to maximize the participation outcome in terms of hours spent on activities and further financial independence. Important interventions aimed at a successful reintegration in work are promoting the behavioural repertoire of the patient and creating participation opportunities.30
Regarding the hours spent on work, we found a reduction of more than 50% in comparison with preinjury hours. The least reduction of working hours was found if the subjects changed to other jobs that better match with their capabilities. To prevent large decreases in working hours, it is essential to create opportunities for jobs that fit with physical capabilities and personal needs. As was expected from literature, the participation in sports diminished significantly.31 On average twice as much more time was spent on self-care. Only an additional 40 min a day were reported, which seems of little clinical relevance. However, it is good to realize that people with SCI generally need a lot of time for self-care on several planned and unplanned points in time. The extra time that is needed for all inconveniences outdoors due to the continence problems and reduced mobility is usually underestimated.
Comparison of respondents with full-time jobs (A) and part-time jobs (B) showed remarkable variation in the extent of changes in participation. The loss of total participation hours of part-time workers is not only explained by the reduction of their working hours. Some of the part-time workers make every effort to keep at work for social and personal reasons, even if this leads to substantial loss of other activities. Some of those who failed to reintegrate in work compensated the time formerly spent on work with various other activities. A few of them changed roles with their partners and became homemakers instead of breadwinners. Others expanded their activities to voluntary work. SCI-specific factors were not associated with these different outcomes, which is an interesting finding. More studies are needed to analyse the role of coping and motivation.
As in other studies on the quality of life among persons with chronic disabilities, most participants were satisfied with their lives.21, 22 Life satisfaction is considered to embody an assessment of life as a whole, based on how well personal goals match with personal achievement.19 Adjustment to the consequences of SCI is an immense, complex procedure and considerable research effort has been made to assess those factors associated with good or bad adjustment.18, 19, 21
Comparison of the results of life satisfaction in our study with those of Post et al23 is summarized in Table 5. As standard deviations were lacking in their publication, it was not possible to compare the studies statistically. A large proportion of our study group was particularly satisfied with their leisure situation and succeeded in adapting preinjury leisure activities to the disability or finding new hobbies. Unlike other studies,20, 23 the mean satisfaction with the vocational situation in this study was also relatively good and comparable with the Dutch reference group of Post, contrary to his findings. An explanation for this is not easily given. There were little differences between the study populations regarding age, type of SCI and years postinjury. Socioeconomic and cultural differences may play a role, but analysis regarding these factors was not possible.
Life satisfaction in this study was not associated with being employed. This illustrates that most people with SCI gradually adjust to a situation without paid work. However, it was remarkable to find that the subgroup that was less satisfied with life in general was particularly dissatisfied with their vocational and leisure situation. Other factors related to satisfaction were not easily identified. A larger study is needed to further test the trends regarding SCI-related pain and educational level.
A substantial number of patients wished more contacts with reintegration professionals. Participation issues deserve more priority during follow-up of the multidisciplinary rehabilitation team. Ongoing stimulation and support in creating participation opportunities for people with SCI is needed to ameliorate this important aspect of quality life. When it becomes clear that reintegration in work fails, a renewed attempt at creating leisure opportunities should be made, even if this is several years after the initial rehabilitation period. For some patients, it can be too premature to focus on participation during the rehabilitation period, due to a delayed or postponed coping and acceptance process.
In terms of future research, more qualitative studies are needed regarding the process of reintegration in society, which give more information with respect to the role of more subjective factors associated with changes in participation and satisfaction, such as coping abilities, psychosocial factors, support from family and professionals, etc. In-depth interviews with all persons involved can reveal which interventions are best to promote adequate skills and create opportunities for participation, and in which phase they are most effective.
Conclusions
Within the Dutch population it has been found that the majority of people with SCI are able to resume work, and are satisfied with their work and leisure situation. However, extensive reduction of working hours takes place, which is partially compensated for with significant involvement in the housekeeping, leisure activities or voluntary work. Long-term follow-up by the rehabilitation team is recommended to evaluate participation and satisfaction. Rehabilitation interventions should be made available even a long time after the SCI.
References
Pentland W, Harvery AS, Smith T, Walker J . The impact of spinal cord injury on men's time use. Spinal Cord 1999; 37: 786–792.
Siösteen A, Lundqvist C, Blomstrand C, Sullivan L, Sullivan M . The quality of life of three functional spinal cord injury subgroups in a Swedish community. Paraplegia 1990; 28: 476–488.
ICF. International Classification of Functioning, Disability and Health: World Health Organisation: Geneva 1999.
Krause JS . Employment after spinal cord injury. Arch Phys Med Rehabil 1992; 73: 163–169.
Noreau L, Dion S-A, Vachon J, Gervais M, Laramée M-T . Productivity outcomes of individuals with spinal cord. Spinal Cord 1999; 37: 730–736.
Andries F et al. Vocational perspectives and neuromuscular disorders. Int J Rehab Res 1997; 20: 255–273.
Wevers CWJ, Brouwer OF, Padberg GW, Nijboer ID . Job perspectives in facioscapulohumeral muscular dystrophy. Disab Rehab 1993; 15: 24–28.
Schoppen T, Boonstra AM, Groothoff JW, de Vries J, Göeken LNH, Eisma WH . Employment status, job characteristics and work related health experience of people with lower limb amputation in the Netherlands. Arch Phys Med Rehabil 2001; 82: 239–245.
Murphy G, Brown D, Athanasou J, Foreman P, Young A . Labour force participation and employment among a sample of Australian patients with spinal cord injury. Spinal Cord 1997; 35: 238–244.
Berghammer A, Gramm M, Vogler L, Schmitt-Dannert H-H . Investigation of the social status of paraplegic individuals after medical rehabilitation. Spinal Cord 1997; 35: 493–497.
Post MWM, de Witte LP, van Asbeck FWA, van Dijk AJ, Schrijvers AJP . Predictors of health status and life satisfaction in spinal cord injury. Arch Phys Med Rehabil 1998; 78: 395–402.
Conroy L, McKenna K . Vocational outcome following spinal cord injury. Spinal Cord 1999; 37: 624–633.
Tomassen PCD, Post MWM, van Asbeck FWA . Return to work after spinal cord injury. Spinal Cord 2000; 38: 51–55.
Schönherr MC, Groothoff JW, Mulder GA, Eisma WH . Vocational reintegration following spinal cord injury: expectations, participation and satisfaction. Spinal Cord 2004; 42: 177–184.
DeJong G, Branch LG, Corcoran PJ . Independent living outcomes in spinal cord injury: multivariate analyses. Arch Phys Med Rehabil 1984; 65: 66–73.
DeVivo MJ, Rutt RD, Stover SL, Fine PR . Employment after spinal cord injury. Arch Phys Med Rehabil 1987; 68: 494–498.
Levi R, Hultling C, Seiger A . The Stockholm spinal cord injury study: 4. Psycho-social and financial issues of the Swedish annual level-of-living survey in SCI subjects and controls. Paraplegia 1996; 34: 152–157.
Taricco M et al. The social and vocational outcome of spinal cord injury patients. Paraplegia 1992; 30: 214–219.
Glass CE, Jackson HF, Dutton J, Charlifue S, Orritt C . Estimating social adjustment following spinal trauma – l: who is more realistic – patient or spouse? A statistical justification. Spinal Cord 1997; 35: 320–325.
Fuhrer MJ, Rintala DH, Hart KA, Clearman R, Young ME . Relationship of life satisfaction to impairment, disability, and handicap among persons with spinal cord injury living on the community. Arch Phys Med Rehabil 1992; 73: 552–557.
Cushman LA . Spinal cord injury: 10 and 15 years after. Paraplegia 1992; 30: 690–696.
Eisenberg MG, Saltz CC . Quality of life among aging spinal cord injured persons: long term rehabilitation outcomes. Paraplegia 1991; 29: 514–520.
Post MWM, van Dijk AJ, van Asbeck FWA, Schrijvers AJP . Life satisfaction of persons with spinal cord injury compared to a population group. Scand J Rehab Med 1998; 30: 23–30.
Clayton KS, Chubon RA . Factors associated with the quality of life of long-term spinal cord injured persons. Arch Phys Med Rehabil 1994; 75: 633–638.
Post MWM . Utrechtse Activiteitenlijst. In: van Asbeck FWA (ed). Handboek dwarslaesierevalidatie. Bohn, Stafleu & Van Longhum: Houten/Diegum 1998 pp 356–357.
Whiteneck GG et al. Quantifying handicap: a new measure of long-term rehabilitation outcomes. Arch Phys Med Rehabil 1992; 73: 519–526.
Fugl-Meyer AR, Branholm I-B, Fugl-Meyer KS . Happiness and domain-specific life satisfaction in adult Northern Swedes. Clin Rehabil 1991; 5: 25–35.
Bränholm I-B, Eklund M, Fugl-Meyer KS, Fugl-Meyer AR . On work and life satisfaction. J Rehab Sci 1991; 4: 29.
Wade DT . Evidence relating to goal planning in rehabilitation. Clin Rehabil 1998; 12: 273–275.
Wade DT . A framework for considering rehabilitation interventions. Clin Rehabil 1998; 12: 363–368.
Tasiemski T, Bergström E, Savic G, Gardner BP . Sports, recreation and employment following spinal cord injury – a pilot study. Spinal Cord 2000; 38: 173–184.
Acknowledgements
We acknowledge Frank Andries of TNO for the use of the questionnaire developed as part of the Vocational Handicap Research Programme. We thank Roy Stewart for his assistance in the statistical analysis.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Schönherr, M., Groothoff, J., Mulder, G. et al. Participation and satisfaction after spinal cord injury: results of a vocational and leisure outcome study. Spinal Cord 43, 241–248 (2005). https://doi.org/10.1038/sj.sc.3101683
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101683
Keywords
This article is cited by
-
Work, Leisure, and Life Satisfaction for Employees with Physical Disabilities in South Korea
Applied Research in Quality of Life (2022)
-
BCI system with lower-limb robot improves rehabilitation in spinal cord injury patients through short-term training: a pilot study
Cognitive Neurodynamics (2022)
-
Improving quality of life after spinal cord injury in India with telehealth
Spinal Cord Series and Cases (2019)
-
Associations between time since onset of injury and participation in Dutch people with long-term spinal cord injury
Spinal Cord (2018)
-
Impact of health problems secondary to SCI one and five years after first inpatient rehabilitation
Spinal Cord (2017)
